Article Text

Abstract
Objectives The recombinant zoster vaccine (RZV) containing a strong non-aluminium adjuvant is associated with increased risk of gout flares, presumably via NLRP3 inflammasome activation. We tested the possibility that other vaccines may also be associated with gout flares.
Methods We conducted an online case-crossover study of patients with gout to examine the association between vaccination and gout flares. We collected information through the Internet on exposures to potential risk factors, including vaccinations, during 2-day hazard periods prior to gout flare and 2-day control periods without a flare. Conditional logistic regression was used to adjust for covariates.
Results There were 517 participants with gout (mean age 55 years, 79% male) who experienced gout flares during follow-up. There were 28 vaccinations during 990 hazard periods and 21 vaccinations during 1407 control periods. Vaccination was associated with twofold higher odds of gout flare (adjusted OR 1.99; 95% CI 1.01 to 3.89).
Conclusion Our findings suggest vaccines other than RZV are associated with increased odds of gout flares, potentially through a shared pathogenetic mechanism like NLRP3 inflammasome. However, the absolute magnitude of increased odds of gout flares with vaccinations remains small and must be interpreted within the context of the overwhelming benefits of vaccinations.
- case-crossover study
- gout
- vaccination
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The new recombinant shingles vaccine (RZV) was associated with increased risk of gout flares.
Aluminium adjuvants contained in vaccines can activate the NLRP3 inflammasome in vitro.
What does this study add?
This study showed that receiving a non-RZV vaccine was associated with a two-fold higher odds of developing a gout flare within 2 days of vaccination compared with periods when vaccination was not administered.
How might this impact on clinical practice or future developments?
These findings warrant further investigation into whether temporary prophylactic use of anti-inflammatory medications may mitigate the risk of gout flares with vaccination without affecting vaccine efficacy.
These findings must be interpreted within the context of overwhelming benefits of vaccines worldwide.
Introduction
The recombinant zoster vaccine (RZV) provides enhanced protection against shingles and postherpetic neuralgia and is now the preferred zoster vaccine endorsed by the Advisory Committee on Immunization Practices.1 However, safety data from two phase III trials for RZV demonstrated a 3.6-fold higher risk of gout.2–4 Whether this is unique to RZV or if other vaccines may also increase the risk of gout flares is unknown. Given gout’s prevalence among the elderly5 6 and those with multiple comorbidities7 who benefit most from routine vaccinations, it is important to determine whether vaccines other than RZV similarly increase the risk of gout flares.
Studies have shown that monosodium urate-induced activation of the NLRP3 inflammasome, leading to maturation and release of interleukin-1 beta, is a key second signal triggering the inflammatory cascade responsible for gout flares.8 The non-aluminium adjuvant used in RZV is hypothesised to activate the NLRP3 inflammasome.4 Furthermore, aluminium adjuvants, which are contained in more than half of routinely administered adult vaccines,9 have also been shown to activate the NLRP3 inflammasome.10 11 This study tested the hypothesis that vaccines other than RZV may also be associated with increased acute gout flares using a prospective case-crossover study12 that recorded both exposures and gout flares before the RZV vaccine was available.
Methods
Study design and participants
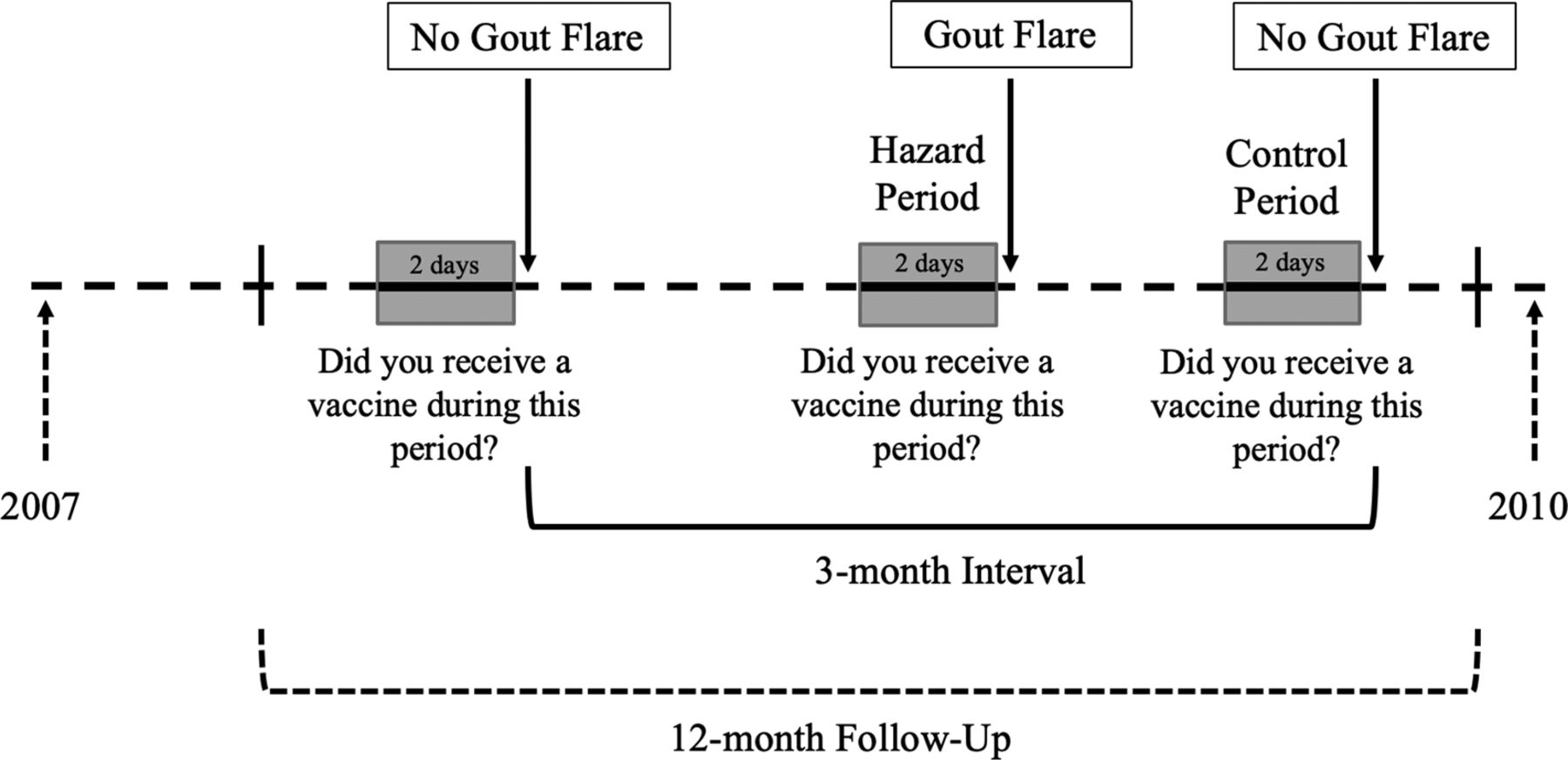
We conducted a prospective, Internet-based, case-crossover study with the primary aim to investigate purported triggers for recurrent gout flares as previously described.12 This study was conducted between 2003 and 2010, thus, before the introduction of the RZV vaccine.1 The study design and timing of exposure measurements in relation to recurrent gout flares are depicted in figure 1. Eligibility criteria included history of physician-diagnosed gout and at least one gout flare in the last year.12 Medical records pertaining to gout diagnosis and treatment were collected so that the diagnosis could be adjudicated according to the 1977 American College of Rheumatology (ACR) Preliminary Gout Classification Criteria.13 Each participant was asked to complete online questionnaires every 3 months over the 1-year follow-up and at the time of a gout flare. A question regarding vaccination was added in 2007. The case-crossover study design allows each participant to serve as his/her own control, thereby eliminating time-fixed confounding between participants.12
{kind=link}
Study design and timing of exposure measurements.
Patient and public involvement
There was no patient or public involvement in the design or conduct of this study.
Ascertainment of gout flares
Participants were asked to log into the study website at the time of gout flares. Consistent with the methods proposed by ACR/European League Against Rheumatism,14 we collected data at the time of gout flare regarding date of onset, clinical signs and symptoms, and any medications used to treat the flare.
Ascertainment of exposure
Subjects completed questionnaires about exposures to purported risk factors such as purine intake, alcohol consumption and medication exposures during the 2-day period prior to the gout flare (ie, hazard period). To ascertain vaccination, subjects were asked: ‘Did you receive an immunization, such as a flu shot, tetanus, travel vaccination?’ These same questions regarding exposures to purported risk factors were also ascertained over a 2-day period when the participant was free from a gout flare (ie, control period) every 3 months over the 1-year follow-up.
Statistical analysis
Because every participant could contribute multiple hazard or control periods which were matched within a participant, we used a conditional logistic regression for M:N matched case-control study to examine the relation of vaccination to risk of gout flares, adjusting for alcohol consumption, diuretic use and purine intake.
Results
There were 517 participants with gout who completed both hazard and control period questionnaires; their baseline characteristics are shown in table 1. The mean age was 55 years, and 79% were male. Most responders were Caucasian and college educated (89% and 59%, respectively). The participants reported a mean disease duration of 7.9 (range 0–55) years, and a mean of 1.9 gout attacks per person.
Participant characteristics
During the 1-year follow-up period, the participants completed 990 hazard period questionnaires, of which 28 reported receiving vaccinations in the 2-day period prior to flare onset (table 2). Of the 1407 control period questionnaires completed, 21 of them reported receiving vaccinations. Receiving a vaccination within the prior 2 days was associated with two-fold higher odds of developing a gout flare (adjusted OR 1.99; 95% CI 1.01 to 3.89). We pursued a parsimonious multivariable model, including only conventionally known triggers of gout (ie, alcohol, purine and diuretics), as our bivariate models did not suggest confounding by any covariate (see online Supplemental Table 1). For male participants, vaccination within the prior 2 days was associated with a 2.4-fold (adjusted OR 2.35, 95% CI 1.12 to 4.92) higher odds of developing a gout flare, whereas the small number of vaccinations did not allow for robust multivariable adjustment (see online supplemental table 1). The OR tended to be larger among participants ≤ 60 years, those on allopurinol, non-steroidal anti-inflammatory drugs and diuretics, and those with higher alcohol and purine consumption, although none reached statistical significance (see online supplemental table 1) (all p values for interaction >0.05).
Supplemental material
Vaccination in the prior 48-hour period and risk of recurrent gout flares
Discussion
In this case-crossover study of patients with gout, vaccination in the prior 2 days was associated with a two-fold increased odds of gout flares compared with periods when vaccination was not administered. Because this study was conducted before the availability of RZV, our finding expands on what is currently known about vaccinations and risk of gout flares. In two phase III clinical trials for RZV, 27 patients (0.18%) who received RZV reported a gout flare within 30 days of vaccine administration compared with 8 patients (0.05%) who received placebo,2 3 yielding a 3.6-fold higher risk of gout flare with RZV.2–4 This has prompted the implementation of an enhanced postmarketing surveillance programme for gout flares.4 Our findings suggest that this adverse effect is also applicable to other vaccines, although the effect size may be lower.
These findings collectively raise relevant pathogenic implications. The activation of the NLRP3 inflammasome is hypothesised to be the key mechanistic link between vaccinations and gout flares. The non-aluminium adjuvant contained in RZV triggers a local and transient activation of the innate immune system through MPL and QS-21 signalling, the latter of which is believed to involve the NLRP3 inflammasome.15 Aluminium adjuvants, which are contained in half of all routine adult vaccines, including tetanus, diphtheria and pertussis (Tdap, Td), pneumococcal conjugate (PCV-13) and hepatitis B vaccines,16 have also been shown to activate the NLRP3 inflammasome in vitro.10 11 As such, aluminium adjuvants in vaccines can conceivably trigger gout flares through the same mechanism. Whether other adjuvants, live and killed organisms, and recombinant peptide constituents of vaccines also promote gout flares remains to be clarified.
Nevertheless, the clinical implications of our findings must be interpreted carefully, as vaccines decrease the morbidity and mortality associated with communicable illnesses.17 Given the high prevalence of gout among patients most susceptible to adverse outcomes from infections, such as the elderly5 6 and those with multiple comorbidities,7 avoiding vaccinations due to the increased odds of gout flares is not advisable. There appears to be a low absolute frequency of gout flares in relation to vaccination, both in the RSV trials2–4 and our current study. Studying the capacity of prophylactic use of anti-inflammatory medications to prevent such flares without hindering vaccine efficacy may be warranted.
Some strengths and weaknesses of this study warrant comment. The data were deliberately collected prospectively through the Internet to effectively capture real-life time-varying triggers of gout over a short timeframe (ie, 24–48 hours). As such, this study design is highly adaptable to assessing the effect of a transient exposure as a trigger for an acute event,18 and self-matching of each participant minimises bias in control selection and removes the confounding effects of factors that are constant within a subject over the study period but differ between participants.19 The participants in our study may not be representative of patients with gout in the general population given predominance of White and college-educated patients; however, the biological effects of vaccination on gout flares should be similar. Although this study relied on self-report of exposures, vaccination was not suspected of causing gout flares during the entirety of this study, leaving no ground for preferential recall. While we were unable to verify vaccine administration through the patients’ medical records, vaccination is known to be one of the most accurately reported medical exposures,20 thereby minimising potential for recall bias. Weaknesses include the small number of events not allowing for robust conclusions from our subgroup analyses and lacking information on specific vaccines administered which may have been associated with gout flares.
In conclusion, this study suggests that vaccination in the prior 2 days is associated with a two-fold higher odds of gout flares compared with periods when no vaccine was administered. However, these findings must be interpreted within the context of the low frequency of gout flares in relation to vaccinations and the overwhelming benefits of vaccinations.
References
Footnotes
Handling editor Josef S Smolen
Contributors TN, YZ, HC contributed to study design. CC, TN, CEC, YZ and HC contributed to study conduct. CY, NM, YZ and HC contributed to study analysis. All authors contributed to interpretation of results. CY and HC drafted the manuscript, and all authors reviewed and revised the manuscript for content.
Funding This study was supported by the National Institutes of Health [P60 AR047785]. CY is supported by Ruth L Kirschstein Institutional National Research Service Award [T32-AR-007258]. NM is supported by a Fellowship Award from the Canadian Institutes of Health Research. RT is supported by the National Institutes of Health [AR060772] and VA Research Service [I01BX001660]. DJH is supported by an NHMRC practitioner fellowship. TN was supported by [K24 AR070892] for this work. HKC is supported by the National Institutes of Health [AR060772].
Disclaimer RT consultant to SOBI, Horizon and Selecta. DJH consultant to TLC Bio, Pfizer, Lilly, Merck Serono. TN consultant to (all unrelated to this study) Pfizer, EMD, Merck Serono, Regeneron, Novartis. HKC reports research support from AstraZeneca, and consultant to Takeda, Selecta, GSK and Horizon (all less than $10 000).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Boston University Medical Center Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.