Article Text

Abstract
Objective To assess the validity of ultrasound of major salivary glands (sUS) compared with parotid and labial gland biopsies, sialometry, anti-SSA/Ro antibody status and classification criteria in patients clinically suspected with primary Sjögren’s syndrome (pSS).
Methods 103 consecutive outpatients with clinically suspected pSS underwent sUS. Parenchymal echogenicity, homogeneity, hypoechogenic areas, hyperechogenic reflections and clearness of salivary gland border were scored according to the Hocevar scoring system. Total ultrasound score was calculated as the sum of these domains (range 0–48).
Results Absolute agreement between sUS and parotid (83%) and labial (79%) gland biopsy outcome was good. Negative sUS predicts negative parotid gland biopsy, and positive sUS predicts positive labial gland biopsy. Compared with the American European Consensus Group (AECG) classification, sUS showed an absolute agreement of 82%, sensitivity of 71% and specificity of 92%. Compared with the American College of Rheumatology (ACR) classification, absolute agreement was 86%, sensitivity was 77% and specificity was 92%. Compared with the ACR-European League Against Rheumatism (EULAR) classification, absolute agreement was 80%, sensitivity was 67% and specificity was 94%. Positive sUS predicts classification, but negative sUS does not exclude classification. The combination of positive sUS with presence of anti-SSA/Ro antibodies or negative sUS with absence of anti-SSA/Ro antibodies showed a high predictive value for classification as pSS or non-pSS.
Conclusion In our prospective inception cohort study derived from daily clinical practice, absolute agreement between sUS and salivary gland biopsies was slightly higher for parotid compared with labial gland biopsies. The combination of positive sUS and presence of anti-SSA/Ro antibodies highly predicts classification according to the AECG, ACR and ACR-EULAR classification criteria.
- sjögren’s syndrome
- ultrasound
- salivary gland biopsy
- classification criteria
Statistics from Altmetric.com
Introduction
Primary Sjögren’s syndrome (pSS) is a chronic, systemic autoimmune disease characterised by inflammation of the exocrine glands, with an estimated prevalence of 0.05% in the general population.1 Most patients with pSS suffer from xerostomia, keratoconjunctivitis sicca and extreme fatigue.2 In addition, different extraglandular manifestations, most frequently arthralgia, arthritis and myalgia, may be present.2
Currently, multiple criteria sets are available for the classification of pSS. In 2002, the American European Consensus Group (AECG) criteria were developed, and although not endorsed by the American College of Rheumatology (ACR) or European League Against Rheumatism (EULAR) these are yet most commonly used in daily clinical practice.3 4 In 2012, the ACR criteria were developed and provisionally approved by the ACR,5 but these criteria were not well received by many Sjögren’s syndrome (SS) experts.6 In order to develop international consensus on classification criteria, the ACR-EULAR criteria were recently introduced, endorsed by both EULAR and ACR.4 7 In all three sets, salivary gland biopsies and presence of anti-SSA/Ro antibodies play a significant role in classifying patients as pSS.3–5 In the AECG and ACR-EULAR criteria, salivary gland involvement is also assessed by unstimulated whole saliva flow (UWS).3 4
Ultrasound of major salivary glands (sUS) is an upcoming diagnostic method to assess involvement of major salivary glands in pSS.8 9 sUS is well tolerated, non-invasive, inexpensive, non-irradiating and widely available in the rheumatological outpatient clinics, but its reliability depends greatly on its operator. A recent meta-analysis assessing the diagnostic properties of sUS in pSS reported a pooled sensitivity of 69% and specificity of 92%. This meta-analysis also revealed a large clinical and methodological heterogeneity between studies, which hampered interpretation of pooled outcomes and influenced the results reported in the various studies.8 Thus, the possible role of sUS in the diagnosis of pSS remains unclear.8–10
This study assesses the validity of sUS compared with parotid and labial gland biopsies, sialometry, anti-SSA/Ro antibody status and classification criteria in patients clinically suspected with pSS.
Materials and methods
Patients
The present cross-sectional study is based on prospective data from the multidisciplinary Sjögren’s expertise centre in the University Medical Center Groningen, a tertiary referral centre. One hundred and ten consecutive patients clinically suspected with pSS, who underwent sUS as part of the diagnostic work-up and were over 18 years of age, were included. All patients underwent the diagnostic work-up. All domains of the AECG, ACR and ACR-EULAR criteria were assessed, including parotid and/or labial gland biopsy.
Primary assessment
Ultrasonography
All patients were examined with the same ultrasonographic scanner (Esaote MyLab Seven, Genova, Italy), equipped with a high-resolution linear scanner (4-13 MHz). Patients were examined in supine position with their neck slightly extended and turned away from the examined side.11 12 The Hocevar et al12 scoring system was used investigating (1) parenchymal echogenicity compared with the thyroid gland, graded 0–1; (2) homogeneity, graded 0–3; (3) presence of hypoechogenic areas, graded 0–3; (4) hyperechogenic reflections, graded 0–3 in parotid glands and 0–1 in submandibular glands; and (5) clearness of the salivary gland border, graded 0–3, in both parotid and submandibular salivary glands. Total ultrasound score was the sum of these five domains and can range from 0 to 48.12
Other assessments
Parotid and/or labial gland biopsies were considered positive if the focus score (defined as the number of mononuclear infiltrates containing ≥50 lymphocytes/4 mm2 of glandular tissue) was ≥1.13–15 UWS was evaluated by measuring the saliva production in 15 min.3 UWS ≤1.5 mL/15 min was considered abnormal.16 Serum levels of anti-SSA/Ro and anti-SSB/La antibodies were assessed with ELISA tests.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics V.23. Descriptive parameters were expressed as number of patients (%) or mean (SD).
Receiver operating characteristic analysis was performed to determine the accuracy of sUS to predict parotid or labial gland biopsies, UWS, anti-SSA/Ro antibody status and classification as pSS. Area under the curve (AUC) was interpreted as no discrimination (0–0.5), poor accuracy (0.5–0.7), fair (0.7–0.8), good (0.8–0.9) or excellent (0.9–1.0).17 The optimal cut-off point for sUS positivity was determined according to the highest combination of sensitivity and specificity.
The percentage of absolute agreement between sUS outcome and parotid or labial gland biopsies, UWS, anti-SSA/Ro antibody status and classification according to the classification criteria was determined. The association between ultrasound and UWS was analysed using Spearman correlation coefficient (ρ), and interpreted as poor agreement (0.0–0.2), fair (0.2–0.4), moderate (0.4–0.6), good (0.6–0.8) or excellent (0.8–1.0).18 Furthermore, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated.
Mann-Whitney U tests were used to evaluate differences in total ultrasound score between patients with (1) positive versus negative parotid or labial gland biopsies, (2) UWS ≤1.5 mL/15 min versus UWS >1.5 mL/15 min, (3) presence versus absence of anti-SSA/Ro and/or anti-SSB/La antibodies and (4) pSS versus non-pSS according to the classification criteria. p Values <0.05 were considered statistically significant.
Results
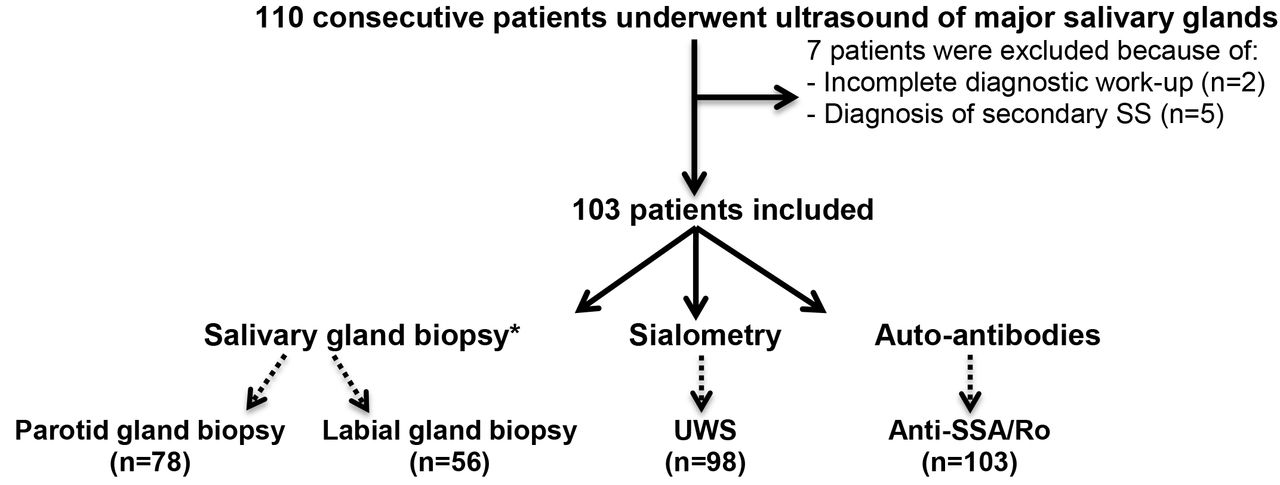
A flow chart of inclusion and exclusion of patients and information about the number of patients included in the analyses on salivary gland biopsies, sialometry and anti-SSA/Ro antibody status is presented in figure 1. Of the 103 included patients, the mean age was 50 years (15), 90% were female and the mean total ultrasound score was 15 (10) (see online supplementary table S1). For research purposes, 43 patients underwent parotid and labial gland biopsies. Of the remaining patients, 35 had a parotid gland biopsy only and 13 had a labial gland biopsy only.
Supplementary file 1

Flow chart of number of patients with available data per analysis. *43 patients underwent parotid gland as well as labial gland biopsy. SS, Sjögren’s syndrome; UWS, unstimulated whole saliva.
Ultrasound versus salivary gland biopsy
The accuracy of sUS to predict a parotid gland biopsy outcome was good, with an AUC of 0.849 (95% CI 0.746 to 0.952) and optimal cut-off point of 15 (see online supplementary table S2). The absolute agreement between sUS outcome and parotid gland biopsy was 83% (65/78), with a sensitivity of 75% (21/28), specificity of 88% (44/50), PPV of 78% (21/27) and NPV of 86% (44/51) (table 1).
Ultrasound of major salivary glands versus salivary gland biopsy, sialometry and anti-SSA/Ro antibodies status
The accuracy of sUS to predict a labial gland biopsy outcome was good, with an AUC of 0.824 (95% CI 0.714 to 0.934) and optimal cut-off point of 14 (see online supplementary table S2). The absolute agreement between sUS outcome and labial gland biopsy was 79% (44/56), with a sensitivity of 72% (21/29), specificity of 85% (23/27), PPV of 84% (21/25) and NPV of 74% (23/31) (table 1).
Total ultrasound score was significantly higher in patients with positive parotid or labial gland biopsies compared with patients with negative parotid or labial gland biopsies (p<0.001; figure 2).

Ultrasound total score compared with salivary gland biopsy. (A) Positive versus negative parotid gland biopsy. (B) Positive versus negative labial gland biopsy. Histopathology: positive parotid or labial gland biopsy was defined as focus score ≥1.
Ultrasound versus sialometry
The accuracy of sUS to predict UWS outcome was poor, with AUC of 0.696 (95% CI 0.593 to 0.799). The absolute agreement between sUS outcome and UWS was 66% (65/98) (table 1).
Total ultrasound score was significantly higher in patients with UWS ≤1.5 mL/15 min compared with patients with UWS >1.5 mL/15 min (p<0.001; see online supplementary figure S1A). There was a fair reversed association between total ultrasound score and UWS total flow (ρ=−0.366) (see online supplementary figure S2B).
Ultrasound versus autoantibodies
The accuracy of sUS to predict anti-SSA/Ro antibody status was good, with an AUC of 0.803 (95% CI 0.711 to 0.894). The absolute agreement between sUS outcome and anti-SSA/Ro antibody status was 82% (84/103) (table 1).
Total ultrasound score was significantly higher in patients with anti-SSA antibodies compared with patients without anti-SSA/Ro antibodies (p<0.001; see online supplementary figure 2).
Ultrasound versus classification criteria
For the following analyses, sUS is compared with classification criteria with the outcome of parotid gland biopsy considered as an item of these criteria. For the comparison of sUS with classification criteria with the outcome of labial gland biopsy considered as an item, see table 2, see online supplementary table S3 and figure 3.
Ultrasound of major salivary glands versus classification criteria
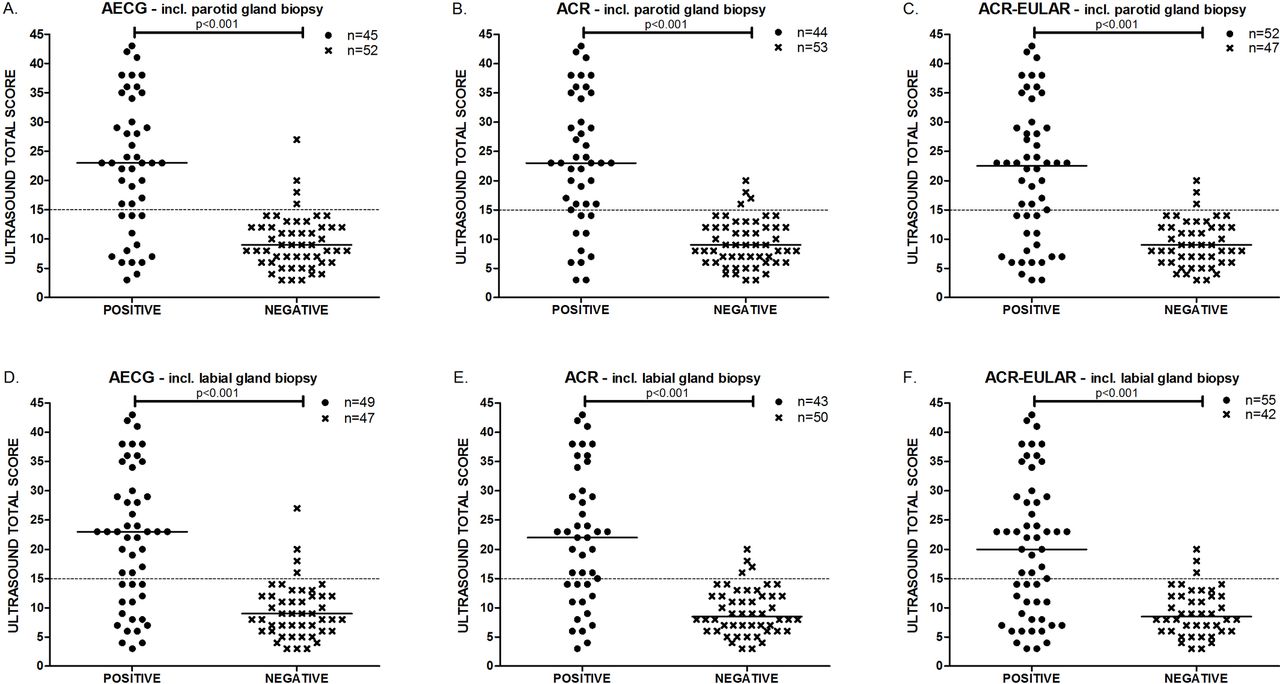
Ultrasound total score compared with classification criteria for pSS. In A–C, when ‘including parotid gland biopsy’ is added, parotid gland biopsy outcome is considered an item of the AECG, ACR and ACR-EULAR criteria. In D–F, when ‘including labial gland biopsy’ is added, labial gland biopsy outcome is considered an item of the AECG, ACR and ACR-EULAR criteria. (A) Positive versus negative of fulfilling AECG criteria, (B) positive versus negative of fulfilling ACR criteria, (C) positive versus negative of fulfilling ACR-EULAR criteria, (D) positive versus negative of fulfilling AECG criteria, (E) positive versus negative of fulfilling ACR criteria and (F) positive versus negative of fulfilling ACR-EULAR criteria. In most patients who underwent only one salivary gland biopsy, classification as pSS or non-pSS could be determined, as the biopsy would not have been decisive for classification. Therefore, ≥90% (93/103) of the patients could be included in the analysis of the agreement between sUS and the different criteria sets including parotid or labial gland biopsy. ACR, American College of Rheumatology; AECG, American European Consensus Group; EULAR, European League Against Rheumatism; pSS, primary Sjögren’s syndrome; sUS, ultrasound of major salivary glands.
The accuracy of sUS to predict AECG classification was good, with an AUC of 0.826 (95% CI 0.735 to 0.918) and optimal cut-off point of 15 (see online supplementary table S3). The absolute agreement between sUS outcome and AECG classification was 82% (80/97), with a sensitivity of 71% (32/45), specificity of 92% (48/52), PPV of 89% (32/36) and NPV of 79% (48/61) (table 2).
The accuracy of sUS to predict ACR classification was good, with an AUC of 0.862 (95% CI 0.777 to 0.947) and optimal cut-off point of 15 (see online supplementary table S3). The absolute agreement between sUS outcome and ACR classification was 86% (83/97), with a sensitivity of 77% (34/44), specificity of 92% (49/53), PPV of 89% (34/38) and NPV of 83% (49/59) (table 2).
The accuracy of sUS to predict ACR-EULAR classification was good, with an AUC of 0.802 (95% CI 0.710 to 0.894) and optimal cut-off point of 15 (see online supplementary table S3). The absolute agreement between sUS outcome and ACR-EULAR classification was 80% (79/99), with a sensitivity of 67% (35/52), specificity of 94% (44/47), PPV of 92% (35/38) and NPV of 72% (44/61) (table 2).
Total ultrasound score was significantly higher in pSS versus non-pSS according to the classification criteria (p<0.001; figure 3).
Predictive value of the combination of sUS and antibody status
In patients with positive sUS combined with anti-SSA/Ro antibodies, 78% (14/18) had a positive parotid gland biopsy and 94% (17/18) had a positive labial gland biopsy.
In patients with negative sUS combined with absence of anti-SSA/Ro antibodies, 93% (37/40) had a negative parotid gland biopsy and 77% (17/22) had a negative labial gland biopsy.
In patients with positive sUS combined with anti-SSA/Ro antibodies, 94% (32/34) fulfilled the AECG, 97% (34/35) fulfilled the ACR and 97% (35/36) fulfilled the ACR-EULAR criteria, considering the outcome of parotid gland biopsies as an item for classification. Percentages are equal when the outcome of labial gland biopsy is considered as an item for classification (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of patients either or not fulfilling the AECG, ACR or ACR-EULAR criteria including only parotid gland biopsy or only labial gland biopsy. When ‘parotid gland’ is mentioned, parotid gland biopsy outcome is considered an item of the AECG, ACR and ACR-EULAR criteria. When ‘labial gland’ is mentioned, labial gland biopsy outcome is considered an item of the AECG, ACR and ACR-EULAR criteria. (A) Fulfilling the AECG, ACR or ACR-EULAR classification criteria, with on the left positive sUS in combination with presence of anti-SSA/Ro antibodies and on the right negative sUS in combination with absence of anti-SSA/Ro antibodies. (B) NOT fulfilling the AECG, ACR or ACR-EULAR classification criteria, with on the left positive sUS in combination with presence of anti-SSA/Ro antibodies and on the right negative sUS in combination with absence of anti-SSA/Ro antibodies. ACR, American College of Rheumatology; AECG, American European Consensus Group; EULAR, European League Against Rheumatism; sUS, ultrasound of major salivary gland.
In patients with negative sUS combined with absence of anti-SSA/Ro antibodies, 98% (45/46) did not fulfil the AECG, 100% (45/45) did not fulfil the ACR and 98% (44/45) did not fulfil the ACR-EULAR criteria, considering the outcome of parotid gland biopsies as an item for classification (figure 4). Percentages are lower when the outcome of labial gland biopsy is considered as an item for classification: 89% (40/45) did not fulfil the AECG, 93% (43/46) did not fulfil the ACR and 89% (39/44) did not fulfil the ACR-EULAR criteria (figure 4).
Discussion
This study assessed the validity of sUS in a representative population of patients with clinically suspected pSS. It is the first study that directly compared the validity of sUS with parotid gland biopsy outcome, and to the best of our knowledge the first that compared the validity of sUS with the ACR-EULAR criteria.
Since the Hocevar scoring system was the most comprehensive and valid, it was incorporated in our daily clinical practice in order to address all relevant aspects of sUS. Previously, three studies evaluated the optimal cut-off of the Hocevar scoring system.12 These studies used different gold standards, viz AECG criteria,12 labial gland biopsy19 or AECG and ACR criteria.20 The cut-off points ranged from 15 to 19. In the present study, the optimal cut-off point for the Hocevar score was found to be 15 in almost all analyses. Applying a higher cut-off value, for example, 17 as used by Hocevar et al,12 would lead to increased specificity and PPV for parotid and labial gland biopsies, as well as for the AECG, ACR and ACR-EULAR classification criteria, at the expense of sensitivity and NPV (see online supplementary table S2 and S3). Furthermore, when comparing the PPV and NPV reported in different studies, it is important to keep in mind that both strongly depend on the prevalence of the disease in the investigated population, while sensitivity and specificity are less influenced.
To date, no consensus has been reached about the optimal scoring system and cut-off point for the ultrasonographic evaluation of the major salivary glands in patients suspected with pSS. Consensus is certainly needed to further elucidate the role of sUS in the diagnosis of pSS and is prerequired for being officially included in the classification criteria for pSS. Additionally, it will make the comparison between similar studies easier. sUS showed good absolute agreement and specificity using salivary gland biopsies as gold standard. Both were slightly higher when parotid gland instead of labial gland biopsies were used, possibly because the parotid gland is included in the sUS evaluation, whereas the labial gland is not.
Interestingly, the parotid gland biopsies were negative in most patients with a negative sUS, but the labial gland biopsies were positive in 26% of patients with a negative sUS. On the other hand, positive sUS predicts positive labial gland biopsies, while 22% of patients with a positive sUS had a negative parotid gland biopsy. When comparing the results of parotid and labial gland biopsies, it is important to keep in mind not all patients had both biopsies performed and the populations in which the agreement of sUS with parotid and labial gland biopsies were evaluated were not the same. However, this is the first study to compare sUS with parotid as well as labial gland biopsies.
There was a fair reversed association between total ultrasound score and UWS total flow. In other words, patients with more pronounced abnormalities on ultrasound tend to have a reduced UWS production. However, there was also a significant amount of patients with few abnormalities on ultrasound who did have a reduced UWS production. This group may consist of patients with early pSS, where UWS is lowered but no sUS abnormalities are yet seen or another condition is causing the decrease in UWS. A next step would be to assess whether the performance of the different classification criteria will improve, when UWS is replaced by salivary gland ultrasonography.
The specificity of sUS was high when anti-SSA/Ro antibody status was used as gold standard, confirming a previous study.21
Our findings regarding the sensitivity and specificity of sUS outcome compared with the classification criteria for pSS are similar with the results described in a recent meta-analysis.8 Sensitivity of sUS was lowest when compared with the recently published ACR-EULAR criteria, when either parotid or labial gland biopsies were considered as an item for classification. It is currently unknown if sUS is sensitive enough to detect changes in the major salivary glands early in the disease course. In our inception cohort, more patients with low sUS scores fulfil the ACR-EULAR criteria compared with the AECG and ACR criteria. This may either suggest that patients are classified as pSS at an earlier stage of the disease according to the ACR-EULAR criteria or that the ACR-EULAR criteria are too liberal.7 Finally, the PPV of sUS compared with the classification criteria was higher than the NPV. Thus, positive sUS predicts fulfilment of the AECG, ACR and ACR-EULAR criteria, but negative sUS does not exclude classification. When applying classification criteria, we should keep in mind that they are developed for research purposes to define homogeneous study groups, although in clinical practice they are often used for diagnostic purposes.22
In accordance with our findings, Astorri et al23 reported that positive sUS was highly predictive of positive labial gland biopsies. Therefore, one could consider not performing a labial gland biopsy in patients with a positive sUS. This previous study also showed that negative sUS was highly predictive of negative labial gland biopsies in patients with sicca symptoms. However, we were unable to confirm this observation with our data, as we found a moderate NPV of sUS for labial gland biopsies. Therefore, in patients with a negative sUS the result of labial gland biopsies could not fully be predicted. There are some possible explanations for this discrepancy. None of the ‘non-Sjögren sicca patients’ in the study of Astorri et al23 had a positive labial gland biopsy, while some of our ‘non-Sjögren sicca patients’ did have a positive biopsy. These biopsies may be false-positive,24 25 or these patients have SS not meeting the classification criteria. Moreover, Astorri et al23 did not mention the time interval between sUS and labial gland biopsy, which may be longer than in our study and a different sUS scoring system was used.
Astorri et al23 stated that labial gland biopsies should not be performed in extractable nuclear antigen (ENA)-negative patients with negative sUS, unless there are other strong clinical indications for SS. Based on our data, we cannot support this conclusion. It is well established that negative serology occurs in 10%–50% of patients with pSS and correlates with milder disease.26–28 Interestingly, when labial gland biopsies are considered an item of the classification criteria, 7%–11% of our patients with the combination of negative sUS and absence of anti-SSA/Ro antibodies were classified as pSS according to the different criteria sets. In these anti-SSA/Ro-negative patients, positive biopsies are decisive for classification.29 Thus, ultrasound cannot fully replace salivary gland biopsies as there is a risk of underdiagnosing serological negative patients. Consequently, we recommend that physicians should still consider performing biopsies in patients with absence of anti-SSA/Ro antibodies and negative sUS, especially when gland function (eg, abnormal Schirmer or UWS) is impaired or when there are other signs and symptoms pointing to pSS.
Strikingly, almost all of our patients with both a positive sUS and presence of anti-SSA/Ro antibodies fulfilled the classification criteria for pSS. In this patient group, physicians could consider to skip the salivary gland biopsy as the combination of positive sUS and presence of anti-SSA/Ro antibodies is already highly suggestive of pSS. These rather interesting results are to be confirmed in other cohorts.
The main strength of our study is that consecutive patients clinically suspected with pSS were included. Thus, the study population clearly represents the clinical circumstances in daily clinical practice. Moreover, our Sjögren’s expertise centre is one of the few centres in which both parotid and labial gland biopsies can be performed.14 Having access to parotid gland biopsies has several advantages, in particular that repeated biopsies of the same parotid gland can be performed (eg, for monitoring treatment efficacy) and mucosa-associated lymphoid tissue (MALT)-lymphoma might be identified at an earlier stage.14
In conclusion, in our prospective inception cohort study derived from daily clinical practice, absolute agreement between sUS and salivary gland biopsies was good, although slightly higher for parotid compared with labial gland biopsies.
Positive sUS predicts classification according to the AECG, ACR and ACR-EULAR classification criteria, but negative sUS does not exclude classification.
Positive sUS in combination with presence of anti-SSA/Ro antibodies highly predicts classification according to the AECG, ACR and ACR-EULAR criteria. The combination of negative sUS and absence of anti-SSA/Ro antibodies highly excludes classification when parotid gland biopsy outcome is considered as an item for classification, but when the outcome of labial gland biopsy is considered as an criteria item, combining negative sUS with absence of anti-SSA/Ro antibodies does not exclude classification.
Acknowledgments
The authors would like to acknowledge the participating patients.
Part of this study has been presented at the ACR 2016 in Washington and the corresponding abstract has been published as a conference abstract.
References
Footnotes
Handling editor Tore K Kvien
Contributors EM and KD: designed the study, collected, analysed and interpreted data, drafted the article, and approved the version to be published. SA: designed the study, analysed and interpreted data, critically revised the article, and approved the version to be published. JFvN and AJS: critically revised the article and approved the version to be published. FGMK, FKLS, AV and HB: designed the study, critically revised the article and approved the version to be published.
Funding No funding has been received for the conduct and/or preparation of this article.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Ethics committee of the University Medical Center Groningen (METC waiver 016/120).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.