Article Text

Abstract
Objectives To examine the association between blood-brain barrier (BBB) integrity, brain volume and cognitive dysfunction in adult patients with systemic lupus erythematosus (SLE).
Methods A total of 65 ambulatory patients with SLE and 9 healthy controls underwent dynamic contrast-enhanced MRI scanning, for quantitative assessment of BBB permeability. Volumetric data were extracted using the VolBrain pipeline. Global cognitive function was evaluated using a screening battery consisting of tasks falling into five broad cognitive domains, and was compared between patients with normal versus extensive BBB leakage.
Results Patients with SLE had significantly higher levels of BBB leakage compared with controls (p=0.04). Extensive BBB leakage (affecting over >9% of brain volume) was identified only in patients with SLE (16/65; 24.6%), who also had smaller right and left cerebral grey matter volumes compared with controls (p=0.04). Extensive BBB leakage was associated with lower global cognitive scores (p=0.02), and with the presence of impairment on one or more cognitive tasks (p=0.01).
Conclusion Our findings provide evidence for a link between extensive BBB leakage and changes in both brain structure and cognitive function in patients with SLE. Future studies should investigate the mechanisms underlying BBB-mediated cognitive impairment, validate the diagnostic utility of BBB imaging, and determine the potential of targeting the BBB as a therapeutic strategy in patients with SLE.
- systemic lupus erythematosus
- magnetic resonance imaging
- autoimmunity
- Blood-brain barrier
- cognitive impairment
Statistics from Altmetric.com
- systemic lupus erythematosus
- magnetic resonance imaging
- autoimmunity
- Blood-brain barrier
- cognitive impairment
Key messages
What is already known about this subject?
Cognitive impairment is the most frequent manifestation of neuropsychiatric systemic lupus erythematosus (SLE), yet the mechanisms underlying it remain poorly understood.
What does this study add?
Our findings implicate the blood-brain barrier (BBB) in the pathogenesis of cognitive dysfunction in patients with SLE (n=65).
Using dynamic contrast-enhanced MRI, extensive BBB leakage was identified in a quarter of patients with SLE and in none of the healthy controls.
SLE patients with extensive BBB leakage had smaller grey matter volumes and impaired cognitive function, compared to SLE patients with normal BBB function.
How might this impact on clinical practice or future developments?
Our findings highlight the role of the BBB in SLE-associated cognitive impairment, and call for future studies to examine the potential of treatments targeting BBB dysfunction.
Our study further suggests that BBB imaging may serve as a mechanism-specific biomarker for cognitive impairment in SLE.
Introduction
Cognitive impairment is the most commonly reported and most widely studied manifestation of neuropsychiatric systemic lupus erythematosus (NPSLE),1–4 yet its causality remains incompletely understood. Disease mechanisms implicated in NPSLE include thrombotic cerebrovascular ischaemia, brain-reactive autoantibodies and complement activation.3 These pathways may also damage the blood-brain barrier (BBB), and thereby expose the brain to neurotoxic blood components that are normally restricted from entering the brain by the BBB. In animal models, extravasation of plasma proteins (such as albumin, thrombin and activated protein C) and lupus autoantibodies into brain tissue causes neuroinflammation and neurodegeneration.5–9 Recent evidence also suggests that autoimmune antibodies and cytokines can themselves alter the normal function of endothelial cells, breaching the BBB and infiltrating the brain.10 11
Despite a strong rationale for BBB dysfunction playing a role in the pathogenesis of NPSLE,12 13 evidence in patients with SLE remains scarce and largely circumstantial (eg, postmortem findings of vascular lesions14). Technical advances in neuroimaging offer a direct, quantitative and detailed method for BBB assessment.15 Specifically, the use of dynamic contrast-enhanced MRI (DCE-MRI) allows quantification of contrast extravasation into brain parenchyma, and calculation of cross-BBB leakage rates for every voxel of the brain.16–18 While DCE-MRI has been validated in conditions associated with BBB dysfunction (eg, multiple sclerosis,19 stroke,20 traumatic brain injury18 and dementia21), it has not been well studied in NPSLE.22 Our objective was to measure BBB permeability in a large, unselected adult population of patients with SLE, and to examine associations with brain volume and cognitive function.
Patients and methods
Patients
Patients fulfilling the revised American College of Rheumatology (ACR) criteria for SLE23 were consecutively recruited from the Dalhousie Lupus Clinic, Division of Rheumatology, Queen Elizabeth II Health Sciences Center, Halifax, Nova Scotia, Canada. All patients were invited to participate unless there were contraindications to contrast-enhanced MRI scanning. Patients were not prescreened for cognitive impairment prior to study enrolment. Controls were healthy individuals with no neuropsychiatric (NP) history, consecutively recruited for another study.24 For the present study, additional exclusion criteria were significant chronic illness (eg, SLE, diabetes); and age under 35 or over 70 years old. This research was planned without patient involvement.
Demographic and clinical data, disease activity (Systemic Lupus Erythematosus Disease Activity Index-2000 (SLEDAI-2K))25 and cumulative organ damage (Systemic Lupus International Collaborating Clinics/ACR Damage Index (SDI)26) were recorded (table 1). Other variables included: lupus-related medications such as corticosteroids, antimalarials, immunosuppressive drugs (methotrexate, azathioprine, cyclophosphamide, leflunomide, mycophenolate mofetil and intravenous gamma globulin) and biological agents (rituximab or belimumab); use of psychoactive medications; lifestyle habits and comorbidities (cigarette smoking, diabetes mellitus and hypertension). Laboratory variables included a complete blood count, serum creatinine, urinalysis, anti-dsDNA, antiphospholipid (anticardiolipin, lupus anticoagulant) antibodies, C3, and C4 levels. Clinical and cognitive assessments, blood collection and DCE-MRI scanning were performed on the same day.
Demographic and clinical features of patients with systemic lupus erythematosus (SLE; n=65)
Cognitive function
Clinical neuropsychological tests, based on ACR recommendations,27 focused on five broad cognitive domains commonly affected in SLE.28 Information processing speed and executive abilities were represented by the Symbol Digit Modalities Test29 and the Design Fluency test (‘fixed’ generation of designs guided by predetermined rules),30 respectively. Components of the California Verbal Learning Test II31 provided indices of attention span (number of words recalled correctly on trial 1), new learning (total words recalled over five list presentations on trials 1–5) and delayed spontaneous recall (number of word recalled spontaneously after a 20 min delay) for verbal information. Raw scores were standardised based on normative data published for each test, and converted to Z-scores.30 Z-scores ≤−1.5 were considered to reflect ‘impaired’ performance.
Imaging
MRI acquisition
Images were acquired using a 3T MRI scanner (Discovery MR750, GE Healthcare, Waukesha, Wisconsin, USA), with a 32-channel MR Instruments head coil. The sequences for BBB assessment included: (1) a T1-weighted three-dimensional (3D) sagittal anatomical scan (BRAVO, TE/TR=2/6 ms, TI=450 ms, Field-of-View (FOV) 224 m, acquisition matrix 224×224×168, voxel size 1×1×1 mm, acceleration 2, averages 2, scan time 5 min 42 s); (2) a T1-weighted 3D tilted axial sequence with variable flip angles (5°–10°–30°, DESPOT1, TE/TR=2/10 ms, flip angle 15°, averages 2, FOV 240 mm, acquisition matrix 192×192×34, voxel size 1.25×1.25×6 mm, scan time 6 min 39 s) for the calculation of precontrast T1 map32; and (3) a T1-weighted 3D axial dynamic scan (LAVA, TE/TR=2/4 ms, FOV 240 mm, acquisition matrix: 192×192×34, voxel size 1.25×1.25×6 mm, flip angle 15°, averages 1, Δt=20 s) acquired between minutes 6 and 20 after intravenous injection of the magnetic contrast Gadobenate Dimeglumine (0·1 mmol/kg, MultiHance, Bracco Imaging Canada, Montreal, Quebec).
Volume analysis
T1-weighted anatomical images were processed using VolBrain software (http://volbrain.upv.es),33 an online pipeline that registers images to the Montreal Neurological Institute (MNI) space, and reports the volumes of expert-labelled anatomical structures as percentage of total intracranial cavity.33 We analysed the volume of the following 23 structures: right/left cerebral gray/white matter, right/left cerebellum gray/white matter, right/left caudate, right/left putamen, right/left thalamus, right/left globus pallidus, right/left hippocampus, right/left amygdala, right/left nucleus accumbens and the brainstem.
BBB leakage analysis
Contrast extravasation due to cross-BBB leakage leads to increased T1-weighted signalling in the affected tissue, allowing the calculation of the contrast leakage rate. To achieve this, T1-weighted images acquired continuously post contrast injection are first registered and normalised to MNI coordinates using SPM12 (University College London, www.fil.ion.ucl.ac.uk/spm). The signal magnitudes of the T1-weighted images are then converted to contrast concentration values,32 and concentration–time curves are constructed for every brain voxel. The concentration–time curves can next be fitted to one of several pharmacokinetic models, allowing the calculation of parameters corresponding to leakage rates. We used the linear model17 18 24 34 which estimates the leakage rate Ki (mMol/min) by calculating the slope of each concentration–time curve between 6 and 20 min. To compensate for intersubject variabilities (due to heart rate, blood flow or rate of contrast injection), each voxel’s leakage rate was normalised to that of the superior sagittal sinus, resulting in a dimensionless leakage-rate measure. With each voxel represented by the calculated leakage rate, 3D maps of BBB leakage were constructed for each subject. Leakage rates were considered pathological when exceeding 0.02, the 95th percentile of all values in a cohort of control subjects.18 The per cent of suprathreshold voxels was used as a measure reflecting overall BBB leakage.
To identify individuals with overall BBB leakage significantly different from the majority of participants, we applied an outlier analysis. The Median Absolute Deviation approach was used for outlier identification, as it is more robust than traditional thresholding using standard deviations around the mean.35 We calculated the median value of all 74 subjects (65 SLE and 9 controls) and the median of absolute deviations from the median. The threshold for abnormal values was defined as the median plus two medians of absolute deviations from the median. Participants with overall BBB leakage above this threshold were considered outliers, and this group was termed ‘extensive BBB leakage’.
The 3D BBB leakage maps were segmented in accordance with the VolBrain atlas.33 BBB leakage within the above-detailed 23 structures was calculated as the per cent of each structure’s voxels with suprathreshold leakage (ie, leakage rates exceeding 0.02).
Statistical analysis
Continuous variables were compared using the Wilcoxon rank sum test, and categorical variables using the χ2 test. The false discovery rate method was used to correct for multiple comparisons.
Results
Demographic and clinical characteristics
The 65 patients with SLE were predominantly Caucasian (89%) and women (87.7%), with a mean age of 48.9±13.3 years (table 1). The median disease duration was 14 years,1–44 with a mean±SD of 15.1±10.5. Cumulative disease manifestations, medication utilisation and autoantibodies reflected the general lupus population,39 with low generalised disease activity and modest organ damage.
Prior NP events from all causes occurred in 50/65 (77%) patients and NP events attributable to SLE were present in 15/65 (23%). The latter included transient ischaemic attacks (n=4), stroke (n=3), cranial neuropathy (n=3), seizure disorder (n=2), acute confusional state (n=2), psychosis (n=2) and aseptic meningitis (n=1). Neuropsychological testing was omitted in one patient who was not a native English speaker. Impairment in one or more cognitive tests was present in 31/65 (47.7%) patients. This included deficits in information processing speed (11%), attention span (22%), new learning (4.7%), delayed recall (12.5%) and executive abilities (22%).
A subgroup of patients with SLE has extensive BBB leakage
Three-dimensional maps of BBB leakage rates were calculated for all patients with SLE and controls (figure 1A). Compared with controls, patients with SLE had significantly higher brain volumes with pathological BBB leakage (p=0.04, figure 1B). Outlier analysis was applied to identify subjects with abnormally high overall BBB leakage, termed ‘extensive BBB leakage’. Notably, all 16 individuals identified as outliers were patients with SLE. Those with lower levels of BBB leakage included all controls and 49 patients with SLE. As SLE patients within the lower BBB leakage group were comparable to controls (p=0.3, figure 1B), they were considered to have normal BBB function.

A subgroup of patients with systemic lupus erythematosus (SLE) has extensive blood-brain barrier (BBB) leakage. (A) The rate of BBB leakage was quantified for every brain voxel, with shades of blue representing tissue with non-permeable BBB and shades of red representing contrast agent accumulation due to BBB leakage. A qualitative review of leakage maps in these selected cases illustrates that some patients with SLE are comparable to controls, while others exhibit visibly higher number of voxels with BBB leakage. (B) The per cent of brain volume with BBB leakage was quantified for each subject, revealing a significant difference between patients with SLE and controls (p=0.04). Outlier analysis of all 74 participants identified a group with ‘extensive BBB leakage’, consisting of 16 patients with SLE; and a group termed ‘normal BBB leakage’, consisting of 9 controls and 49 patients with SLE.
Extensive BBB leakage in patients with SLE is associated with smaller gray matter volume
Volumetric comparison of 23 brain structures revealed that SLE patients with extensive BBB leakage had significantly smaller cerebral gray matter volumes compared to controls (right and left, p=0.04, corrected for multiple comparisons, figure 2A). To examine whether the decrease in cerebral gray matter volume was associated with structure-specific BBB leakage, we compared the extent of BBB leakage within the 23 structures between the two SLE groups and controls. While the volumetric differences were restricted to cortical gray matter, differences in BBB leakage were present in all 23 structures (p<0.001, corrected for multiple comparisons, figure 2B).
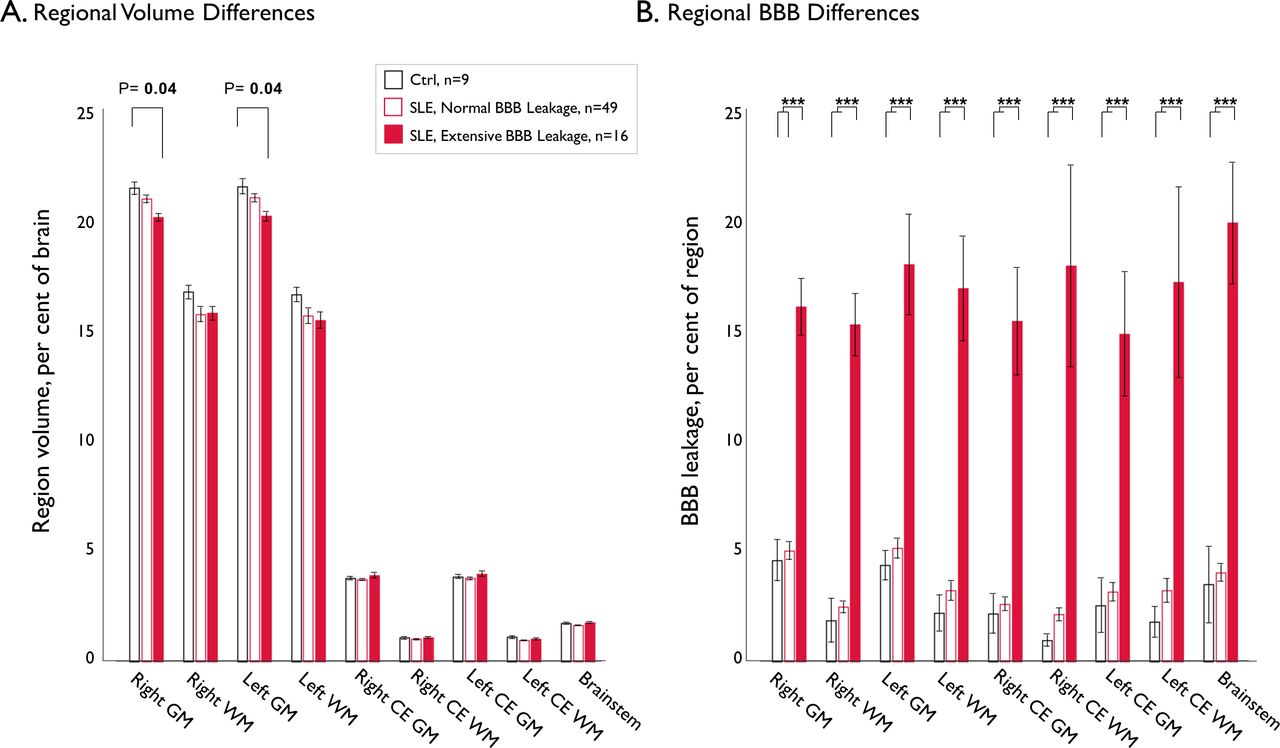
Extensive BBB leakage in patients with systemic lupus erythematosus (SLE) is associated with smaller grey matter volume. (A) Depiction of the 9 largest brain structures (of the 23 regions compared between the groups) illustrates the reduced right-grey and left-grey matter volumes in patients with extensive blood-brain barrier (BBB) leakage compared with controls (p=0.04, corrected for multiple comparisons). There were no volumetric differences in any other regions. (B) Comparison of BBB leakage in the same 23 brain structures revealed that the ‘extensive BBB leakage group’ had higher levels of leakage in all regions (the same 9 regions are depicted in B and A), compared with patients with normal BBB leakage and controls (p≤0.001, corrected for multiple comparisons). The Wilcoxon rank sum test was used to compare between the groups, and the false discovery rate algorithm was used to correct for multiple comparisons. Error bars denote SE of the mean. Asterisks denote level of significance, with ***p≤0.001. CE, cerebellum; GM, grey matter; WM, white matter.
Extensive BBB leakage in patients with SLE is associated with cognitive impairment
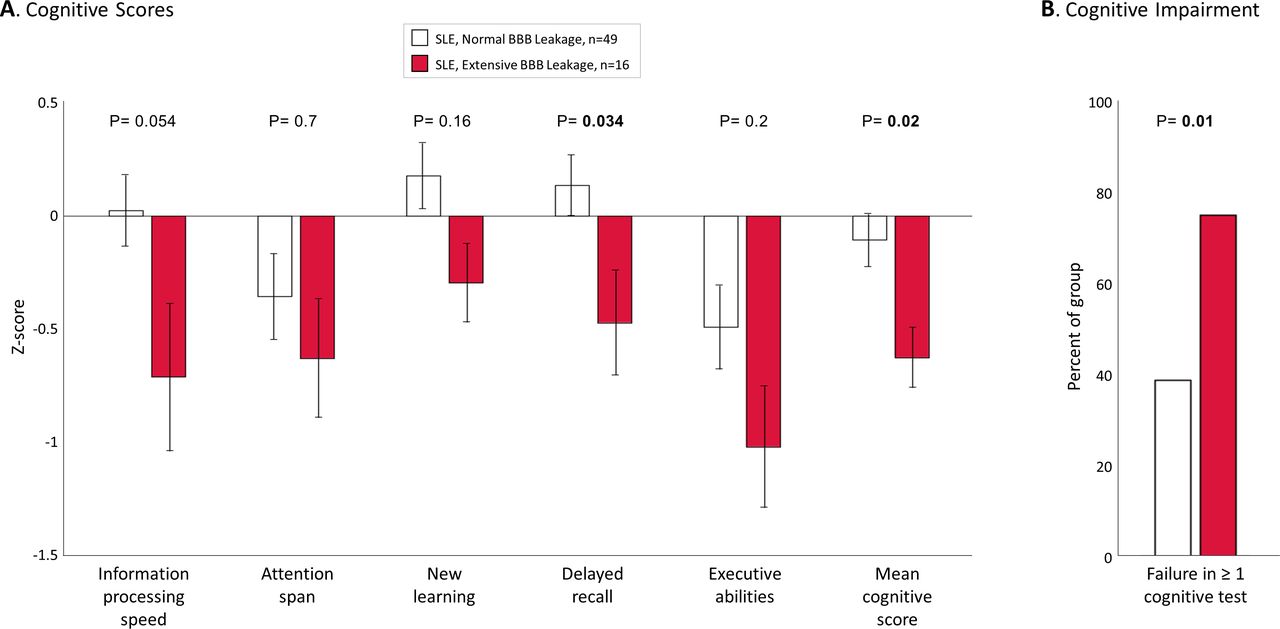
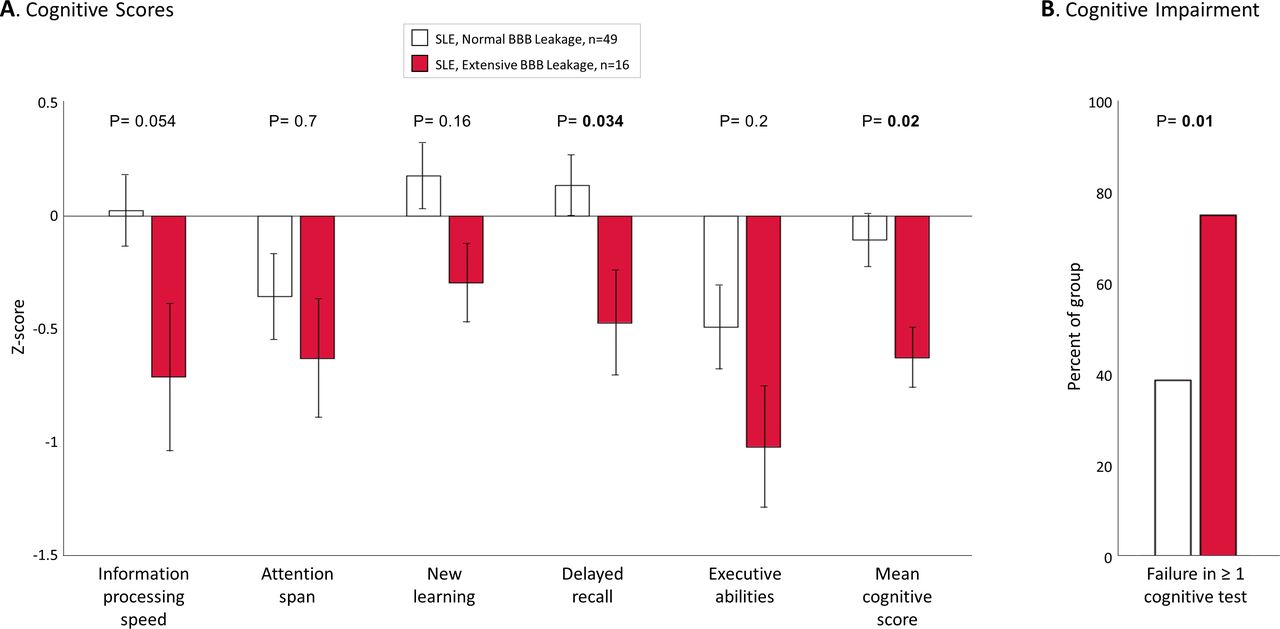
Compared with patients with normal BBB leakage, patients with extensive BBB leakage had poorer delayed recall (p=0.034, figure 3A) and worse overall cognitive test performance (averaged Z-score of five cognitive tasks, p=0.02). Impairment in ≥1 cognitive task was present in 47.7% of the total SLE sample, but occurred in 75% of patients with extensive BBB leakage, compared with only 38.8% of patients with normal BBB leakage (p=0.01, figure 3B). Testing for potential confounders (table 2) revealed that the groups were similar in age, use of medications, prior NP events due to any cause and those attributed to SLE, disease activity (SLEDAI-2K), cumulative organ damage (SDI) and rates of hypertension and diabetes mellitus, but that patients with extensive BBB leakage were more likely to be active smokers (p=0.03).
Comparison between patients with systemic lupus erythematosus (SLE) with extensive versus normal blood-brain barrier (BBB) leakage
{kind=link}
{kind=link}
{kind=link}
Extensive blood-brain barrier (BBB) leakage in patients with systemic lupus erythematosus (SLE) is associated with cognitive impairment. (A) SLE patients with extensive BBB leakage had worse delayed recall and lower mean cognitive scores (averaged Z-scores of the selected test scores representing each broad cognitive domain) compared with patients with normal BBB leakage (p=0.02, Wilcoxon rank sum test). (B) The extensive BBB leakage group also had a significantly higher per cent of subjects failing at least one cognitive test (p=0.01, χ2 test). Error bars denote SE of the mean.
Discussion
The proposed pathogenesis of NPSLE involves variable autoimmune-mediated prothrombotic and proinflammatory mechanisms.3 4 36 Microvascular damage is common in many organs affected by SLE37 and has been found in brains of SLE patients examined postmortem.14 While impairment of the BBB may be a core component of the pathogenesis of NPSLE,12 13 the evidence for this remains indirect and circumstantial,14 38 39 as clinical tools for diagnosing BBB dysfunction are lacking. In the current study, we employed DCE-MRI to quantify BBB permeability directly and objectively in 65 ambulatory patients with SLE. We found associations of extensive BBB leakage with reduced cortical grey matter and with concurrent cognitive impairment. These findings are a key step in establishing the role of BBB dysfunction in the pathogenesis of NPSLE and highlight the BBB as a potential diagnostic and therapeutic target.
The BBB provides the major physical interface between the circulation and the brain,13 regulating the passage of substances in and out of brain neuropil and maintaining the chemical environment needed for normal neuronal function. This control occurs through tightly connected endothelial cells, and the pericytes and astrocytes surrounding the endothelium. Dysfunction of the BBB allows leakage of blood components into the brain neuropil, triggering inflammatory processes that alter glial function, extracellular matrix composition, neuronal connectivity and neuronal function. One widely studied example is the inflammatory cascade initiated when albumin, a large serum protein, enters the brain. Albumin binds to astrocytes and activates the proinflammatory transforming growth-factor beta (TGF-β) cascade, resulting in neuronal hyperexcitability and delayed neurodegeneration.6 Similarly, thrombin and activated protein C enhance neuronal excitability in the brain.5
In SLE, autoantibodies and inflammatory mediators may be responsible for BBB leakage.40 Antiribosomal P and anti-NR2 autoantibodies,11 associated with NPSLE, were shown to bind the surface of cultured endothelial cells, causing endothelial activation, upregulation of adhesion molecules and increased production of cytokines such as interleukin 6. Complement activation products, including C5a generated by immune complexes, can cause in vitro BBB disruption and apoptosis of endothelial cells in an animal model of SLE.10 Once the BBB is breached, circulating autoantibodies (including antiribosomal P7 and anti-NR2 antibodies8) can access the brain and bind to neuronal cells, causing apoptotic cell death,7 8 as well as microglial activation, synaptic pruning and reduced synaptic density.9
Non-SLE specific mechanisms such as hypertension, systemic infection and cigarette smoking can also injure endothelial cells and increase BBB permeability.41 42 More frequent in patients with SLE, these variables may be viewed as modifiable risk factors for BBB dysfunction. Our data revealed an association between current cigarette smoking and extensive BBB leakage in our SLE cohort. This finding is supported by experimental evidence that tobacco smoke disrupts endothelial tight junctions,43 and generates highly reactive oxygen species that cause oxidative damage.44
Our study focused on cognitive impairment as a clinical phenotype of NPSLE. Neuropsychological testing permitted a standardised and objective determination of cognitive impairment, which can be regarded as both a subset of NPSLE and an indicator of overall brain health. A recent review reported 38% point prevalence (95% CI 33 to 43) of cognitive impairment in patients with SLE.1 Our study identified a comparable prevalence of 47.7% that is similar to previously reported studies.2 Our patients were ambulatory with stable SLE and participated regardless of cognitive symptoms. It is, therefore, striking that extensive BBB leakage was found in 24.6% of patients, and one might anticipate an even higher prevalence in SLE patients with more overt NPSLE manifestations. The fact that not all patients with cognitive impairment had extensive BBB leakage is not surprising, since impaired cognition can result from a variety of factors, including many unrelated to SLE. However, patients with extensive BBB leakage were twice as likely to have cognitive impairment compared to those with normal BBB function, suggesting that the BBB plays an important role in this NPSLE manifestation. Notably, while 77% of patients had a history of NP events, none had clinically active NP events during the study which may account for the lack of association between extensive BBB leakage and clinically overt NP events in our cohort.
In early BBB studies, evidence for BBB leakage was inferred from cerebrospinal fluid (CSF) proteins that are normally restricted to the peripheral circulation (eg, albumin13 and immunoglobulin G45). However, the presence of these proteins in the CSF can result from BBB-unrelated factors, such as blood-CSF barrier dysfunction (ie, damaged choroid plexus epithelium) or meningeal barrier dysfunction (ie, damaged arachnoid epithelium).13 These barriers differ significantly from the BBB, the capillaries of which penetrate deep into the brain parenchyma. To address the limitations of CSF markers, BBB studies have evolved to MRI-based BBB assessment that allows calculation of cross-BBB contrast leakage in every voxel of the brain. Such studies have already demonstrated BBB dysfunction in patients with multiple sclerosis,19 stroke,20 traumatic brain injury18 and dementia.21 Two recent pilot studies demonstrated the proof of concept of MRI-based BBB assessment in 6 adult patients with SLE (focusing on 5 regions of interest),22 and in 11 children with SLE (using arterial spin labelling).46 While limited by small sample sizes, both studies reported increased BBB leakage in patients with SLE compared with controls (finding lower cognitive performance in the 6 adult patients and normal cognition in the 11 children with SLE). Here, we studied BBB leakage in a cohort of 65 patients, confirming higher levels of leakage compared with controls, and revealing that this difference is driven by a subgroup of patients. Our results further demonstrate that compared with the rest of the SLE cohort, this subgroup had worse cognitive performance, and smaller cortical grey matter volumes, a finding commonly associated with neurodegenerative dementias. These findings support the hypothesis that BBB leakage may mediate neurodegeneration in SLE, leading to loss of grey matter and cognitive impairment. Our findings also highlight the potential of BBB imaging as a biomarker for identifying SLE patients at risk of cognitive decline.
Strengths of our study include the lack of explicit recruitment bias, and the temporal proximity between clinical and neuroimaging protocols, usually within 6 hours. Longitudinal studies of cognition in SLE indicate that impairments can be subtle and evanescent.47 Thus, the short interval between neuroimaging and cognitive testing increases the biological plausibility of the observed associations. Our study reflects the demographic characteristics of SLE patients in our clinic48 but may not be applicable to younger SLE patients with more diverse race/ethnicity and shorter disease duration. The small number of controls and the sample size of our SLE cohort were additional limitations, precluding a more detailed examination of associations between BBB permeability in specific brain regions and scores in specific cognitive tests. A more comprehensive cognitive battery (allowing precise distinction between cognitive domains) and a larger sample size are needed to address this important question. Additionally, our imaging protocol required a gadolinium-based contrast that may be a concern in patients with substantial renal impairment. The use of contrast-free BBB imaging (eg, arterial spin labelling), or identification of reliable serum-based markers of BBB dysfunction, may allow wider applicability of BBB pathology as a screening biomarker.
The current study provides the first compelling evidence for a link between extensive BBB leakage and cognitive impairment within a sample of SLE patients. Future longitudinal studies are needed to examine changes in BBB permeability over time and whether concurrent presence of circulating autoantibodies increases the risk of cognitive impairment or other NPSLE features. Our findings also highlight the need to clarify the exact mechanisms underlying BBB damage and subsequent neuronal dysfunction in SLE, and the therapeutic potential of treatments targeting these mechanisms.
Acknowledgments
The corresponding author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive license (or non-exclusive for government employees) on a worldwide basis to the BMJ Publishing Group and its Licensees to permit this article (if accepted) to be published in Annals of the Rheumatic Diseases and any other BMJPGL products to exploit all subsidiary rights, as set out in our license http://group.bmj.com/products/journals/instructions-for-authors/licence-forms.
References
Footnotes
Handling editor Josef S Smolen
Contributors All authors participated in the collection of research data or the data analysis or writing and critical review of the manuscript.
Funding This study was supported by the Canadian Institutes of Health Research (CIHR, MOP-88526 and PJT148896), Nova Scotia Health Research Foundation (NSHRF, MED-EST-2015-10067), Natural Sciences and Engineering Research Council of Canada (NSERC, RGPIN 04293-17) and Brain Canada (BC PSG2015-3780), Mitacs grant IT11112 and Nova Scotia Research Fund.
Disclaimer The funders of the study had no role in study design, patient recruitment, data collection, analysis, interpretation or publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval The study was approved by the Nova Scotia Health Authority Research Ethics Board, and participants provided written informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.