Article Text

Abstract
Lupus nephritis (LN) occurs in 50%–60% of patients with childhood-onset systemic lupus erythematosus (cSLE), leading to significant morbidity. Timely recognition of renal involvement and appropriate treatment are essential to prevent renal damage. The Single Hub and Access point for paediatric Rheumatology in Europe (SHARE) initiative aimed to generate diagnostic and management regimens for children and adolescents with rheumatic diseases including cSLE. Here, we provide evidence-based recommendations for diagnosis and treatment of childhood LN. Recommendations were developed using the European League Against Rheumatism standard operating procedures. A European-wide expert committee including paediatric nephrology representation formulated recommendations using a nominal group technique. Six recommendations regarding diagnosis and 20 recommendations covering treatment choices and goals were accepted, including each class of LN, described in the International Society of Nephrology/Renal Pathology Society 2003 classification system. Treatment goal should be complete renal response. Treatment of class I LN should mainly be guided by other symptoms. Class II LN should be treated initially with low-dose prednisone, only adding a disease-modifying antirheumatic drug after 3 months of persistent proteinuria or prednisone dependency. Induction treatment of class III/IV LN should be mycophenolate mofetil (MMF) or intravenous cyclophosphamide combined with corticosteroids; maintenance treatment should be MMF or azathioprine for at least 3 years. In pure class V LN, MMF with low-dose prednisone can be used as induction and MMF as maintenance treatment. The SHARE recommendations for diagnosis and treatment of LN have been generated to support uniform and high-quality care for all children with SLE.
- corticosteroids
- disease activity
- lupus nephritis
- systemic lupus erythematosus
- treatment
Statistics from Altmetric.com
Introduction
In 2012, the Single Hub and Access point for paediatric Rheumatology in Europe (SHARE) initiative was launched with the aim to optimise and disseminate diagnostic and management regimens for children and adolescents with rheumatic diseases, including childhood-onset systemic lupus erythematosus (cSLE).1 cSLE is rare, with a prevalence of 1.9–25.7 per 1 00 000 children and incidence of 0.3–0.9 per 1 00 000 children-years worldwide.2–4 cSLE in general has a more severe phenotype than adult-onset disease.5–8 Fifty to sixty per cent of patients with cSLE will develop lupus nephritis (LN).5–8 Timely and accurate recognition of renal involvement combined with appropriate treatment choices will optimise clinical outcome and decrease renal-associated morbidity and mortality.1
Consensus treatment recommendations for proliferative LN in children are available,9 10 but do not include a paediatric-specific systematic literature review, nor do they focus on recommendations regarding diagnosis of LN or treatment in non-proliferative LN.
SHARE recommendations for paediatric antiphospholipid syndrome, juvenile dermatomyositis, familial Mediterranean fever and auto-inflammatory diseases have been published.11–14 SHARE recommendations for diagnosis and treatment of cSLE (excluding LN) have also been published.15 Here, the SHARE recommendations for LN are presented. These recommendations will support clinicians caring for children with or without suspected LN in carrying out a stepwise diagnostic process and guide them in treatment decision-making.
Methods
SHARE is a European Union (EU)-funded project; therefore, representative paediatric rheumatologists from across Europe formed a panel of 16 members, with representation of paediatric nephrology. Disease experts from outside the EU also contributed to the project. The European League Against Rheumatism (EULAR) standardised operating procedures for developing best practice recommendations were followed.16
Systematic literature search and study selection
A systematic literature search, based on specific research questions was performed in the electronic databases PubMed/MEDLINE, EMBASE and Cochrane in July 2013 (see online supplementary table S1), using a validated filter to search articles pertaining to children and adolescents only.17 All titles and abstracts were screened independently by two reviewers (NG, NdG). Articles fulfilling the inclusion criteria were sent to the experts for validity assessment and data extraction (see online supplementary table S2). While the literature search included terms regarding cSLE generally and paediatric antiphospholipid syndrome (APS), these topics are discussed separately.14 18 Here, we report the LN-specific studies identified.
Supplementary file 1
Validity assessment
All articles were analysed by the expert panel (two reviewers per article), using standardised data extraction and scoring forms. Any discrepancies were resolved by a third expert (SK or MWB) to reach consensus. Adapted classification tables for diagnostic19 and therapeutic20 studies were used to determine the level of evidence and strength of each recommendation16 (see online supplementary tables S3 and S4).
Establishment of recommendations
Based on this evidence base, provisional statements regarding diagnosis and treatment of LN were formulated (NG, NdG, SK, MWB). Adult-derived literature was consulted if no evidence in children was found. Provisional statements were presented to the expert committee (n=15) in an online survey (100% response rate). Recommendations were revised according to responses and discussed at two sequential face-to-face consensus expert meetings in March 2014 (Genova, n=16) and March 2015 (Barcelona, n=14). Nominal group technique was used to reach consensus,21 where final recommendations were formulated. Recommendations were accepted when a predefined >80% of the experts agreed.
Results
Literature review
Figure 1 summarises the literature review. The initial search yielded 9341 articles regarding diagnosis, treatment and management of cSLE. After screening title and abstract, and assessing full texts for relevance, 55 articles were used (see online supplementary table S5).

Summary results from the systematic literature review. cSLE, childhood-onset systemic lupus erythematosus; LN, lupus nephritis; NP, neuropsychiatric.
Recommendations for LN—diagnosis
Renal symptoms that could be indicative of LN include: renal dysfunction (acute kidney injury, acute-on-chronic kidney disease), hypertension, macroscopic or microscopic haematuria and/or proteinuria. Proteinuria is not always related to LN. Orthostatic proteinuria or postural proteinuria is the most common cause of proteinuria in teenagers, and should therefore be excluded as a cause of mild proteinuria in patients with (suspected) cSLE.22 23 Confirmation and classification of renal involvement with consultation with paediatric nephrologist is recommended, proceeding to a percutaneous renal biopsy (table 1).
Recommendations for LN—diagnosis
The International Society of Nephrology/Renal Pathology Society (ISN/RPS) 2003 classification system is commonly used to classify LN9 24 (see online supplementary table S6). Studies using the ISN/RPS classification system showed that class of nephritis is associated with severity of renal disease and long-term renal outcome. Therefore, treatment strategies were based on the ISN/RPS 2003 classification system.25 26
Assessment of renal biopsies can be challenging. A renal pathologist experienced in LN should be consulted for biopsy evaluation.27 Even so, misclassification of a renal biopsy is possible. For example, patients diagnosed with class I or II LN should not generally have proteinuria after 3 months of treatment. If proteinuria persists after 3 months, the possibility of misclassification of the biopsy or progression to class III or IV LN must be considered.28 To avoid unnecessary repeat biopsy, the expert group recommends re-evaluating the initial biopsy as a first step.
Recommendations for LN—treatment
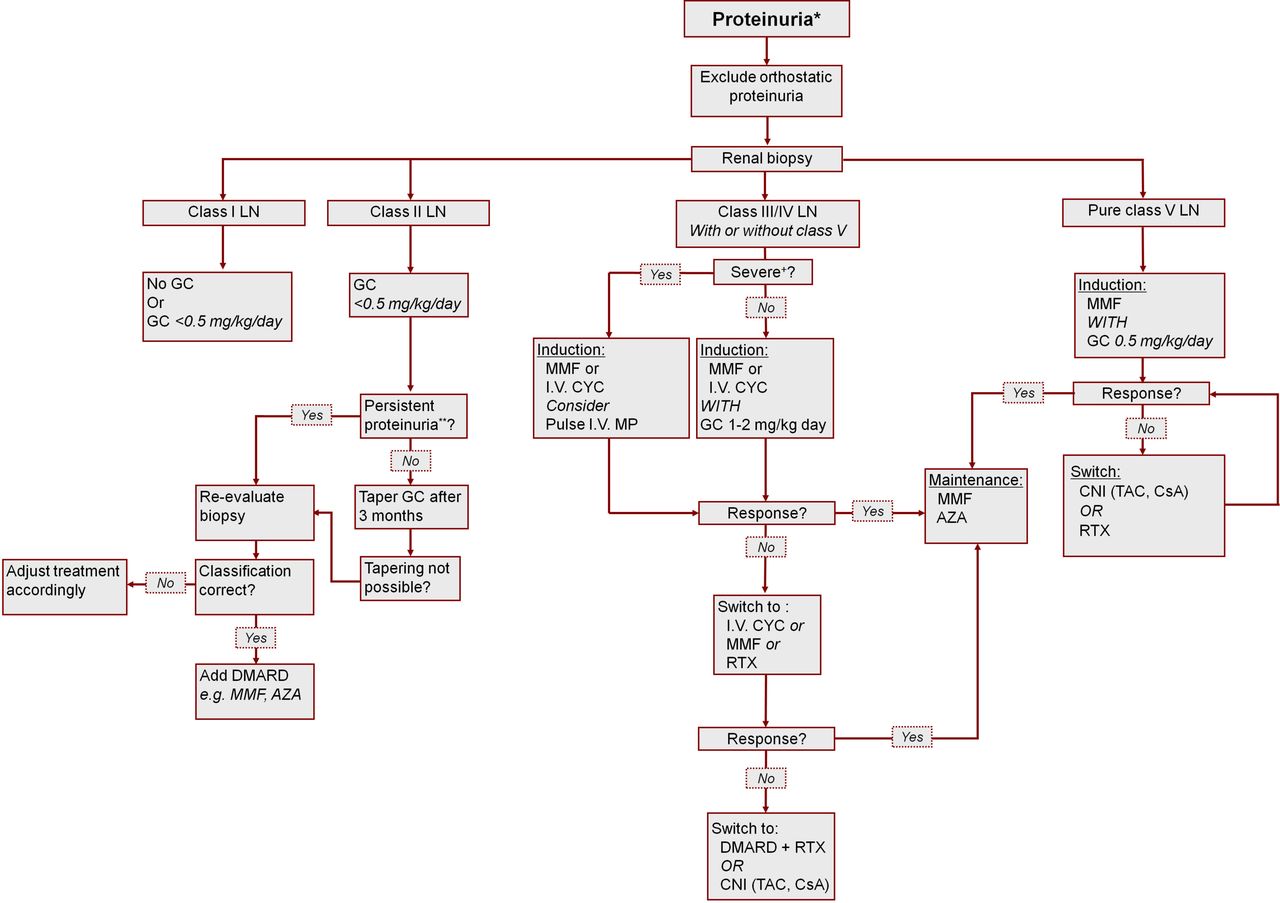
As clinical symptoms are not reliable enough to reflect severity of renal disease, a renal biopsy is needed to guide treatment strategy. Treatment strategies for the different classes of LN are discussed in table 2 and summarised in figure 2. Renal biopsy is not always possible (eg, critical clinical condition; lack of resources to safely perform the procedure). As nephrotic syndrome, hypertension and impaired renal function are all correlated with class III/IV LN,29–31 these symptoms should be considered as reflecting class III/IV LN and treated likewise if renal biopsy cannot be performed.
Recommendations for LN—treatment

{kind=link}
{kind=link}
Treatment strategies for the different classes of LN definitions: *proteinuria: 0.5 g/24 hour or UP:CR >50 mg/mmol in a urine sample; **persistent proteinuria: presence of proteinuria for >3 months; DMARD: MMF, AZA, CNI, intravenous CYC; +severe disease, eg, impaired eGFR, estimated glomerular filtration rate (<80 mL/min/1.73 m2), nephrotic range proteinuria (>1 g/m2/day), biopsy-proven crescentic glomerulonephritis. AZA, azathioprine; CNI, calcineurin inhibitors; CsA, ciclosporin; CYC, cyclophosphamide; DMARD, disease-modifying antirheumatic drug; GC, corticosteroids; LN, lupus nephritis as classified by the ISN/RPS 2003 classification system; MMF, mycophenolate mofetil; MP, methylprednisolone; RTX, rituximab; TAC, tacrolimus.
The long-term aim for treatment of LN should be complete renal response, with early morning urine protein:creatinine ratio (UP:CR) of <50 mg/mmol (or urine albumin:creatinine ratio of <35 mg/mmol) and normal renal function (estimated glomerular filtration rate >90 mL/min/1.73 m2). Within 6–12 months after initiation of treatment, partial renal response, defined as ≥50% reduction in proteinuria to at least subnephrotic levels and normal or near-normal renal function should be achieved.9 Degree of proteinuria at baseline was not a statistical significant predictor of renal function deterioration among patients with (membranous) LN, and herewith is not a decisive factor for specific treatment strategies.32–36
Several studies have reported on the antiproteinuric effect of ACE-inhibitors (ACE-I) or angiotensin-II receptor blockers (ARB) in renal disease. Evidence in patients with adult-onset SLE shows that these inhibitors of the renin-angiotensin system have a protective effect on the kidneys in case of proteinuria.37 38 Additional treatment with ACE-I and/or ARB in children with LN and proteinuria should be advocated, guided by consultation with a paediatric nephrologist. Notably, the use of hydroxychloroquine is recommended in all patients with cSLE.15
ISN/RPS class I and II LN
Although class I LN is more common in cSLE compared with adult-onset SLE, no specific articles on treatment of class I LN were identified. Based on adult literature and consensus, class I LN could be treated with low-dose oral corticosteroid therapy.39 If other organ systems are involved and class I LN has been found, treatment choice should be guided by these other clinical features. If class I LN is the only clinically active feature, adding other disease-modifying antirheumatic drugs (DMARDs) is generally not necessary (table 2, figure 2).
Class II LN generally responds well to low-dose oral corticosteroid therapy, tapered over a 3–6 months period (starting dose 0.25–0.5 mg/kg/day, maximum of 30 mg/day; often 0.25 mg/kg/day is sufficient). If proteinuria is persistent after 3 months or corticosteroid dose cannot be effectively weaned, renal biopsy should be re-evaluated by an experienced renal pathologist to exclude misclassification. Adding a DMARD to the treatment or switching to another DMARD effective for LN (eg, MTX to AZA) is recommended (table 2, figure 2).40–42 Notably, if treatment of class II LN remains unchanged despite the lack of renal response or prednisone dependency, renal impairment or even renal failure may develop.43 There is little evidence for a specific DMARD in class I/II LN. Only case series or cohorts with limited number of patients are available and report the use of, mycophenolate mofetil (MMF), tacrolimus and cyclophosphamide (CYC) with variable effects.44–46
ISN/RPS class III and IV LN with or without class V LN
Class III and IV LN (proliferative LN) are the most common and severe forms of LN in cSLE.6 29 30 47–49 Combination of class III or IV LN with class V LN is prevalent. As class III and IV LN generally show a less favourable disease course than class V LN, treatment strategies advised for proliferative LN should be followed in case of combined class III or IV with class V LN.
Induction treatment of ISN/RPS class III and IV LN with or without ISN/RPS class V LN
In adults, evidence for induction treatment of class III and IV LN is based on several randomised controlled trials (RCT).50 51 Equal efficacy and toxicity ratios are present for low-dose intravenous CYC (in adults: fixed dose 500 mg/pulse, six pulses given every 2 weeks), and high-dose CYC (500–750 mg/m2/pulse, if tolerated increase to 750 mg/m2/pulse, maximum dose 1000–1200 mg/pulse, 6 monthly pulses), adjusting appropriately in cases of renal dysfunction.50 When comparing high-dose intravenous CYC with MMF (in adults: starting 1000 mg/day, increase to maximum dose 2000–3000 mg/day), renal outcomes were similar.51 Recently, a network meta-analysis including only RCTs investigated comparative efficacy and toxicity of multiple treatment regimens for induction and/or maintenance treatment of proliferative adult-onset LN. This concluded that induction treatment with MMF, calcineurin inhibitors (CNIs) or a combination thereof, when added to corticosteroids, were the most effective treatments compared with intravenous CYC.52
In cSLE, there are no RCTs on this topic but several observational cohort studies and case series describe treatment of class III/IV LN. Intravenous CYC is generally used as induction treatment, with good results in most patients.53–61 Three studies compared intravenous CYC induction therapy with azathioprine (AZA) in proliferative LN, one including patients with acute renal failure at diagnosis, showing similar efficacy.55 57 59 Notably, patients with acute renal failure at diagnosis had excellent renal outcome.57
When comparing MMF with intravenous CYC in 13 patients with class III LN, complete or partial remission was achieved by more patients in the MMF group than in the intravenous CYC group.60 MMF is well tolerated as induction treatment.62 Initial MMF monotherapy combined with ciclosporin after 4 weeks has been shown to be safe and effective therapy after 12 months follow-up for 16 patients.63
When considering these adult and cSLE-derived data, the consensus group concluded that MMF (standard dose 1200 mg/m²/day, maximum 2000 mg/day; when poor response option to increase to maximum of 1800 mg/m²/day, maximum dose 3000 mg/day, but toxicity increases with higher dose) or intravenous CYC combined with high-dose prednisone (1–2 mg/kg/day, maximum 60 mg/day) should be considered for induction treatment of proliferative LN in cSLE.10 50–68 The dosing of intravenous CYC (high or lower-dose, see above) is left to the discretion of the treating physician. The toxicity profile of MMF is more favourable when compared with intravenous CYC and may be preferred for this reason. In case of suspected non-compliance to oral medication, intravenous CYC should be considered (table 2, figure 2).51 66 Notably, in contrast to high-dose, low-dose intravenous CYC does not seem to impact ovarian reserve as measured by anti-Mullerian hormone.69
Maintenance treatment of ISN/RPS class III and IV LN with or without ISN/RPS class V LN
RCT in adults demonstrate that both MMF and AZA are good options for maintenance treatment in class III and IV LN,64 65 70 71 although a higher relapse rate is seen in patients treated with AZA.64 65 71 Additionally, a recent network meta-analysis showed that MMF was the most effective strategy to maintain remission for proliferative LN.52
Studies of proliferative LN in cSLE show similar results for MMF and AZA. Some studies indicate better outcomes for MMF, others for AZA.55–57 59 60 62 63 72 73 The expert group therefore advises to use MMF (dosing: see above) or AZA (2–3 mg/kg/day, maximum 150 mg/day) as maintenance treatment for LN. Of note, AZA is associated with a higher flare risk in a meta-analysis of adult LN RCT.70 Intravenous CYC can be effective as maintenance treatment,53–55 58 59 61 72 73 but is not advised due to higher toxicity when compared with MMF or AZA (eg, increased risk of a reduced ovarian reserve/premature ovarian failure, inhibition of spermatogenesis, increased risk of bladder carcinoma).74
Duration of maintenance treatment in LN in the cSLE from the literature search was variable (1–5 years). Adult proliferative LN RCT studying maintenance therapy treated patients up to 3 years with good results.65 71 The expert panel agreed that adopting this time frame was the best strategy, while accepting additional supportive evidence is necessary (table 2, figure 2).
Corticosteroid use in ISN/RPS class III/IV LN
Corticosteroids are generally used concomitantly with induction/maintenance regimen for class III/IV LN. Comparative studies regarding corticosteroid dose and oral versus intravenous use are not available. EULAR/European Renal Association–European Dialysis and Transplant Association (ERA-EDTA) and American College of Rheumatology (ACR) guidelines for treatment of proliferative LN in adult-onset SLE, recommend intravenous methylprednisolone pulse therapy in the initial treatment strategy, followed by oral prednisone (0.5–1 mg/kg/day) and tapered to the minimal amount necessary to control disease. This recommendation is based on expert opinion and extrapolation from controlled studies.9 75 The Childhood Arthritis and Rheumatology Research Alliance (CARRA), a North American-based research collaboration specifically for paediatric rheumatic diseases, have provided consensus treatment plans for induction therapy of proliferative LN in cSLE.10 These plans include three different dosing regimens combining oral corticosteroids with intravenous methylprednisolone-pulses based on expert opinion and by evidence from gene-expression arrays suggesting that intravenous methylprednisolone pulses but not oral prednisone have the potential to eliminate the interferon-alpha gene expression signature in cSLE.10 However, no clinical data available reports that eliminating the interferon-alpha gene expression signature is associated with better renal outcomes.
As there is no robust evidence for the ideal dosing strategy of corticosteroids in proliferative LN, the expert group has not specified this in a recommendation. Most studies in cSLE report the use of oral prednisone 1–2 mg/kg/day (maximum 60 mg/day) as initial dosing in proliferative LN where children <30 kg mostly are dosed up to 2 mg/kg/day.46 55 56 60 61 73 Intravenous methylprednisolone pulse therapy (30 mg/kg/dose intravenous for three consecutive days, maximum 1000 mg/dose) may be added to induction treatment before start of oral prednisone, especially in case of severe disease (eg, impaired GFR (<80 mL/min/1.73 m2); nephrotic range proteinuria (>3.5 g/24 hours); biopsy-proven crescentic glomerulonephritis). An example for a prednisone-tapering schedule that may be used is tapering by 10%–20% at 1-week or 2-week interval based on clinical improvement.50 51 66 71
ISN/RPS class V LN
When comparing the use of corticosteroids with intravenous CYC with corticosteroids alone, combination therapy was superior in the only RCT for adults with pure class V LN available.32 A pooled analysis of patients with pure class V LN included in two RCTs showed that MMF was equally efficacious when compared with intravenous CYC as induction treatment.33 Patients with class V LN with or without class III or IV LN were also included in RCT for LN in adults, showing no difference between the use of MMF or high-dose intravenous CYC as induction treatment.66 Evidence for treatment strategies in the literature search for children with class V LN was very limited. Good renal outcome has been shown in a cohort (n=30, 90% achieved renal remission as defined by the ACR76) of cSLE with pure class V LN. Thirty-three per cent of the total cohort were treated with DMARDs (AZA/ciclosporin/MMF).77
When combining the evidence of adult-onset SLE and cSLE, the expert group recommends the use of MMF in combination with low-dose oral prednisone (0.5 mg/kg/day) as induction treatment for pure class V LN in cSLE. MMF or AZA are recommended as maintenance treatment. CNI (ciclosporin, tacrolimus), rituximab or intravenous CYC are recommended as alternative options or for non-responders, with consideration of their respective toxicity profiles32 33 51 77 (figure 2, table 2).
Renal flares and refractory disease
In general, in a patient not responding to the prescribed treatment as expected or developing disease flare, medication non-compliance should first be explored. Lack of adherence to therapy can be as high as 50%, and has been associated with higher persistent disease activity and poorer renal outcomes.78–81 Measuring medication (trough) levels to unmask non-compliance is advisable.15 RCTs in adult LN have shown that time is needed to reach complete renal response for at least 3–6 months.51 However, if a patient shows hardly any response within 3 months of induction treatment, it is generally accepted to change the principle induction agent.
Renal flares can occur in up to 50% of patients with cSLE during maintenance treatment.49 82 83 After excluding non-compliance, restarting or increasing corticosteroid dose (oral prednisone or intravenous methylprednisolone pulses) and a switch of DMARD should be considered. Defining renal response criteria or other outcomes of renal disease was outside the scope of these recommendations. In persistent active or refractory cases of lupus nephritis class III and IV, with or without class V LN, treatment should be changed to another therapeutic agent. For example, when treating with MMF this should be changed to rituximab or intravenous CYC. Adherence must be re-assessed and dosing of current treatment must be optimised first. Two RCTs in adults testing rituximab for LN did not reach their primary end point, and is not recommended as primary treatment for LN.84 85 However, in observational studies of LN in adults, rituximab has been successfully used as rescue treatment for refractory LN.86 87 There is limited evidence for the use of rituximab for LN in cSLE.45 56 An observational cohort study in cSLE reported the effects of rituximab treatment in 63 children, LN was the indication to start rituximab treatment in 36% of the patients. Rituximab was well-tolerated and improved disease activity in these children with a significant reduction in oral corticosteroid dose.88 The expert group recommends that rituximab should be considered in refractory LN, in addition to the DMARD currently used.
CNI (tacrolimus, ciclosporin) can be considered as a treatment option for LN in selected cases, although with the consideration of potential nephrotoxicity especially related to ciclosporin after long-term use.89
Discussion
Six recommendations regarding diagnosis and 20 recommendations regarding treatment for LN in children were accepted with >93% agreement among a European-wide group of cSLE experts, including paediatric nephrology.
Recommendations for treatment of LN in cSLE are available.9 10 The CARRA cSLE subcommittee have published consensus treatment plans for newly diagnosed class III and IV LN.10 These plans correspond well with the SHARE LN recommendations. Differences do exist, specifically regarding the use of concomitant corticosteroid use. The EULAR/ERA-EDTA have also published recommendations for management of adult and paediatric lupus nephritis. These recommendations mainly focus on evidence obtained in adult studies of LN. Notably, these recommendations underline the importance of a well-coordinated transition programme in the care for children with LN.9 The expert group fully supports this recommendation. As specific EULAR guidelines for transition programmes for young people with rheumatic diseases have been published,90 we have refrained from this subject in these SHARE guidelines.
The SHARE recommendations are the first to specifically focus on evidence in cSLE for diagnosis and treatment of all classes of LN using a systematic literature search. Evidence in cSLE was limited and the need for new high-quality studies in this field is clear.
In conclusion, the SHARE project has resulted in evidence-based recommendations for diagnosis and treatment of LN, to support uniform and high-quality care for all children with LN.
References
Footnotes
NG and NG contributed equally,
MWB and SK contributed equally.
Handling editor Tore K Kvien
Contributors SK and MB are senior authors. NW and SV designed the SHARE initiative. NG and NdG performed the systematic literature review, supervised by MB and SK. Validity assessment of selected papers was done by MWB, SK, TA, AR, IKP, BBM, CP. Recommendations were formulated by NG, MB and SK. The expert committee consisted of TA, BBM, PB, PD, IKP, PL, LM, SO, CP, AR, AvR, YU, NW, SK, MWB, SM, GK; they completed the online surveys and/or participated in the subsequent consensus meetings. NG, NdG, SK and MWB prepared the consensus meetings, and NG and NdG chaired the meetings and took minutes. AR and BF facilitated the consensus procedure using nominal group technique. NG, SK and MWB wrote the manuscript, with contribution and approval of all coauthors.
Funding EAHC; grant number 2011 1202
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.