Article Text

Abstract
Objectives Several population-based studies on systemic lupus erythematosus (SLE) have been reported, yet community-based, individual-case validated, comprehensive reports are missing. We studied the SLE epidemiology and burden on the island of Crete during 1999–2013.
Methods Multisource case-finding included patients ≥15 years old. Cases were ascertained by the ACR 1997, SLICC 2012 criteria and rheumatologist diagnosis, and validated through synthesis of medical charts, administrative and patient-generated data.
Results Overall age-adjusted/sex-adjusted incidence was 7.4 (95% CI 6.8 to 7.9) per 100 000 persons/year, with stabilising trends in women but increasing in men, and average (±SD) age of diagnosis at 43 (±15) years. Adjusted and crude prevalence (December 2013) was 123.4 (113.9 to 132.9) and 143 (133 to 154)/105 (165/105 in urban vs 123/105 in rural regions, p<0.001), respectively. Age-adjusted/sex-adjusted nephritis incidence was 0.6 (0.4 to 0.8) with stable trends, whereas that of neuropsychiatric SLE was 0.5 (0.4 to 0.7) per 100 000 persons/year and increasing. Although half of prevalent cases had mild manifestations, 30.5% developed organ damage after 7.2 (±6.6) years of disease duration, with the neuropsychiatric domain most frequently afflicted, and 4.4% of patients with nephritis developed end-stage renal disease. The ACR 1997 and SLICC 2012 classification criteria showed high concordance (87%), yet physician-based diagnosis occurred earlier than criteria-based in about 20% of cases.
Conclusions By the use of a comprehensive methodology, we describe the full spectrum of SLE from the community to tertiary care, with almost half of the cases having mild disease, yet with significant damage accrual. SLE is not rare, affects predominantly middle-aged women and is increasingly recognised in men. Neuropsychiatric disease is an emerging frontier in lupus prevention and care.
- epidemiology
- incidence
- prevalence
- lupus nephritis
- neuropsychiatric lupus
Statistics from Altmetric.com
Introduction
Systemic lupus erythematosus (SLE) is a complex autoimmune disease with chronic relapsing-remitting nature.1 Clinical-epidemiological research has advanced our knowledge; however, most reports are based on tertiary care data, which often provide conflicting or non-generalisable results.2 3 Updated, comprehensive information at the community level may contribute to realising the disease’s unmet needs and unravel the role of genetic and environmental factors.4
To address the need for accurate data on the epidemiology of the disease, we established the Lupus Registry ‘Leto’. The main objectives of the study were (1) to obtain population-based estimates of SLE incidence and prevalence in individuals residing in Crete during 1999–2013, and (2) to describe the main clinical features, including trends of severe disease manifestations (lupus nephritis (LN), neuropsychiatric lupus) and outcomes (organ damage).
Methods
Source population and setting
Crete, the fifth largest southernmost island in the Mediterranean, provides an advantageous setting to study complex diseases such as SLE. First, it is geographically isolated with a relatively closed, genetically homogeneous population of approximately 0.65 million and low migration/translocation rates. Second, it comprises both urban (>15 000, 39% of the inhabitants) and rural (61% of the inhabitants) areas (2011 National Census, http://www.statistics.gr/en/statistics/pop). Third, the healthcare system is mixed public/private and patients can visit a specialist without a general practitioner’s referral, but typically even patients with mild SLE are not followed exclusively at primary care. There is a single rheumatology clinic, at the University Hospital of Iraklio, with expertise in SLE since 1990, which serves as referral centre and has strong connections to primary/secondary care units (including private rheumatologists) involved in lupus diagnosis and care, thus resulting in low rate of patients seeking medical care outside Crete.
Case-finding and patient recruitment
This is an ongoing programme that started in 2012. The present study involved an initial retrospective research of potential cases from 1990 until 2011 (irrespective of the year of their diagnosis), coupled with a prospective active surveillance (2012–2015). To ensure data completeness, we included in the study incident and prevalent SLE cases from 1999 to 2013 (thus extending our surveillance period by another 2 years).
Multiple case-finding sources were used (online supplementary figure S1). Our primary source was the medical charts of the rheumatology clinic. More than 10 000 paper records were screened for SLE and related diagnoses (‘incomplete lupus’, ‘possible lupus’, ‘lupus-like’ and ‘undifferentiated connective tissue disease’). Second, the programme was communicated to nephrology and dermatology departments across the island, so that they provided access to data (eg, biopsies archives) and referred patients who had never been evaluated by us. Third, we communicated with all private rheumatologists to possibly detect milder cases followed at the community. Furthermore, the Arthritis Foundation of Crete endorsed a campaign to inform patients and the public.
Supplementary file 2
Patients who were identified were recruited (on their visit at the clinic, referred by the collaborative network of physicians or by email/telephone in case of no regular follow-up). On enrolment to the registry, they were administered with a structured questionnaire after signing informed consent. Interviews were performed by trained personnel.
Complementary data were retrieved from hospital databases (discharges, laboratory tests) queried for relevant International Classification of Diseases-9 codes and the National Renal Data System for end-stage renal disease (ESRD). These sources also provided mortality data.
Database registry establishment, variables and information synthesis
For each potential case, dedicated personnel reviewed all available paper and electronic files. The ACR 19975 and Systemic Lupus International Collaborating Clinics (SLICC) 20126 classification criteria, validated activity (SLE Disease Activity Index 20007) and organ damage (SLICC/ACR Damage Index (SDI)8) items were recorded from the medical charts, and the respective indexes were calculated. SLE was characterised as mild, moderate or severe based on the British Isles Lupus Assessment Group-defined9 severity of disease manifestations, medications received and physician’s global assessment. LN was defined according to kidney biopsy and/or the classification criteria. The SDI definition of ESRD was used.8 Diagnosis of neuropsychiatric SLE (NPSLE) (ie, attributed to the disease) was according to the ACR definitions,10 following multidisciplinary approach and validated with attribution models.11 12 Time-relevant data included dates of SLE diagnosis, any previous diagnoses and dates for major clinical features and score items described above. From the questionnaires, we gathered detailed data on demographics, residence, family and personal history, disease manifestations, body mass index (BMI) and tobacco use. All data/variables were entered into a database to enable cross-checking and information synthesis.
SLE definitions and case ascertainment (validation)
Primary analyses were based on cases that fulfilled the ACR 1997 criteria during the period 1999–2013. Secondary analyses used rheumatologist-based and SLICC 2012 criteria-based diagnoses. Cases were counted as incident at the year the diagnosis clearly reported for the first time in patient’s medical records and/or the fourth criterion was fulfilled. To count a case (incident or prevalent) for a specific calendar year, a patient had to reside in Crete at least 1 year before and be over 15 years old. Patients who died still counted as prevalent in the same year of death but not in the ensuing year(s). Drug-induced and cutaneous-only lupus were excluded. The relevant flow chart is shown in online supplementary figure S1.
Statistical analysis (see also online supplementary material13–15)
Supplementary file 1
Age-specific, sex-specific and region-specific denominators were based on National Census (2001, 2011). Interim population estimations generated by the Hellenic Statistical Authority were publicly distributed (Thessaly University, http://www.e-demography.gr). Crude and stratum-specific average annual incidence and prevalence with 95% CIs were calculated. Age-standardised and gender-standardised rates for SLE, LN and NPSLE were calculated with the direct method using the European Standard Population as a reference.
Study approval
The study was approved by the Ethics Committee of the University Hospital of Iraklio.
Results
Increasing incidence of SLE during the period 1999–2010
The overall crude and age-adjusted/sex-adjusted incidence rate of SLE (ACR 1997-based) in Crete during 1999–2013 was 8.6 (95% CI 8.0 to 9.0) and 7.4 (95% CI 6.8 to 7.9) per 100 000 persons/year, respectively. The incidence female-to-male ratio was 13:1. There was an increase in SLE incidence during the years 1999–2010, which stabilised afterwards (figure 1A). This trend was observed in both genders, but in men the increase continued until the end of the study period (online supplementary table S1).
Supplementary file 3

Incidence of SLE, lupus nephritis and NPSLE according to 3-year intervals during the period 1999–2013. (A) Age-adjusted and sex-adjusted incidence of SLE (ACR 1997 definition) per 100 000 persons/year. (B) Age-adjusted and sex-adjusted incidence of lupus nephritis per 100 000 persons/year. (C) Age-adjusted and sex-adjusted incidence of NPSLE per 100 000 persons/year. ACR, American College of Rheumatology; NPSLE, neuropsychiatric SLE; SLE, systemic lupus erythematosus.
Incidence of severe SLE: stable rates of LN but increasing trends of NPSLE
We next focused on severe forms of SLE, namely LN and NPSLE. Overall age-adjusted/sex-adjusted incidence of LN during 1999–2013 was 0.6 (95% CI 0.4 to 0.8) per 100 000 persons/year, corresponding to incidence rates of 1.0 (95% CI 0.7 to 1.3) and 0.2 (95% CI 0.1 to 0.4) per 100 000 persons/year in women and men, respectively. Rates of incident nephritis remained stable (figure 1B). Adjusted NPSLE (cerebrovascular disease, seizures and cognitive dysfunction being the most frequent manifestations) incidence rates in the total, female and male population were 0.5 (95% CI 0.4 to 0.7), 0.8 (95% CI 0.5 to 1.1) and 0.3 (95% CI 0.1 to 0.4), respectively. Temporal trends of incident NPSLE resembled those of SLE, that is, increasing during 1999–2010 and remaining stable afterwards (figure 1C). Detailed rates per calendar year are presented in online supplementary table S1. The female-to-male ratio of incident nephritis and NPSLE cases was 4.2:1 and 3:1, respectively.
Earlier onset of LN and NPSLE in male than female patients
The mean (±SD) age at the time of SLE diagnosis was 43 (±15) years (range 9–81), with a peak at the age group 45–54 years for both men and women (figure 2A). LN occurred earlier in men than in women, with most cases diagnosed at 15–24 vs 45–54 years, respectively (figure 2B). In NPSLE, the peak age of diagnosis was also lower in men than in women (35–44 vs 45–54 years) (figure 2C).

Incidence of SLE, lupus nephritis and NPSLE across different age groups (period 1999–2013). (A) Crude incidence rates (per 100 000 persons/year) of SLE. (B) Crude incidence rates (per 100 000 persons/year) of lupus nephritis. (C) Crude incidence rates (per 100 000 persons/year) of NPSLE. NPSLE, neuropsychiatric SLE; SLE, systemic lupus erythematosus.
Increasing prevalence of SLE, LN and NPSLE
There was a steady increase in crude SLE prevalence (ACR 1997-defined) from 22 (95% CI 18 to 26) in 1999 to 143 (95% CI 133 to 154) per 100 000 individuals aged ≥15 years old in 2013. The age-adjusted/sex-adjusted prevalence was 18.7 (95% CI 14.8 to 22.6) in 1999 and 123.4 (95% CI 113.9 to 132.9) per 100 000 in 2013. The increasing trend was noted in both genders (online supplementary table S2).
Supplementary file 4
Crude prevalence of LN in 2013 was 14.4 (95% CI 11.1 to 17.6) per 100 000, which corresponds to prevalence of 24.1 (95% CI 18.1 to 29.9) and 4.3 (95% CI 1.8 to 6.8) (per 100 000) in women and men, respectively. We examined the possibility of missing LN cases and found that the number of prevalent cases (n=90) approximated the median number of expected patients with LN according to capture–recapture for all sources (89.5, 95% CI 73.0 to 105.9) and the Bayesian model-derived estimate of prevalent LN cases (86, 95% CI 83 to 89). As for NPSLE, crude prevalence in the total, female and male population was 9.7 (95% CI 7.0 to 12.3), 14.9 (95% CI 10.3 to 19.5) and 4.3 (95% CI 1.8 to 6.9) per 100 000, respectively. Both prevalence of nephritis and NPSLE increased during the study period (twofold and sixfold, respectively).
Similar trends in SLE incidence and prevalence using different case definitions
To validate our findings, we estimated the disease occurrence using alternative case definitions. Time trends in SLE incidence were similar according to ACR 1997, SLICC 2012 classification criteria and physician diagnosis (figure 3). Incident cases were defined by rheumatologist diagnosis on average 3 months earlier than with the ACR 1997 criteria, and by the ACR 1997 criteria on average 3 months earlier than the SLICC 2012 criteria. Within cases who fulfilled both the ACR 1997 criteria and rheumatologist-based diagnosis, 68% had the diagnosis by these two definitions in the same year; in 22%, clinical diagnosis preceded that of ACR 1997 criteria and in the remaining 10% the ACR-based diagnosis preceded the clinical one. The respective percentages were 70%, 19% and 11% for the comparison of SLICC 2012 criteria against rheumatologist-based diagnosis, and 87%, 5% and 8% for the comparison of ACR 1997 against SLICC 2012 criteria. By use of any of the three definitions, SLE prevalence estimates demonstrated a steady increase during 1999–2013 (figure 4).

Incidence of SLE (per 100 000 persons/year) according to 3-year intervals (period 1999–2013) based on three case definitions (ACR 1997 criteria definition, rheumatologist-based definition and SLICC 2012 criteria definition). ACR, American College of Rheumatology; SLE, systemic lupus erythematosus; SLICC, Systemic Lupus International Collaborating Clinics.

Annual prevalence of SLE (per 100 000 persons/year) during the period 1999–2013 based on three case definitions (ACR 1997 criteria definition, rheumatologist-based definition and SLICC 2012 criteria definition). ACR, American College of Rheumatology; SLE, systemic lupus erythematosus; SLICC, Systemic Lupus International Collaborating Clinics.
Demographic and clinical features of prevalent cases: higher disease severity in male patients
The ACR 1997-based prevalent population (December 2013) comprised 750 patients and was sociodemographically homogeneous: 97% Greek, 93% women, 81% married, 70% with <12 years of education and 80% with Cretan descent (defined as past three generations). The mean disease duration was 7.2 (±6.6) years. Of the patients, 68.4% had disease duration longer than 5 years. Current smoking and obesity (BMI >30 kg/m2) were each found in 30% of the patients.
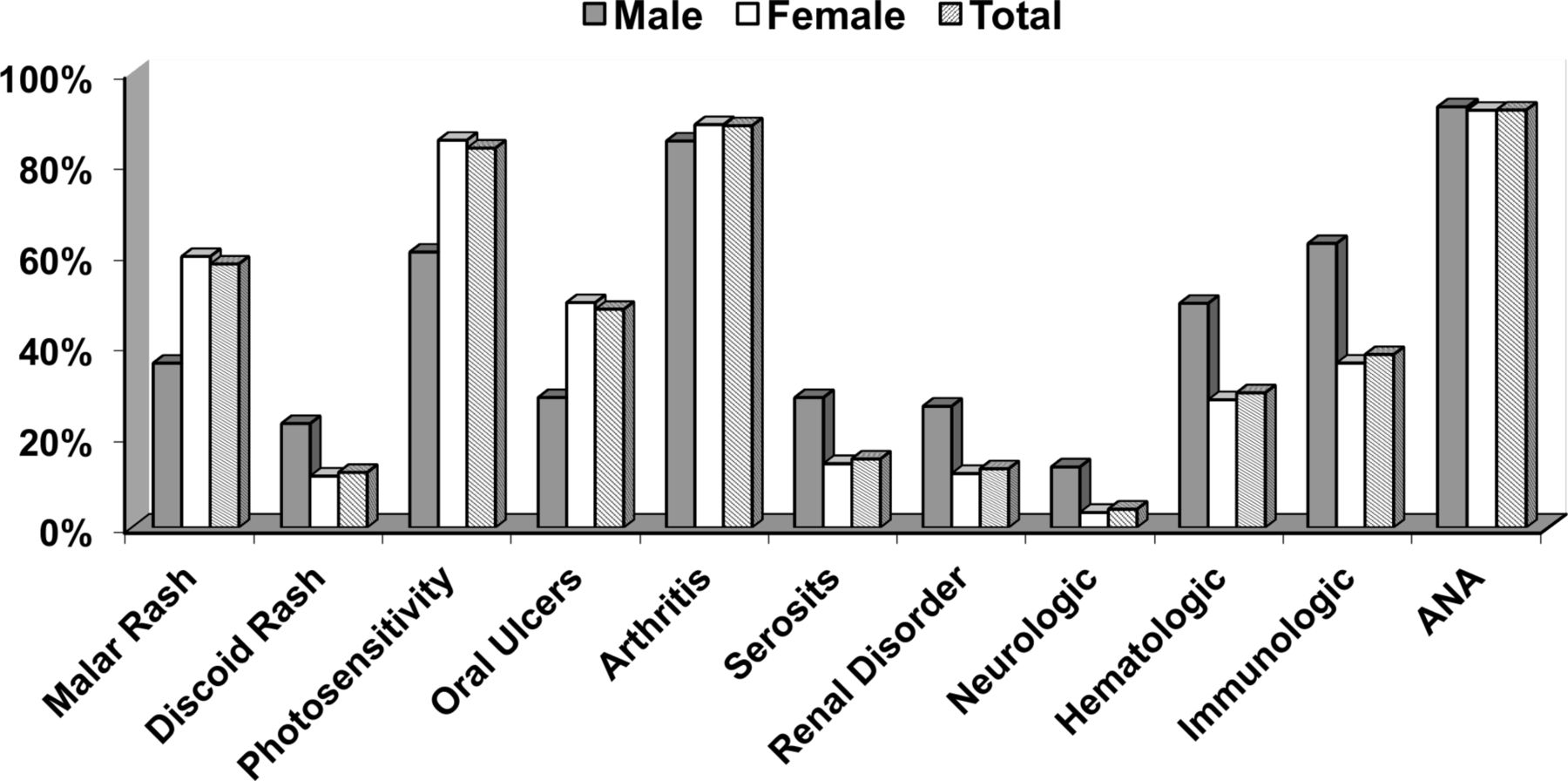
The most frequent clinical features (cumulative incidence of ACR 1997 criteria) were arthritis and mucocutaneous manifestations (figure 5). The following manifestations occurred more frequently in men versus women: serositis (28% vs 14%, p<0.001), renal involvement (26.4% vs 11.8%, p<0.001), neurological manifestations (13.3% vs 3.3%, p<0.001) and haematological abnormalities (47.2% vs 28.0%, p<0.001). Based on the severity of manifestations and the use of lupus treatments, the disease was classified as mild, moderate and severe in 50%, 33% and 17% of all prevalent SLE cases. Of the patients, 14.8% had received azathioprine or mycophenolate, 9% cyclophosphamide and 3.6% rituximab. In total, 34% of the moderate/severe cases had received potent immunosuppressive drugs. Significantly more men than women displayed moderate (30.2% vs 25.8%) or severe (34.0% vs 13.5%) forms of SLE (p<0.001 for both comparisons).

Clinical and serological manifestations in the 750 prevalent SLE cases (year 2013) (ACR 1997 criteria definition). ACR, American College of Rheumatology; SLE, systemic lupus erythematosus.
Significant organ damage develops early in the disease course
Data for organ damage, assessed by the SDI (score range 0–46; 0=no damage, 1–2=moderate damage, ≥3= severe damage),16 17 were available in 613 patients. On the year of diagnosis, 84.0% of patients with SLE were free of damage, whereas 12.6%, 2.9% and 0.5% had SDI scores of 1, 2 and 3, respectively. Three years after diagnosis, the respective percentages were 76.7%, 18.3%, 3.8% and 1.3% (figure 6A). At last follow-up, 30.5% of patients with prevalent SLE had organ damage (figure 6B). Men had more damage than women: 28% vs 18% (p<0.003) on the year of diagnosis, 34% vs 22% (p<0.005) after 3 years and 38% vs 30% (p<0.005) at last follow-up. The most frequent component of the SDI was the neuropsychiatric items (cognitive impairment, seizures, cerebrovascular accident), followed by the musculoskeletal and malignancy items (figure 6C). Within the subgroup of patients with LN, 4.4% developed ESRD.

![[SP2.jpg]](https://ard.bmj.com/content/annrheumdis/76/12/1992/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Non-reversible organ damage in patients with prevalent SLE. (A) Frequency of organ damage (assessed by the SDI) in prevalent SLE cases at the time of diagnosis and after 3 years. Results are from 613 patients with available data at both time points. No deaths occurred during this time period. (B) Frequency of organ damage (SDI) in prevalent SLE cases at last follow-up. (C) Individual damaged domains (SDI) in prevalent SLE at last follow-up. ACR, American College of Rheumatology; SDI, SLICC/ACR Damage Index; SLE, systemic lupus erythematosus; SLICC, Systemic Lupus International Collaborating Clinics.
Discussion
By employing a comprehensive methodology, from primary to tertiary care, we describe high SLE occurrence in Crete. Our incidence is higher than estimates from Nordic countries and Europe,18 although lower than ethnic minorities’ rates in the UK,19 USA20 and elsewhere.3 21 The observed adjusted incidence rates (7.4/105 persons/year) exceed those from previous decade in Greece (1.90/105 persons/year, 1982–2001).22 Likewise, our prevalence estimates are higher than those previously reported in Greece (5023–11024 per 100 000). Together, our findings concord with recent estimates suggesting that SLE should no longer be considered a rare disease (average threshold of 40 cases/10525).
We found an increase in SLE incidence in our region during 1999–2010, which stabilised thereafter. Relevant reports worldwide21 are conflicting and suggest increasing trends in USA26 27 and Greece,22 decreasing in Spain28 and UK,29 or stable in Norway and Denmark.30 31 Increases during the previous decades (1950–1990) were attributed to wider use and improvements in antinuclear antibodies (ANA) testing and diagnosis of milder cases.27
In our study, the observed rise might be—at least partially—explained by better disease awareness and recognition. Incomplete case-finding or ascertainment during the early years might also be possible, thus leading to ‘inflation’ of cases. To address this, we compared disease severity, use of potent immunosuppressive/biological drugs and organ damage in incident cases across three consecutive periods (1999–2003, 2004–2008 and 2009–2013) and found no differences in ratios (online supplementary table S3).
Supplementary file 5
The possible effect of environmental factors on the increase cannot be excluded. In Crete, there was a profound urbanisation during the previous decades both in terms of people migrating to larger cities and also in lifestyle changes. Circumstantial evidence suggests increased or increasing prevalence among adults in the general population of Crete in factors such as westernised diet and lifestyle,32 vitamin D deficiency (severe in 21%33) and smoking (44% among parents of preschool children34), which all could contribute to SLE increase. Notably, and in agreement with other studies,22 35 SLE was more prevalent in urban than rural regions, a result that deserves more detailed investigation.
The increasing prevalence of SLE in our region concords with worldwide trends.21 Besides increased incidence, this may be explained also by improved survival. Unfortunately, detailed mortality data were not available especially for the first decade of the observation period, and this is a limitation. Nonetheless, during the more recent 5 years for which we had more accurate data, we had only nine deaths, suggesting a low risk of survival bias.
Our incidence of LN (0.6 per 100 000/year) is higher than those in the UK,36 Denmark37 and Norway38 (ranging from 0.40 to 0.45 per 100 000/year). Accordingly, prevalence of LN in Crete in 2013 (14.4 per 100 000) is higher than in the UK (5.6 per 100 000 white individuals in 2001)36 and Denmark (6.4 per 100 000 in 2011),37 but lower than in white US Medicaid-enrolled adults (15.8 per 100 000).20 Regarding NPSLE, epidemiological studies are scarce and results are variable.39 Herein, we provide, for the first time, sex-adjusted/age-adjusted incidence and prevalence estimates for NPSLE, and demonstrate increasing trends during 1999–2010, possibly due to better awareness and increasing use of neuroimaging.
By using rheumatologist diagnosis, the ACR 1997 and SLICC 2012 criteria for case definition, we noted concordant time trends in SLE (figures 3–4). There were differences in the timing of diagnosis with physician-based preceding criteria-based diagnosis in about 20% of cases. At the end of 2013, fewer patients with SLE had been classified with the SLICC 2012 than with the ACR 1997 criteria. Preliminary data suggest that this is largely due to lack of inclusion of photosensitivity and of malar rash in the former, which agrees with a previous report.40
Although direct comparisons are difficult, one could argue SLE in our region has some characteristics suggestive of less severe disease as compared with North/Latin America or other parts of Europe.41 42 This can be extrapolated by the lower prevalence of nephritis (13%), NPSLE (7.8%), anti-DNA autoantibodies (23% by Crithidia luciliae), organ damage (30.5%) and the increased prevalence (50%) of mild disease forms. In accordance, ESRD rate was 4.4%, which is lower than elsewhere (typically 10%–15% after 5 years).43–45 Alamanos et al also reported a milder SLE profile in northern Greece due to lower prevalence of nephritis (15% at diagnosis) and lower standardised mortality ratio.22 46 These findings could be attributed to genetic/ethnicity factors, although differences in the methodology, particularly the fact that our study is representative of SLE at the community, may be important. In addition, a theoretical risk for survival bias could have influenced the prevalence of severe cases, but we do not consider this significant, in view of the small number of observed deaths and the stable ratio of mild/severe disease over the study period (3.80, 4.17 and 3.85 across the three consecutive 5-year periods; online supplementary table S3).
Our study has several strengths; it included multiple sources to ensure data completeness and reliability.47 48 Demographics (including residence history) were determined from self-reports and not exclusively from administrative data.4 Case validation was performed through chart review and in-person interviews,4 further contributing to data reliability and integrity.49 The use of alternative case definitions facilitated disease ascertainment. Although this is a referral centre study, we adopted a community-based method, which avoids selection biases.50
One of the study limitations is that capture–recapture methods were not used in the total SLE population. LN cases followed exclusively in nephrology departments may have received care outside our capture area hospitals and are more likely to have been missed. Accordingly, we used capture–recapture analysis in this particular group, showing no missing cases. Although our study was regional, Crete is inhabited by 6.5% of the total Greek population, and due to the homogeneity of the ethnicity/race and the infrequency of extreme socioeconomic differences our estimate might approach the national estimate.
In conclusion, our project offers robust, updated estimates of SLE occurrence and burden. Alike other studies, we document that SLE frequency may be higher than previously considered. These results confirm that SLE is not rare, affecting also older ages and being increasingly recognised in men. Our data corroborate previous findings on the increased burden of NPSLE among whites, which represents an unmet need. Despite milder phenotype in the community as compared with tertiary centres, a considerable proportion of patients develop severe disease requiring immunosuppressive therapy and accrue organ damage, emphasising the need for optimisation of early diagnosis and management.
Acknowledgments
We would like to acknowledge the following collaborators who participated in the case-finding, recruitment or data collection for the Leto registry: Nestor Avgoustidis, MD; Nikos Kougkas, MD; Marilena Mamoulaki, MD; Ioannis Kallitsakis, MD; Ioannis Katzakis, MD; Eleni Kouroumali, MD; Eleni Fragkouli, MD; Ioannis Papalopoulos, MD; Niki Lydataki, MD; Eleni Kteniadaki, MD; Manolis Papastefanakis, MSc; Konstantinos Stylianou, MD; Stavros Stratakis, MD; and Garyfallia Perysinaki, MD. Also, the authors wish to thank the Arthritis Foundation of Crete for the support, especially Katerina Koutsogianni, Argyro Stara and Foteini Ksomeritaki for helping in patient recruitment, and finally the staff of the Rheumatology Clinic, especially Eleni Krasoudaki, MD, Maria Terizaki, Giota Rapsomaniki, Antzela Kountouri and Stella Polia (research nurses) and Mary Adamaki, who graciously facilitated the medical records archiving activities.
References
Supplementary materials
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2018 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
DTB and GKB contributed equally.
Contributors IG conducted the study, performed research and face interviews; AF, AR, CA and AP examined and interviewed patients; MT and IT provided data on lupus nephritis patients; GS established and maintained the SLE database; EK arranged patients visits and delivered questionnaires; LC supervised the methodology; AB performed the statistical analysis; PS examined patients and supervised the study; GKB and DTB conceived the study and supervised the study; GKB and IG drafted the manuscript.
Funding This work was implemented by the Greek General Secretariat of Research and Technology ‘Aristeia’ action of the Operational Programme ‘Education and Lifelong Learning’, and was co-funded by the European Social Fund (ESF) and National Resources (Aristeia I 2344 to DTB).
Competing interests None declared.
Patient consent Obtained.
Ethics approval University Hospital of Iraklio.
Provenance and peer review Not commissioned; externally peer reviewed.