Article Text

Abstract
Objectives To determine the causes of death and risk factors in systemic sclerosis (SSc).
Methods Between 2000 and 2011, we examined the death certificates of all French patients with SSc to determine causes of death. Then we examined causes of death and developed a score associated with all-cause mortality from the international European Scleroderma Trials and Research (EUSTAR) database. Candidate prognostic factors were tested by Cox proportional hazards regression model by single variable analysis, followed by a multiple variable model stratified by centres. The bootstrapping technique was used for internal validation.
Results We identified 2719 French certificates of deaths related to SSc, mainly from cardiac (31%) and respiratory (18%) causes, and an increase in SSc-specific mortality over time. Over a median follow-up of 2.3 years, 1072 (9.6%) of 11 193 patients from the EUSTAR sample died, from cardiac disease in 27% and respiratory causes in 17%. By multiple variable analysis, a risk score was developed, which accurately predicted the 3-year mortality, with an area under the curve of 0.82. The 3-year survival of patients in the upper quartile was 53%, in contrast with 98% in the first quartile.
Conclusion Combining two complementary and detailed databases enabled the collection of an unprecedented 3700 deaths, revealing the major contribution of the cardiopulmonary system to SSc mortality. We also developed a robust score to risk-stratify these patients and estimate their 3-year survival. With the emergence of new therapies, these important observations should help caregivers plan and refine the monitoring and management to prolong these patients’ survival.
- systemic sclerosis
- epidemiology
- cardiovascular disease
- pulmonary fibrosis
Statistics from Altmetric.com
Introduction
Systemic sclerosis (SSc) is a devastating disease that has a profound impact on life expectancy, reflected by a standardised mortality ratio of 3.5.1 Its discordant causes and predictors of death have been studied in mostly small samples from single institutions, limiting their application to new studies of epidemiology.1–10 Because the presentation and prognosis of SSc are highly heterogeneous, the identification of patients at high risk of death, who may benefit from close monitoring and early treatment, is crucial.
Among various methods available to determine the causes of death, the analysis of death certificates is considered robust,11 although it has been scarcely used in investigations of SSc, with no report after year 2000.12 The ongoing European Scleroderma Trials and Research (EUSTAR) is an international, multicentre, prospective registry managed by physicians (list of authors and online supplementary appendix 1) and organised centrally by its committee.13 This database offers a unique opportunity to study the natural history of the disease and predict outcomes through the prospective, standardised collection of multiple characteristics of patients with SSc. Since the first report based on 284 deaths among 5860 patients in 2010,14 the database has grown to >11 000, and the numbers of follow-up visits and deaths have increased accordingly.
Supplementary file 1
Our aim was to identify the specific causes of death and their respective incidence by reviewing all death certificates of patients presenting with SSc, collected in France between 2000 and 2011, using a multiple-cause-of-death analysis.15 16 We then examined the causes of death and associated factors to develop a risk score associated with overall mortality in the international EUSTAR sample.
Methods
Death certificates
All death certificates issued in France comply with the international standards of the WHO and are exhaustively collected by the ‘Centre d’épidémiologie sur les causes médicales de décès’ (Epidemiological Centre for the Medical Causes of Death — CépiDc) from the ‘Institut national de la santé et de la recherche médicale’ (National Health and Medical Research Institute — INSERM).17 In January 2015, we examined the certificates of all adults presenting with SSc (international classification of diseases (ICD)-10 code M34) who died between 1 January 2000 and 31 December 2011.
Statistical analysis
A multiple-cause-of-death analysis was performed allowing the retrieval of the death certificates, which listed SSc as the ‘underlying’ cause of death (UCD) and those which considered SSc as the ‘associated’ cause of death (ACD).16 18 19
Mortality rates were calculated by age group for the entire period from 2000 to 2011. Age-standardised mortality rates per 105 patients were calculated by a direct method, per year and for the study period, using the standard 2000–2011 population data of the European Union and the European Free Trade Association.
To measure the strength of association between SSc and the various causes of death, we calculated the observed number of deaths in relation to the expected number of deaths (O/E ratio), based on the proportional mortality rate for the same cause of death within the French general population between 2000 and 2011. An O/E >1 means an excess mortality associated with SSc.
The EUSTAR sample
We interrogated the EUSTAR database at the end of May 2014, providing information on 11 193 patients >18 years age, from 124 participating centres, fulfilling the 2013 criteria formulated for SSc by the American College of Rheumatology/European League Against Rheumatism.20 The structure of the database, the minimum essential data set and the inclusion criteria have been described in detail previously.13 Each participating centre obtained approval of the local ethics committee and all registered patients granted their informed consent. Among the 11 193 patients who underwent ≥1 visit, 7819 had ≥1 follow-up and 1072 died. Besides the disease characteristics and treatment, we recorded the date of death and whether the death was attributable to SSc or to another cause. Furthermore, we probed the participating centres with a view to identify a single pulmonary, cardiac, renal, infectious, neoplastic, gastrointestinal, suicidal or other primary cause of death, according to a standard set of definitions, and to record any clinically significant comorbidity in a brief additional form submitted to all centres where ≥1 patient death was entered in the database (online supplementary appendix 2).
Statistical analysis
Categorical results are presented as counts and percentages, and continuous variables as mean±SD.
Survival and prognostic score
The median (95% CI) follow-up was estimated by the reverse Kaplan-Meier method, and the overall survival by the Kaplan-Meier method. Potential prognostic factors were analysed first by the Cox proportional hazards regression model in single variable analysis. The proportional hazards assumption was verified by Schoenfeld residuals.21 Continuous variables were dichotomised according to the clinical cut-off.
To ascertain a possible linearity among the variables, the variance inflation factor was calculated, and the variables were considered colinear when >2.22 All factors emerging with p values <0.10 by single variable analysis were included in a multiple variable model and stratified by centre. Due to the multicollinearity and missing data for the former, the cutaneous form of the disease and muscle weakness were selected instead of the Rodnan score and muscle atrophy, respectively. A backward, stepwise variable selection algorithm was applied using a stopping rule based on a cut-off p value of 0.05. To account for missing observations, the data were analysed, using multiple imputations by chained equations, with 50 imputations obtained after 20 iterations.23 24 The variables considered in the imputation models were all the characteristics studied as prognostic factors, death status and Nelson-Aalen estimator of the cumulative hazard. In these variables, missing values ranged from 0% to 56.5%, with a median value of 2.0%. The results were aggregated by pooling the estimates obtained on each imputed data set according to Rubin’s rules. To develop the SCleroderma mOrtality p Eustar (SCOpE) prognostic score to use in clinical practice, we assigned points by rounding the beta values multiplied by 5 for the significant predictors, in order to obtain a minimal factor of 1.
The discriminative ability of the models was evaluated by the C-index after bootstrap correction for overoptimism, and by receiver operating characteristics (ROC) curve and area under the curve (AUC) for 3-year mortality. The models calibration was assessed by the calibration slope and the bootstrap, bias-corrected calibration slope at 3 years. The overoptimism induced by the models was corrected by multiplying the regression coefficients by the calibration slope.22 The 50 imputed data sets were internally validated by bootstrapping with random generation of 200 samples from the original data. This score was compared with the previous Bryan score using an ROC analysis.7
All tests were two-sided at a 0.05 significance level. The analyses were carried out using the R V.3.1.2 statistical software. Further details are in the online supplementary methods.
Results
Death certificates
Causes of death
Between 2000 and 2011, 6 474 953 adults died in France. SSc was listed in 2719 death certificates, including 1608 as UCD and 1111 as ACD, representing 0.04% of all death certificates issued during the study period (table 1). The mean age at the time of death was 71.4±12.8 years (online supplementary figure 1). The female/male (2157 female and 562 male) sex ratio was 3.8. The causes of death were cardiac in 31%, respiratory in 18%, infectious in 11% and cancers in 9% of cases (online supplementary table 1). Further information is in the online supplementary information.
Absolute number of deaths related to systemic sclerosis in France between 2000 and 2011
Mortality trends between 2000 and 2011
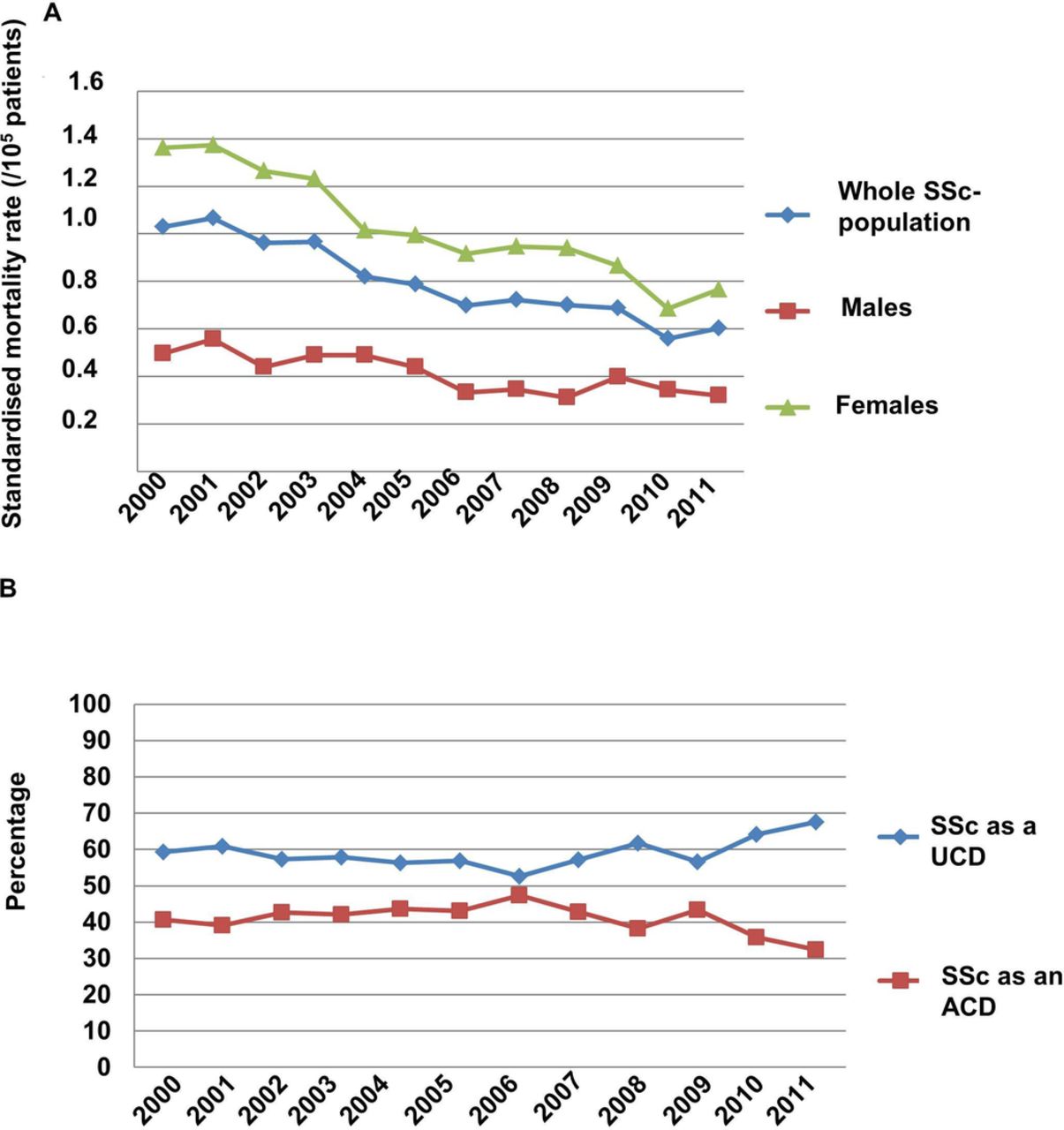
The overall, age-standardised mortality rate among patients with SSc was 0.80 per 105 individuals, with a female/male ratio of 2.49 (table 1). This rate decreased gradually from 1.03 per 105 men and women in year 2000, to 0.60 per 105 in year 2011 (figure 1A). The female-to-male ratio remained stable throughout the period. The ratio of deaths in which SSc was the UCD increased between 2000 and 2011, whereas the proportion of deaths in which SSc was the ACD decreased (figure 1B).
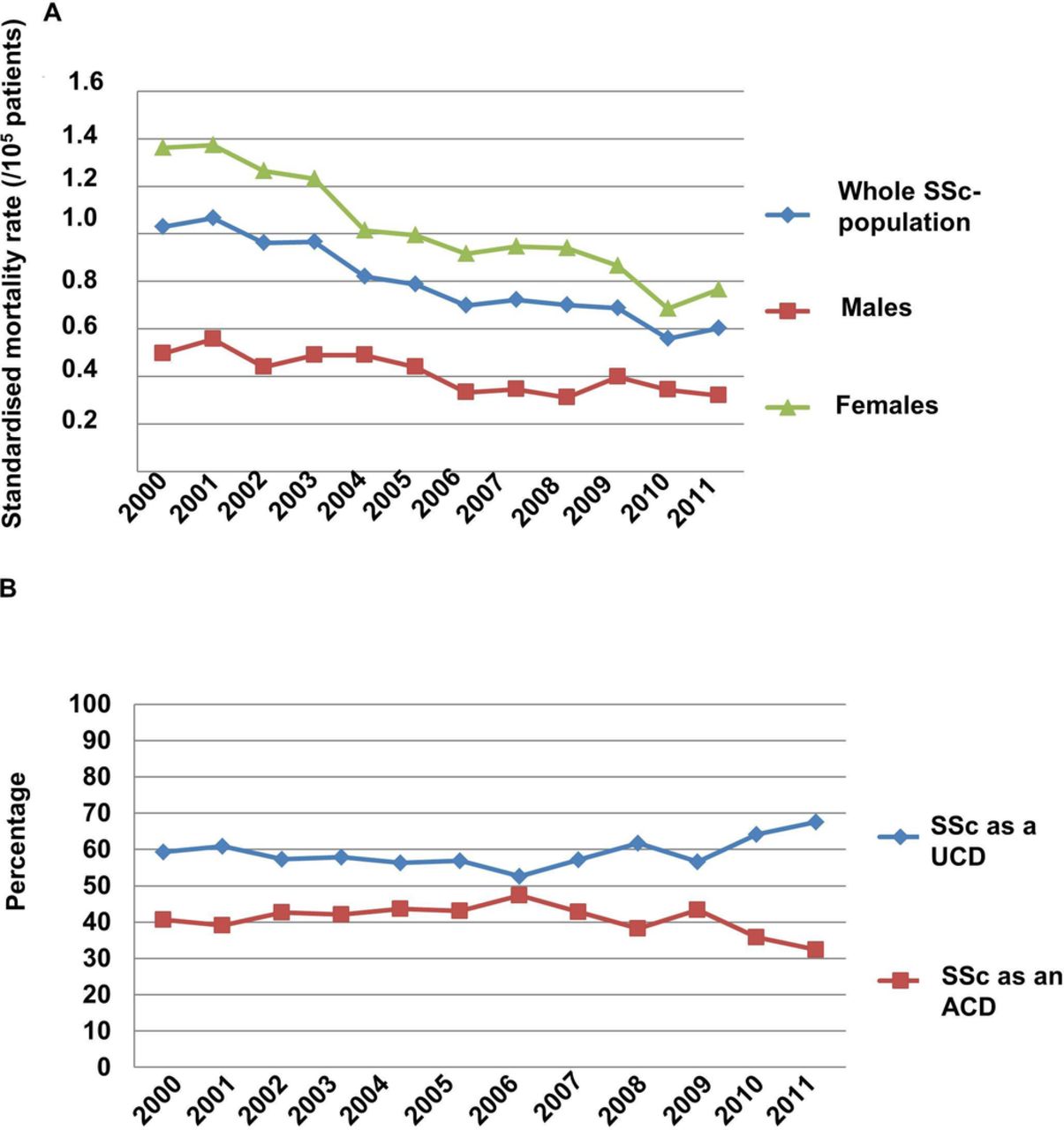
Deaths and systemic sclerosis in France between 2000 and 2011. (A) Age-standardised mortality per 105 men, women or both. (B) Percentage of deaths among patients presenting with systemic sclerosis (SSc) as the underlying cause of death (UCD) versus an associated cause of death (ACD).
Comparison of causes of death with the general population
The O/E ratios for cardiovascular, respiratory and infectious diseases were 1.36, 2.99 and 5.61, respectively, whereas the O/E for malignancy was 0.33. The excess mortality associated with respiratory diseases (O/E=3.77) was particularly prominent in men, while that associated with cardiovascular (O/E=3.14) and respiratory (O/E=9.50) diseases strongly involved patients <60 years (table 2).
(A) Sex-adjusted and age-adjusted O/E ratios for the cause of death in SSc and (B) age-adjusted O/E ratios for the cause of death in SSc
EUSTAR sample
Causes of death
A total of 11 193 patients with SSc were identified in the EUSTAR sample (online supplementary table 3). Of these, 86% were women, 31.0% presented with the diffuse cutaneous subtype and the mean disease duration was 8.1 years. Of these patients, 1072 (9.6%) died. The mean age at time of death was 63.6±13.4 years and the mean disease duration was 12.3±12.4 years (online supplementary figure 2). Death was considered SSc-related in 617 cases (57.6%) and unrelated to SSc in 270 cases (25.2%).
Supplementary file 3
Additional forms were completed for 940/1072 (87.7%) deaths by 64 participating centres (figure 2 and online supplementary table 3). The main causes of death were interstitial lung disease (ILD) (16.8%), pulmonary arterial hypertension (PAH) (14.7%), cancer (13.1%), primary heart disease (12.0%) and infection (9.1%). Further details are in the online supplementary information.

(A) Causes of death in the entire EUSTAR sample and in the limited and diffuse cutaneous forms. (B) Comparison of causes of death in the EUSTAR and in the death certificates samples. The results are presented as % of deaths. EUSTAR, European Scleroderma Trials and Research; PAH, pulmonary arterial hypertension; SSc, systemic sclerosis.
Predictors of death and prognostic score
Among 11 193 patients entered in the database, 7819 had ≥1 additional follow-up after the first visit (median follow-up: 2.3 (1.3–5.3) years). The disease characteristics of the patients with versus without ≥1 additional follow-ups were significantly dissimilar by single, though not by multiple variable analysis (online supplementary table 5). The 3-year survival rate (online supplementary figure 3) was 89.3% (88.5%–90.2%). The 39 variables associated with the 3-year mortality by single variable analysis are listed in online supplementary table 6. Online supplementary table 7 shows the description of the full model variables (1) according to the original data set (without imputation) and (2) averaged over all complete data sets (including the imputed data). No significant difference was observed between the two models. By Cox multiple variable regression analysis, age, male sex, the cutaneous subset of the disease, elevated C reactive protein, class II–IV dyspnoea, ILD, low carbon dioxide diffusing capacity, forced vital capacity, proteinuria, scleroderma renal crisis, depressed left ventricular ejection fraction, digital ulcers and joint involvement were independent predictors of 3-year mortality (table 3), allowing the development of the SCOpE score, ranging between 0 and 32. With an average corrected C-index of 0.80, this score was discriminate. At 3 years, the average AUC was 0.82 (95% CI 0.80 to 0.84; figure 3A). The AUC for 3-year mortality was 0.79 (95% CI 0.75 to 0.81) for diffuse and 0.82 (95% CI 0.80 to 0.85) for limited SSc (online supplementary figure 3c). This score was discriminative for both incident (<1 year) and prevalent SSc (online supplementary figure 3D). The discrimination power of the SCOpE score for 3-year mortality was higher (AUC of 0.82 (95% CI 0.80 to 0.84)) than that of the Bryan score (AUC 0.72 (95% CI 0.70 to 0.74); p<0.001; online supplementary figure 3E).7 8 When divided into quartile, 599 patients with scores ≥15 had a 0.53 (95% CI 0.48 to 0.58) 3-year survival rate, compared with 2777 patients with scores <5, whose 3-year survival rate was 0.98 (95% CI 0.97 to 0.99) (p<0.001; figure 3B).
Supplementary file 4

{kind=link}
![[SP3.jpg]](https://ard.bmj.com/content/annrheumdis/76/11/1897/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
![[SP4.jpg]](https://ard.bmj.com/content/annrheumdis/76/11/1897/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
(A) ROC curves at 3 years for the SCOpE score. The lines indicate ROC curves of 50 models from 50 imputed data sets. (B) Overall survival according to simplified score categories. Curves are plotted for each of the 50 imputed data set. Three-year survival according to SCOpE score: 0.98 (0.97–0.99) (score: 0–4); 0.93 (0.92–0.94) (score: 5–9); 0.80 (0.78–0.83) (score: 10–14); 0.53 (0.48–0.58) (score ≥15). AUC, area under the curve; ROC, receiver operating characteristics; SCOpE, SCleroderma mOrtality p Eustar.
Predictors of low survival in the multiple variable model
Discussion
The strengths of our report include our two-step study with first the collection of all death certificates in France during a 10-year period, corresponding to the analysis of 2719 death certificates from patients with SSc, followed by the interrogation of the very large EUSTAR database that included 11 193 patients and 1072 deaths at the time of the analysis. This large collection of patients represents the most robust report of any mortality study and prediction score. Our analysis of two distinct sources of information and the consistency of our results are evidence that our methodology mitigated the effects of common biases observed in previous studies.
We confirmed that primary heart disease is the main offender in SSc explaining 30% of SSc deaths,1 4 6 14 25 26 while atherosclerosis was responsible for only 5%–8% of deaths.26 This highlights the importance of thorough cardiac investigations to identify patients presenting with SSc at a preclinical stage of PAH and cardiac involvement. Except for systemic hypertension, neither the EUSTAR sample nor the death certificates included a list of cardiovascular risk factors, preventing a correction of the causes of deaths for rates of risk factors. However, in a previous EUSTAR study, the typical cardiovascular risk factors were not identified as important contributors to heart involvement.27
We confirmed that lung involvement is a major complication of SSc, particularly in young patients and in men who, compared with the general population, suffered respectively tenfold and fourfold higher rates of deaths from respiratory diseases. Accordingly, respiratory failure was recently shown to contribute prominently to intensive care unit admissions for management of SSc.28 Besides the high mortality associated with respiratory failure, our study revealed a high mortality from lung infections and a fivefold higher rate of infectious deaths among patients with SSc compared with the general population. These observations highlight the importance of the infectious risk associated with this disease and of the need to use specific therapeutic measures that are underused, such as vaccinations.29
We also observed a high proportion of death from cancer, of the lung in particular, although compared with the general population, the risk of death from cancer was not increased, in contrast to other autoimmune diseases.30 Alternatively, premature death due to terminal SSc may have obscured the age-related increase in deaths from cancer. Finally, the death certificates might have failed to mention the diagnosis of SSc when patients died from cancer.
We observed a gradual decrease in standardised mortality rate over time due to a decrease in mortality unrelated to SSc, while the rate of deaths due to SSc increased. One possible explanation for this finding is that increased survival among the general population may largely account for the increased survival observed in SSc in this study.1 These observations should encourage the community to urgently revise and improve the care of SSc, by focusing on a more accurate identification of poor-prognosis patients, who might benefit from aggressive therapy, and from the development of a critically needed reliable prognostic score.
For this purpose, we developed a weighted risk equation for survival at 3 years from a sample of over 11 000 patients, based on a rigorous data collection by study centres highly skilled in SSc management. There was only a median of 2.0% of missing prognostic variables and we used imputations to minimise the possible role of missing values, and stratified the data analysis by study centre. The respective weight of the selected variables was similar before and after imputation (online supplementary table 7), confirming the robustness of our sample and of our data collection. The AUC of the SCOpE to predict the 3-year mortality was 0.82, and the reliability of our score was confirmed by bootstrapping analysis. This SCOpE ranged from 0 to 32, and is simple to calculate (online supplementary appendix 3). When compared with the Bryan score, our SCOpE score was more discriminate (p<0.001). This score confirmed its robustness in incident and prevalent SSc, as well as in limited and diffuse cutaneous subtypes, suggesting that it is applicable to all patients presenting with this disease. Using that score, we were able to stratify patients among four sharply distinct groups of severity. This risk stratification might help adapt the monitoring to the specific risk represented by a patient, contribute to decision for expert centre referral and advance the diagnosis of internal organ involvement in patients whose score is ≥15. Furthermore, the SCOpE score might help select the candidates for high-level therapeutic interventions, such as stem cell transplantation, and for inclusion in clinical trials and preventive strategies. These broad applications should be validated in dedicated studies. However, our study should be interpreted within its limitations: (1) the precise cause of death may be difficult to ascertain, for example in patients who died away from diagnostic facilities. This may explain disparities between death certificates and adjudicated expert judgement.31 For example, in death certificates, pulmonary embolism was believed to be responsible for 1/3 of cardiac-related deaths. We can hypothesise that most of these deaths might be secondary to right heart involvement or PAH, which were under-recognised by non-experts in SSc. The absence of detailed clinical records and information regarding concomitant illnesses may also bias the death certificates, although the inclusion of a large number of certificates in the analysis should mitigate such biases. Furthermore, our observation of similar causes of death in the certificates analysis and in the EUSTAR sample supports our methodology. (2) The mean disease duration in EUSTAR cohort was over 8 years, which might cause missing of early deaths. However, thanks to the very large population included, we assume this cohort is a representation of our current practice. In addition, early SSc (<3 years) was not associated with mortality. (3) We were not able to externally validate the final model, but we have used the bootstrapping method as a validation tool. Bootstrapping is a robust method that is thought to be used when no external cohort of patients is available.32 (4) Three thousand patients did not have at least one follow-up visit. The disease characteristics were not significantly different in multivariate analysis between patients with and without follow-up, which suggests that it may not have influenced our results. (5) We decided to not include the treatments in our prediction model because (1) in the absence of strict recommendations, many of the disparities observed are based on clinical considerations instead of various forms of the disease, and (2) we wished to develop a score applicable to new patients as well as patients already treated. (6) Finally, since both our study samples included Caucasians, our score cannot be extrapolated to other ethnic groups.
To conclude, our study should impress the community by the lack of progress it reveals in the survival of patients with SSc. An early and systematic management of the large proportion of cardiac complications associated with this disease is in order, in hope of extending survival in SSc. Because of the large difference in mortality compared with the general population, lung involvement as well as infections should be prominently visible on the research agenda. We also developed a robust mortality score to estimate the 3-year survival and risk-stratify patients. With the emergence of new therapies in SSc, these results should help caregivers adapt the monitoring and therapeutic strategies to the specific risk of each patient, with a view to prolong the survival in SSc.
Supplementary file 2
![[SP2.jpg]](https://ard.bmj.com/content/annrheumdis/76/11/1897/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
References
Footnotes
Handling editor Tore K Kvien
Contributors ME, CM and YA formulated the study hypotheses and contributed to its design and analysis of the data, literature search, composition of the tables and figures, and redaction of the first draft and subsequent iterations of the manuscript. ME, MB and CM performed the statistical analyses. JA, EH, ABG, GR, PA, BJ, SV, FC, SU, LC, MT, UML, PC, OD, FI, LPA, RH, RB, AG, ND, MJS, VR, CM, GS, UAW, NH, DM, VS, CDSM, CMM, DO, FI, PGV, BS, ER, SH, JHWD, TZ, MS, AV, EDL, SN, MC, LM, JH, CC, CAVM, KS, SR, LS, BA, VOS, MDS, SY, WASG, EC, JS, JVL, EL, PGDPL, KE, VC, JJAS, OKB, MMC and YA conceived and launched the EUSTAR database, collected data in their respective countries and offered critical comments regarding the manuscript. GR retrieved the death certificates of patients and of the general population and offered critical comments regarding the manuscript.
Funding This study was funded by the “Institut national de la santé et de la recherche médicale (INSERM)” (French National Health and Medical Research Institute).
Competing interests OD reports personal fees from 4D Science, grants and personal fees from Actelion, personal fees from Active Biotech, grants and personal fees from Bayer, personal fees from Biogen Idec, personal fees from BMS, grants and personal fees from Boehringer Ingelheim, personal fees from ChemomAb, personal fees from EpiPharm, personal fees from EspeRare Foundation, personal fees from Genentech/Roche, personal fees from GSK, personal fees from Inventiva, personal fees from Lilly, personal fees from Medac, personal fees from Mepha, personal fees from MedImmune, personal fees from Pharmacyclics, grants and personal fees from Pfizer, grants and personal fees from Sanofi, personal fees from Serodapharm, personal fees from Sinoxa, personal fees from AbbVie, personal fees from iQone Healthcare, outside the submitted work. In addition, OD has a patent mir-29 for the treatment of systemic sclerosis licensed. FI reports personal fees from AbbVie, personal fees from BMS, personal fees from MSD, personal fees from Novartis, outside the submitted work. JHWD reports personal fees from Actelion, grants and personal fees from Anamar, grants and personal fees from Bayer Pharma, grants and personal fees from Boehringer Ingelheim, grants from Celgene, personal fees from Galapagos, grants from GSK, grants and personal fees from Inventiva, personal fees from Pfizer, grants and personal fees from UCB, grants from Novartis, other from 4D Science, outside the submitted work. JvL reports personal fees from Pfizer, grants and personal fees from MSD, personal fees from Eli Lilly, personal fees from BMS, personal fees from Roche, outside the submitted work. Other coauthors have nothing to disclose.
Patient consent Obtained.
Ethics approval Local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data may be available from EUSTAR upon separate scientific request.