Article Text

Abstract
Objectives To provide the level and trends of prevalence, incidence and disability adjusted life years (DALYs) for rheumatoid arthritis (RA) in 195 countries from 1990 to 2017 by age, sex, Socio-demographic Index (SDI; a composite of sociodemographic factors) and Healthcare Access and Quality (an indicator of health system performance) Index.
Methods Data from the Global Burden of Diseases, Injuries, and Risk Factors study (GBD) 2017 were used. GBD 2017 modelled the burden of RA for 195 countries from 1990 to 2017, through a systematic analysis of mortality and morbidity data to estimate prevalence, incidence and DALYs. All estimates were presented as counts and age-standardised rates per 100 000 population, with uncertainty intervals (UIs).
Results Globally, the age-standardised point prevalence and annual incidence rates of RA were 246.6 (95% UI 222.4 to 270.8) and 14.9 (95% UI 13.3 to 16.4) in 2017, which increased by 7.4% (95% UI 5.3 to 9.4) and 8.2% (95% UI 5.9 to 10.5) from 1990, respectively. However, the age-standardised rate of RA DALYs per 100 000 population was 43.3 (95% UI 33.0 to 54.5) in 2017, which was a 3.6% (95% UI −9.7 to 0.3) decrease from the 1990 rate. The age-standardised prevalence and DALY rates increased with age and were higher in females; the rates peaked at 70–74 and 75–79 age groups for females and males, respectively. A non-linear association was found between age-standardised DALY rate and SDI. The global age-standardised DALY rate decreased from 1990 to 2012 but then increased and reached higher than expected levels in the following 5 years to 2017. The UK had the highest age-standardised prevalence rate (471.8 (95% UI 428.9 to 514.9)) and age-standardised incidence rate (27.5 (95% UI 24.7 to 30.0)) in 2017. Canada, Paraguay and Guatemala showed the largest increases in age-standardised prevalence rates (54.7% (95% UI 49.2 to 59.7), 41.8% (95% UI 35.0 to 48.6) and 37.0% (95% UI 30.9 to 43.9), respectively) and age-standardised incidence rates (48.2% (95% UI 41.5 to 55.1), 43.6% (95% UI 36.6 to 50.7) and 36.8% (95% UI 30.4 to 44.3), respectively) between 1990 and 2017.
Conclusions RA is a major global public health challenge. The age-standardised prevalence and incidence rates are increasing, especially in countries such as Canada, Paraguay and Guatemala. Early identification and treatment of RA is vital especially among females, in order to reduce the ongoing burden of this condition. The quality of health data needs to be improved for better monitoring of disease burden.
- rheumatoid arthritis
- epidemiology
- health services research
Statistics from Altmetric.com
Key messages
What is already known about this subject?
No updated global study on rheumatoid arthritis (RA) has been published after 2010.
What does this study add?
Globally, the age-standardised point prevalence and annual incidence rates of RA increased by 7.4% (95% uncertainty interval (UI) 5.3 to 9.4) and 8.2% (95% UI 5.9 to 10.5) from 1990, respectively.
The global age-standardised disability adjusted life year rate decreased from 1990 to 2012 but then increased and reached higher than expected levels in the following 5 years to 2017.
The UK had the highest age-standardised prevalence and incidence rates in 2017.
Canada, Paraguay and Guatemala showed the largest increases in age-standardised prevalence and incidence rates between 1990 and 2017.
How might this impact on clinical practice or future developments?
Early identification and treatment of RA is vital especially among females, in order to reduce the burden and disability associated with this condition and to provide appropriate care for this community.
Introduction
Rheumatoid arthritis (RA) is a systemic auto-immune disease. Symmetrical inflammatory polyarthritis is the primary clinical manifestation, usually beginning in the small joints of the hands and the feet, spreading later to the larger joints.1 A number of national studies have examined prevalence, incidence and mortality of RA2–4; however, there is a lack of a comprehensive global study. In 2016, the WHO estimated the years lived with disability (YLD), years of life lost (YLL) and disability adjusted life years (DALYs) of RA by age, sex and country5 but no paper has been published in this regard. Recently, Sebbag and colleagues reported the global burden of musculoskeletal disease for 2000, 2010 and 2015 using aforementioned WHO database but they have not specifically focused on RA and their estimates rely on 2015 data.6 An analysis utilising the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2010 reported global and regional burden of RA in terms of prevalence and DALYs,7 but national-level estimates were not provided. Association of burden of RA with sociodemographic status of countries was not examined in that study. Another study was conducted on GBD 2013 musculoskeletal data combined and were only reported for Eastern Mediterranean region.8 Overall, no updated global study on RA has been published after 2010. Hence, in the present study, we examined the data from GBD 2017 for global, regional and national prevalence, incidence and DALY in terms of counts and age-standardised rates from 1990 to 2017 by age, sex, Socio-demographic Index (SDI; a composite of sociodemographic factors) and Healthcare Access and Quality (HAQ; an indicator of health system performance) Index to provide comprehensive and comparable analysis of RA burden.
Methods
Overview
GBD 2017, conducted by Institute of Health Metrics and Evaluation (IHME), involved 195 countries, seven super-regions and 21 regions from 1990 to 2017.9 Three hundred and fifty-four diseases and injuries, 282 causes of death and 84 risk factors were systematically analysed in the GBD 2017 study. The general methodology of GBD 2017 and its main changes compared with previous years have been described in previous publications.9–12 The additional information on fatal and non-fatal estimates can be found at https://vizhub.healthdata.org/gbd-compare/ and http://ghdx.healthdata.org/gbd-results-tool. Methods were developed by and most analyses reported here were conducted at IHME.
Case definition and data sources
As stated in many epidemiological studies, RA is a systemic autoimmune disorder that causes pain and swelling of the joints. While RA is known to affect internal organs in addition to the joints, these extra‐articular effects are not factored into the disability weights (DW) used in GBD. The reference case definition for RA is based on the 1987 guidelines by the American College of Rheumatology (ACR 1987),13 which explain seven diagnostic criteria (1. morning stiffness, 2. arthritis of three or more joint areas, 3. symmetric arthritis, 4. arthritis of hand, 5. rheumatoid nodules, 6. serum rheumatoid factor and 7. radiographic changes), of which four need to be satisfied for a diagnosis. Criteria 1 through 4 must have been present for at least 6 weeks.9 13
A comprehensive systematic review was conducted on RA prevalence, incidence and mortality in GBD 2010 and updated in GBD 2017. Studies with the following characteristics were excluded: (a) non-representative, (b) non-population-based, (c) inadequate primary data on epidemiological parameters, (d) studying a specific type of RA, for example, seropositive RA and (e) reviews. Finally, prevalence (site-years=499), incidence (site-years=151) and other, including remission (site-years=20), were estimated through literature studies included in GBD 2017. Notably, a site-year is a unique combination of location and calendar year and is defined as a country or other subnational geographical unit contributing data in a given year. Also, the number of countries with data was quite small globally, and these numbers were different for estimating the prevalence (n=42), incidence (n=14) and other (n=9). The number of GBD regions with data was higher for prevalence (n=16), compared with incidence (n=6) and other (n=5). In addition, USA claims data for 2000, and 2010–2014 by US state and Taiwan claims for 2016 were included. It is worth mentioning that hospital inpatient data were not used as it was assumed, they would not be representative of true prevalence.9
Data used to estimate RA mortality included vital registration, verbal autopsy, and China disease surveillance data from the cause of death database. Outlier criteria were to exclude data points that were (1) implausibly high or low relative to global or regional patterns, (2) substantially conflicted with established age or temporal patterns, or (3) significantly conflicted with other data sources based from the same locations or locations with similar characteristics that is, SDI.
Disease model
GBD 2017 methods included the standard Cause of Death Ensemble model, which was applied to estimate deaths due to RA. The list of covariates used for the RA model can be found in the appendix methods section of previously published GBD 2017 paper.10 RA prevalence, incidence and mortality data were analysed within the IHME Bayesian meta-regression tool DisMod-MR 2.1 for modelling and calculation of estimates by pooling the available heterogeneous data to adjust for methodological differences and check for internal consistency.
IHME prior settings in the DisMod-MR 2.1 model included setting remission to 0.009–0.021, which is the assumed remission rate for natural disease (ie, drug-free) remission, and it was assumed that there was no incidence or prevalence of RA before the age of 5 years.9 Data from all sources were re‐extracted to better reflect the range of case definitions. ACR 1987 criteria13 was set as the reference, with other definitions including Rome 1961,14 American Rheumatology Association 1958,15 or European League against Rheumatism16 criteria identified with a single study covariate ‘non‐ACR_1987’. Additional study covariates were created for studies using administrative health system data sources; for studies covering regional rather than (sub)‐nationally representative populations; and for claims data. R software V.3.5.2 was used to generate figures of the final estimates of prevalence and incidence rates from data available from ghdx.healthdata.org/gbd-results-tool.
Severity and YLD
The International Classification of Diseases version 10 codes were used for RA (M05-M06.9, M08.0-M08.89) with three sequelae (severity levels) where each sequela had specific DW ranging from 0.11 to 0.58 (see online supplementary table 1). GBD 2013 European Disability Weights Measurement Study and GBD 2010 Disability Weights Measurement Study were used as the sources of DW values. More details are described in previous GBD studies.9 17 Medical Expenditure Panel Surveys were used to specify the proportion of each of the severity levels in patients with RA.9 Then, these proportions were used to split the overall prevalence of RA into the severity categories. Finally, the prevalence of each severity category was multiplied by severity-specific DWs to calculate YLDs.
Supplemental material
Compilation of results
The YLLs were calculated by multiplying the number of deaths in an age group by the remaining life expectancy in that age group, taken from the GBD standard life table. DALYs were then calculated as the sum of YLLs and YLDs. Uncertainty was propagated by sampling 1000 draws at each computational step, combining uncertainty from multiple sources such as input data, corrections of measurement error and estimates of residual non-sampling error. Uncertainty intervals (UIs) were defined as the 25th and 975th values of the ordered draws. We examined the shape of association of RA burden in terms of DALYs with SDI and HAQ for 21 regions and 195 countries using the Smoothing Splines models.18 SDI is a composite indicator of lag-dependent income per capita; that is gross domestic product per capita that has been smoothed over the preceding 10 years, average years of schooling for the population older than 15 years of age, and total fertility rate under the age of 25. It ranges from 0 (less developed) to 1 (most developed). HAQ is an indicator of health system performance and reflects personal HAQ for 195 countries and is calculated based on amenable mortality, that is, deaths from causes that should not occur in the presence of effective medical care. This index ranged from 0 (worst-performing health systems) to 100 (best-performing health systems). Additional details for HAQ have been presented previously.19
Results
Global level
The present study found that globally there were 19 965 115 (95% UI 17 990 489 to 21 955 673) prevalent cases of RA, with an age-standardised prevalence rate of 246.6 per 100 000 (95% UI 222.4 to 270.8), which increased by 7.4% (95% UI 5.3 to 9.4) between 1990 and 2017. Also, RA was responsible for 1 204 599 (95% UI 1 071 090 to 1 331 694) incident cases globally with an age-standardised incidence rate of 14.9 (95% UI 13.3 to 16.4), an increase of 8.2% (95% UI 5.9 to 10.5) between 1990 and 2017 (table 1).
Prevalent cases, incident cases and DALYs for rheumatoid arthritis in 2017 for both sexes and percentage change of age-standardised rates by Global Burden of Disease (GBD) region (generated from data available from: ghdx.healthdata.org/gbd-results-tool/)
The global age-standardised DALY rate showed a decreasing trend from 1990 to 2012 but increased and reached higher levels in the following 5 years. Moreover, RA accounted for 3.4 million (95% UI 2.6 to 4.4) DALYs at the global level, with an age-standardised rate of 43.3 (95% UI 33.0 to 54.5) DALYs per 100 000 population. The age-standardised DALY rate reduced by 3.6% (95% UI −9.7 to 0.3) from 1990 to 2017 (table 1).
Regional level
At the regional-level, the age-standardised prevalence of RA was found to be highest in high-income North America (377.6 (95% UI 356.4 to 400.2)), Western Europe (346.8 (95% UI 314.4 to 378.3)) and the Caribbean (338.9 (95% UI 304.6 to 374.1)). In contrast, Southeast Asia (100.9 (95% UI 89.9 to 112.2)), Oceania (135.3 (95% UI 120.9 to 150.8)) and Western Sub-Saharan Africa (135.7 (95% UI 120.6 to 151.6)) showed the lowest age-standardised rates (table 1).
The age-standardised incidence rates were also found to be highest in high-income North America (22.5 (95% UI 20.9 to 24.1)), South Asia (20.7 (95% UI 18.4 to 22.9)) and Western Europe (20.4 (95% UI 18.3 to 22.4)); whereas, Southeast Asia (6.2 (95% UI 5.5 to 6.9)), Oceania (7.9 (95% UI 7.0 to 8.9)) and Western Sub-Saharan Africa (8.5 (95% UI 7.5 to 9.5)) showed the lowest rates (table 1).
The regional-level age-standardised prevalence and incidence estimates for all GBD 2017 regions have been presented by sex in online supplementary figure 1.
Supplemental material
This study also found that the percentage change in age-standardised prevalence rates during 1990–2017 was not similar across the GBD 2017 regions. East Asia (25% (95% UI 22 to 29)), high-income North America (19% (95% UI 14 to 25)) and Western Sub-Saharan Africa (14% (95% UI 11 to 17)) showed the most increasing significant trends, while Southern Sub-Saharan Africa (−12% (95% UI −15 to −8)), high-income Asia-Pacific (−7% (95% UI −10 to −4)) and Eastern Sub-Saharan Africa (−5% (95% UI −8 to −2)) showed decreasing significant trends (table 1 and online supplementary figure 2). The number of prevalent cases was found to be doubled from 1990 (10 226 042 (95% UI 9 320 195 to 11 179 199)) to 2017 (19 965 114 (95% UI 17 990 489 to 21 955 673)) but the contribution of GBD 2017 regions was different (see online supplementary figure 3).
Supplemental material
Supplemental material
East Asia (26% (95% UI 23 to 30)), high-income North America (22% (95% UI 18 to 28)) and North Africa and Middle East (13% (95% UI 10 to 15)) had the top statistically significant increasing trends in age-standardised incidence rates whereas statistically significant decreasing trend was found in Southern Sub-Saharan Africa (−11% (95% UI −14 to −8)), high-income Asia-Pacific (−10% (95% UI −14 to −7)) and Eastern Sub-Saharan Africa (−9% (95% UI −12 to −6)) (table 1 and online supplementary figure 2). The number of incident cases was also found to be doubled from 1990 (650 269 (95% UI 589 738 to 711 375)) to 2017 (1 204 599 (95% UI 1 071 089 to 1 331 694)) with differing contribution of GBD 2017 regions (see online supplementary figure 3).
The top three statistically significant increasing trends in age-standardised DALY rate belonged to high-income North America (13% (95% UI 8 to 18)), Western Sub-Saharan Africa (10% (95% UI 1 to 18)) and Tropical Latin America (9% (95% UI 5 to 13)). Southern Sub-Saharan Africa (−29% (95% UI −35 to −22)), high-income Asia-Pacific (−28% (95% UI −34 to −23)) and Eastern Sub-Saharan Africa (−24% (95% UI −35 to −15)) were considered to have statistically decreasing trend in age-standardised DALY rate among GBD 2017 regions (table 1).
National level
Age-standardised prevalence rate of RA ranged from 91 to 471 cases per 100 000 population. The UK (471.8 (95% UI 428.9 to 514.9)), Trinidad and Tobago (404.4 (95% UI 362.6 to 446.6)) and Barbados (402.6 (95% UI 361.1 to 445.3)) had the three highest age-standardised prevalence rates in 2017, whereas Indonesia (91.1 (95% UI 81.1 to 101.8)), Timor-Leste (91.4 (95% UI 81.5 to 102.4)) and Sri Lanka (97.2 (95% UI 85.9 to 109.6)) showed the lowest rates (figure 1 and online supplementary table 2).
Supplemental material

Age-standardised prevalence rate of rheumatoid arthritis per 100 000 population in 2017, by country. ATG, Antigua and Barbuda; BRB, Barbados; COM, Comoros; DMA, Dominica; FJI, Fiji; FSM, Federated states of Micronesia; GRD, Grenada; KIR, Kiribati; LCA, Saint Lucia; MDV, Maldives; MHL, Marshall Islands; MLT, Malta; MUS, Mauritius; SGP, Singapore; SLB, Solomon Islands; SYC, Seychelles; TLS, Timor-Leste; TON, Tonga; TTO, Trinidad and Tobago; VCT, Saint Vincent and the Grenadines; VUT, Vanuatu; WSM, Samoa (generated from data available from ghdx.healthdata.org/gbd-results-tool/).
Age-standardised incidence rates varied from 5.6 to 27.5 cases per 100 000 population. UK (27.5 (95% UI 24.7 to 30.0)), Ireland (23.7 (95% UI 21.0 to 26.4)) and Sweden (23.4 (95% UI 21.0 to 25.8)) showed the highest age-standardised incidence rates in 2017; in contrast, Indonesia (5.6 (95% UI 4.9 to 6.3)), Timor-Leste (5.7 (95% UI 5.1 to 6.4)) and Sri Lanka (5.9 (95% UI 5.2 to 6.7)) had the lowest rates (figure 2 and online supplementary table 3).
Supplemental material

Age-standardised incidence rate of rheumatoid arthritis per 100 000 population in 2017, by country. ATG, Antigua and Barbuda; BRB, Barbados; COM, Comoros; DMA, Dominica; FJI, Fiji; FSM, Federated states of Micronesia; GRD, Grenada; KIR, Kiribati; LCA, Saint Lucia; MDV, Maldives; MHL, Marshall Islands; MLT, Malta; MUS, Mauritius; SGP, Singapore; SLB, Solomon Islands; SYC, Seychelles; TLS, Timor-Leste; TON, Tonga; TTO, Trinidad and Tobago; VCT, Saint Vincent and the Grenadines; VUT, Vanuatu; WSM, Samoa (generated from data available from: ghdx.healthdata.org/gbd-results-tool/).
The percentage change in age-standardised prevalence rates from 1990 to 2017 differed substantially between countries, with Canada (54.7% (95% UI 49.2 to 59.7)), Paraguay (41.8% (95% UI 35.0 to 48.6)) and Guatemala (37.0% (95% UI 30.9 to 43.9)) showing the largest increases. In contrast, South Africa (−16.6% (95% UI −20.3 to −13.0)) Sweden (−15.7% (95% UI −19.9 to −11.4)) and Burundi (−15.6% (95% UI −19.5 to −11.1)) showed decreasing trends (see online supplementary table 2).
Supplemental material
The percentage change in age-standardised incidence rates (from 1990 to 2017) also differed between countries. The largest increases were seen in Canada (48.2% (95% UI 41.5 to 55.1)), Paraguay (43.6% (95% UI 36.6 to 50.7)) and Guatemala (36.8% (95% UI 30.4 to 44.3)). The largest decreases during this period were found in Burundi (−17.0% (95% UI −21.1 to −12.5)), Ethiopia (−16.6% (95% UI −20.1 to −13.6)) and Sweden (−16.2% (95% UI −20.3 to −11.9)) (see online supplementary table 3). The national-level detailed information on DALYs due to RA can be found in online supplementary table 4.
Age and sex patterns
Globally, age-standardised prevalence rate was higher in females and increased with age, peaking at 70–74 and 75–79 age groups among females and males, respectively in 2017. Also, the number of prevalent cases increased with age and peaked in the 60–64 age group for both males and females; after this age, the trend declined (figure 3). In 2017, the global age-standardised incidence rate was also found to be higher in females and increased with population ageing but there was no statistically significant difference between males and females in the 70+ age groups. The number of incident cases reached the highest level at 50–54 age group then a declining trend was observed to the oldest group (see online supplementary figure 4). The pattern of age-standardised DALY rate by sex across the age groups was relatively similar to the age-standardised prevalence rate (see online supplementary figure 5). Decomposition of DALY rate into YLL and YLD also showed that the YLL rate was significantly lower than YLD up to 70–74 age group. Moreover, it was found 60–64 and 65–69 age groups had the highest number of YLD and YLL, respectively (see online supplementary figure 6).
Supplemental material
Supplemental material
Supplemental material

Global number of prevalent cases and prevalence rate of rheumatoid arthritis per 100 000 population by age and sex, 2017; dotted and dashed lines indicate 95% upper and lower uncertainty intervals, respectively
Burden of RA by SDI and HAQ
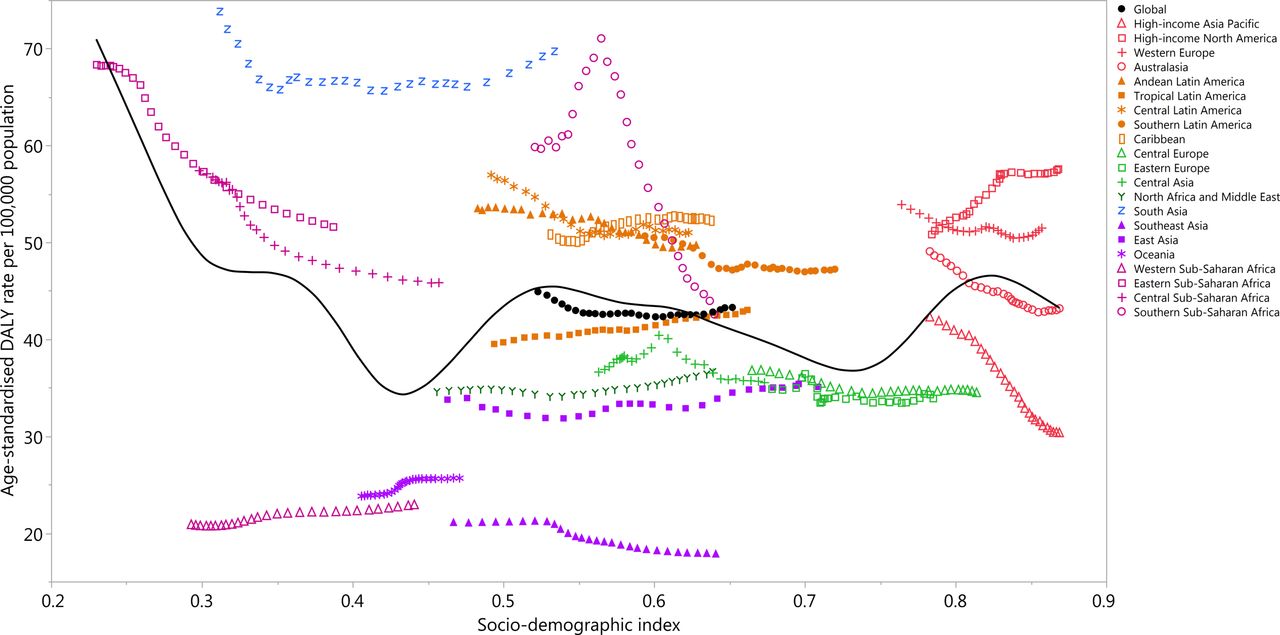
At the regional-level, a non-linear association was found between the age-standardised DALY rate and the SDI. The lowest age-standardised DALY rate was seen at an SDI of around 0.43; it then increased and decreased intermittently with SDI improvement (figure 4). In the high-income super region, only high-income North America showed an increasing level during 1990–2017. Despite a declining trend in Western Europe, this region still showed a higher than expected level of age-standardised DALY rate during the measurement period. In the Latin-America super-region, Caribbean and Tropical Latin America showed increasing trend during 1990–2017 and all regions had higher than expected level of age-standardised DALY rate in the recent 6 years. Central Europe, Eastern Europe, Central Asia, North Africa and Middle East, Southeast Asia, East Asia and Oceania had lower than expected age-standardised DALY rates during 1990–2017. Finally, in the Sub-Saharan Africa super-region, only Western Sub-Saharan Africa showed lower than expected age-standardised DALY rate during 1990–2017 (figure 4).

Age-standardised DALY rates for rheumatoid arthritis for 21 Global Burden of Disease (GBD) regions by Socio-Demographic Index (SDI), 1990–2017; expected values based on SDI and disease rates in all locations are shown as the black line. Twenty-eight points are plotted for each GBD region and show observed age-standardised DALY rates from 1990 to 2017 for that region. DALY, disability adjusted life year
National-level analysis found there was a non-linear association between age-standardised DALY rate and SDI and the high burden of RA was not limited to the most developed or less developed countries. UK, India, Pakistan, Nepal, Honduras, Barbados, Trinidad and Tobago and many other countries showed much higher than expected level of age-standardised DALY rates. In contrast, Singapore, Malaysia, Sri Lanka, Vietnam, Timor-Leste showed and many other countries showed much lower than expected age-standardised DALY rates (figure 5). The association of age-standardised DALY rates and countries’ HAQ also was also non-linear (see online supplementary figure 7).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Age-standardised DALY rates of rheumatoid arthritis by 195 countries and Socio-Demographic Index, 2017; expected values are shown as the black line. Each point shows observed age-standardised DALY rate for specified country in 2017. DALY, disability adjusted life year.
Discussion
In this paper, we presented the prevalence, incidence and DALY counts and age-standardised rates for RA in 195 countries from 1990 to 2017, as reported in GBD 2017. Globally, there were almost 20 million prevalent cases, 1.2 million incident cases and 3.4 million DALYs. These data serve to highlight the significant, yet under-recognised, global burden of RA.
A previous systematic review on RA prevalence found that regional crude prevalence rates were 400 for Southeast Asia, 370 for the Eastern Mediterranean, 620 for Europe, 1250 for North America, and 420 for the Western Pacific.4 While estimates from this review could not be directly compared with the GBD 2017 estimates, it is clear that North America and the Eastern Mediterranean are consistently among the highest regions in terms of prevalence. In GBD 2010,7 RA was found to be responsible for 4.8 million DALYs in 2010, which is higher than the updated GBD 2017 estimates. This difference may in part be explained by additional data sources and new methodologies applied in GBD 2017. The global prevalence of RA was similar between GBD 2010 and GBD 2017, at 240 per 100 000 population.7 The crude DALYs for RA was higher in 2017 than in GBD 2013 (45.7 vs 37.6).8
The GBD 2017 data showed that the age-standardised prevalence and incidence rates have increased during the period 1990 to 2017 but age-standardised DALY rate decreased by 3.6%. An 11.6% increase in crude DALY rate from 1990 to 2013 has been reported8; whereas, GBD 2017 found that the crude DALY rate increased by 25% during 1990–2017. Other studies have not investigated the trend of age-standardised rate of prevalence, incidence and DALYS comprehensively and hence, findings cannot be compared.20 21
Differences in incidence and prevalence in regions that are within the same super-region should be noted. South Asia, which includes Bangladesh, India, Nepal, Bhutan and Pakistan, is among the regions with the highest incidence and prevalence of RA, yet South-East Asia, including Cambodia Myanmar and Thailand among others, is among the lowest incidence and prevalence rates globally.
GBD 2017 also showed that age-standardised prevalence and DALY rates were higher in females and increased with age and peaked at 70–74 and 75–79 age groups among females and males, respectively. Moreover, the age-standardised incidence rate was also found to be higher in females and increased with age, but there was no statistically significant difference between males and females in those aged over 70 years. The prevalence rate of RA across age groups was also examined in the previous studies and prevalence rates have reported to be higher in females than males4 7 8; but the association between prevalence rate and age and sex such as the monotonic positive association of prevalence rate with age found in prior studies7 were not similar to the GBD 2017 findings.
It must be noted that the data presented here were primarily derived from modelled data through the processes in DISMOD-MR 2.1. True population-based national data on incidence and prevalence of RA were available from very few countries, thus the present study relies on modelling. As such, these national estimates should be interpreted with caution. Greater inclusion of musculoskeletal conditions, including RA, is encouraged in national health data collections.
To the best of our knowledge, the associations of prevalence, incidence and DALYs due to RA with developing status of region and countries have not been examined in the previous studies and the present study has some important findings. First, the association between burden of RA and SDI should not be assumed to be simplistic and linear; GBD 2017 showed a complex and non-linear association. In fact, burden of RA is not limited to developed or less developed countries and a high burden of RA was reported in countries with various SDI. Second, the global burden of RA has reached higher than expected levels during recent years and awareness of the importance of early identification and treatment should be encouraged in the countries with high incidence, prevalence and DALY rates to reduce future burden. Third, the effectiveness of prevention programmes should not be only judged based on the observed values but also the expected levels in each region and country need to be addressed.
One of the approaches in prevention programme is to focus on risk factors. However, previous observational studies found only smoking to be clearly associated with RA.12 Although some risk factors such as genetic factors, hormones, stress, obesity, infections, gut bacteria and diet have been studied but the findings have been inconclusive. Smoking, as one of the important risk factors, need to be monitored precisely and specific prevention programme need to be applied in each country. According to a previous study,22 the global age-standardised prevalence of daily smoking decreased by 28.4% and 34.4% in men and women since 1990, respectively. This study also shows the pace of progress as a function of geographies, development status and sex is heterogeneous. Greater success in tobacco control can be achieved through using effective and comprehensive policies introduced in previous papers.23 24
Effective treatment of RA needs a policy and health service response, such as the WHO Global Strategy, which aims to develop and maintain functional ability that enables well-being in older age. In areas where there is problematic access to specialists, delayed diagnosis of RA may impede the effective treatment of RA and difficulties adhering to treat-to-target principles that aim to prevent RA-related disability by reducing disease activity and achieving remission. Early diagnosis and treatment prevent progression of joint damage in 90% of patients with early RA,25 and increased levels of remission can be gained from effective early treatment with more complex disease modifying and biological drugs that are currently available,25 although with their higher cost, this is primarily in high-income regions. However, greater awareness is needed of RA burden and dissemination of knowledge of the large body of evidence of the important improvements in morbidity and mortality that can be achieved with early clinical diagnosis and treatment with relatively low-cost drugs such as methotrexate.26–28 With this early treatment of RA, the adverse consequences and increasing burden of RA can be prevented.
Conclusions
RA is a major global public health challenge; however, the burden of RA varies geographically. The age-standardised prevalence and incidence rates are overall increasing globally. Increasing population awareness regarding RA, its risk factors and the importance of early diagnosis and treatment with disease modifying agents is warranted to reduce the future burden of this condition. Improving health data for better monitoring of disease burden and health outcomes are strongly suggested.
Supplemental material
Acknowledgments
We would like to thank Institute for Health Metrics and Evaluation staff and its collaborators who prepared these publicly available data. Also, we would like to thank Social Determinants of Health Research Center of Shahid Beheshti University of Medical Sciences for financial support under reference 19406.
References
Footnotes
Handling editor Josef S Smolen
Correction notice This article has been corrected since it published Online First. The first and tenth affiliations have been updated.
Contributors SS, AAK, LM and MC designed the study. SS, AAK, MAM, AA-H, AA-A and MQ analysed the data and performed the statistical analyses. SS, AAK, DB and MC drafted the initial manuscript. All authors reviewed the drafted manuscript for critical content. All authors approved the final version of the manuscript.
Funding The GBD study is funded by Bill and Melinda Gates Foundation, however these were not involved in any way in the preparation of this manuscript. The present report was also supported by Social Determinants of Health Research Center, Shahid Beheshti University of Medical sciences, Tehran, Iran (No. 19406).
Disclaimer This study is based on publicly available data and solely reflects the opinion of its authors and not that of the Institute for Health Metrics and Evaluation.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (IR.SBMU.RETECH.REC.1398.161).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository.