Article Text

Abstract
Background Previous data have shown that etanercept levels are associated with clinical response in rheumatoid arthritis. However, for ankylosing spondylitis (AS), data regarding this topic are inconclusive.
Objectives To investigate the relationship between etanercept levels and clinical response in patients with AS.
Methods Observational prospective cohort study of 162 patients with AS =treated with etanercept, monitored during 24 weeks of treatment. Etanercept trough levels were determined, retrospectively, using an ELISA. Disease activity was measured using AS Disease Activity Score (ASDAS), including C-reactive protein (CRP) and Bath AS Disease Activity index (BASDAI). Active disease was defined as ASDAS≥2.1. Since etanercept is a drug administered at home there might have been some variation in trough level sampling.
Results At 24 weeks etanercept levels were significantly higher in patients with ASDAS<2.1, (3.8 mg/L; IQR 2.5–5.2) compared with patients with ASDAS≥2.1 (2.3 mg/L; IQR 1.2–3.4; p≤0.001). Generalised estimating equation analysis demonstrated a statistically significant association between etanercept levels and ASDAS, BASDAI, CRP and erythrocyte sedimentation rate (all p<0.001). When patients were categorised into quartiles according to etanercept levels, the lowest quartile (etanercept<1.80 mg/L) comprised 35% of all patients with ASDAS≥2.1 while the highest quartile comprised only 14%.
Conclusions Disease activity and inflammation are associated with etanercept levels in patients with AS at 24 weeks of treatment. Measuring etanercept levels might help in identifying overtreatment and undertreatment and optimise etanercept therapy in AS.
- Ankylosing Spondylitis
- Anti-TNF
- Pharmacokinetics
- Treatment
- TNF-alpha
Statistics from Altmetric.com
Introduction
The efficacy and safety of tumour necrosis factor (TNF) inhibitor treatment has been demonstrated for ankylosing spondylitis (AS), although approximately 40% of patients do not respond to TNF inhibitor treatment.1 All TNF inhibitors are prescribed in a fixed dose without taking differences in pharmacokinetics into account. However, a substantial proportion of patients remain in a state of low disease activity after dose reduction.2–5 In addition, dose registration trials of etanercept show that a proportion of patients with rheumatoid arthritis (RA) achieve acceptable response rates with a lower dose than standard.6 A previous study of 108 patients with AS treated with etanercept 50 mg subcutaneously weekly showed that administration of etanercept 50 mg twice weekly in those whose condition did not respond to initial treatment did not result in significantly higher response rates (76% vs 71%) in comparison to 50 mg SC once weekly.7 Possibly, patients with AS whose condition did not respond to treatment with low drug levels could profit from a dose increase but drug levels were not taken into account in this study.
The above findings indicate that a proportion of patients are undertreated or overtreated and that there are opportunities to adapt etanercept dose to individual needs. This potentially saves costs, which is important considering the high financial burden of anti-TNF treatment. Currently, due to a lack of dose-tapering guidelines, adaptations of TNF inhibitor dosing regimes are based solely on the clinical opinion of the rheumatologist. Previous studies have shown an association between etanercept levels and response in patients with RA.8 For AS the available data on this subject are lacking. Since therapeutic options in AS are still limited, it is crucial to identify parameters that help to optimise use of TNF inhibitors. In a study of 53 patients with AS, etanercept levels were similar for the responder and non-responder groups.9 Another study, in which 20 patients with AS were treated with etanercept, demonstrated a significant negative correlation between etanercept level and C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) but not with Bath AS Disease Activity index (BASDAI).10
The aim of this study was to investigate the relationship between clinical response and etanercept levels in a large group of patients with AS to explore the utility of drug-level testing for the optimisation of etanercept treatment in AS.
Patients and methods
Study design and patients
This prospective observational cohort consisted of 162 consecutive adult patients with AS (according to the 1984 modified New York Criteria11) who received etanercept at the Department of Rheumatology, Jan van Breemen Research Institute|Reade, Amsterdam. All patients had disease that failed to respond to at least two non-steroidal anti-inflammatory drugs (NSAIDs) at the maximal tolerable dosage or had contraindications for the use of NSAIDs before start of TNF-inhibition treatment according to the Assessment of Spondyloarthritis International Society consensus statement of initiation and continuation of TNF-inhibition therapy in AS.12 Patients were treated with etanercept and concomitant NSAID and/or disease-modifying antirheumatic drug (DMARD) therapy, or with etanercept monotherapy. All patients started with etanercept 50 mg subcutaneously every week. If mandatory, as judged by the rheumatologist, the dosing frequency of etanercept could be adapted to 50 mg twice weekly or every 2 weeks. The study was approved by the Medical Ethics Committee of the Slotervaart Hospital and Jan van Breemen Research Institute|Reade. All patients gave written informed consent.
Clinical response
Disease activity was assessed at baseline and after 4, 12 and 24 weeks of therapy and measured with the AS Disease Activity Score, including CRP (ASDAS)13 and BASDAI.14 Active disease was defined as ASDAS≥2.1.15 ,16
Measurements of etanercept concentrations
Trough serum samples were taken at each visit and etanercept concentrations were measured, retrospectively, by ELISA, designed by Sanquin Research Amsterdam, based on the principle that etanercept is captured via its ability to bind TNF. The details on this assay are given in online supplementary text.
Statistical analysis
For statistical analysis, SPSS V.17.0 was used. For differences between groups, an independent sample t test, Mann–Whitney U test or χ2 test was used, as appropriate. The threshold for significance was set at p<0.05. The generalised estimating equation (GEE) approach (using an exchangeable correlation matrix) was used to investigate the association between etanercept levels and disease activity or inflammation over time. The influence of confounders on this association was investigated. Variables considered as potential confounders were chosen from all available baseline variables if unrelated to ASDAS (hence, not in analysis: BASDAI, CRP and ESR) or BASDAI (hence, not in analysis: ASDAS and visual analogue score general) or CRP (not in analysis: ASDAS and ESR) or ESR (not in analysis: ASDAS and CRP). Variables were included in the regression model as confounders if the β changed 10% or more after inclusion of the variable. To analyse clinical response in patients at 24 weeks of treatment we used last observation carried forward for patients who discontinued etanercept treatment prematurely.
Results
Patient characteristics
The baseline characteristics of 162 patients are shown in table 1. For 11 (6.8%) patients the assessment of response status was not possible due to missing ASDAS data at 24 weeks of treatment. To exclude missing data bias a sensitivity analysis was performed for patients who completed 6 months of etanercept treatment; this did not alter the results (data not shown). Eighty-four patients (52%) had an ASDAS<2.1 and 67 (41%) patients had an ASDAS≥2.1 at 24 weeks of follow-up. At baseline, patients with ASDA≥2.1 had a higher body mass index (BMI) (p=0.001), BASDAI (p=0.03) and Bath AS Functional Index (BASFI) (p<0.001) and a lower number of patients were human leukocyte antigen B27 (HLA-B27) positive (p=0.02).
Baseline demographics and clinical characteristics for the total population and for ASDAS inactive to moderate disease activity (<2.1) and high disease activity (≥2.1) at 24 weeks of follow-up (last observation carried forward)*
Discontinuation of treatment
In total, 14 (8.6%) patients dropped out of the study before 24 weeks of treatment: 12 patients stopped due to treatment failure and 2 due to adverse events (injection site reaction, recurrent infections). Of the 14 patients who dropped out, 13 patients had an ASDAS≥2.1 at the time of drop out.
Clinical response and etanercept concentrations
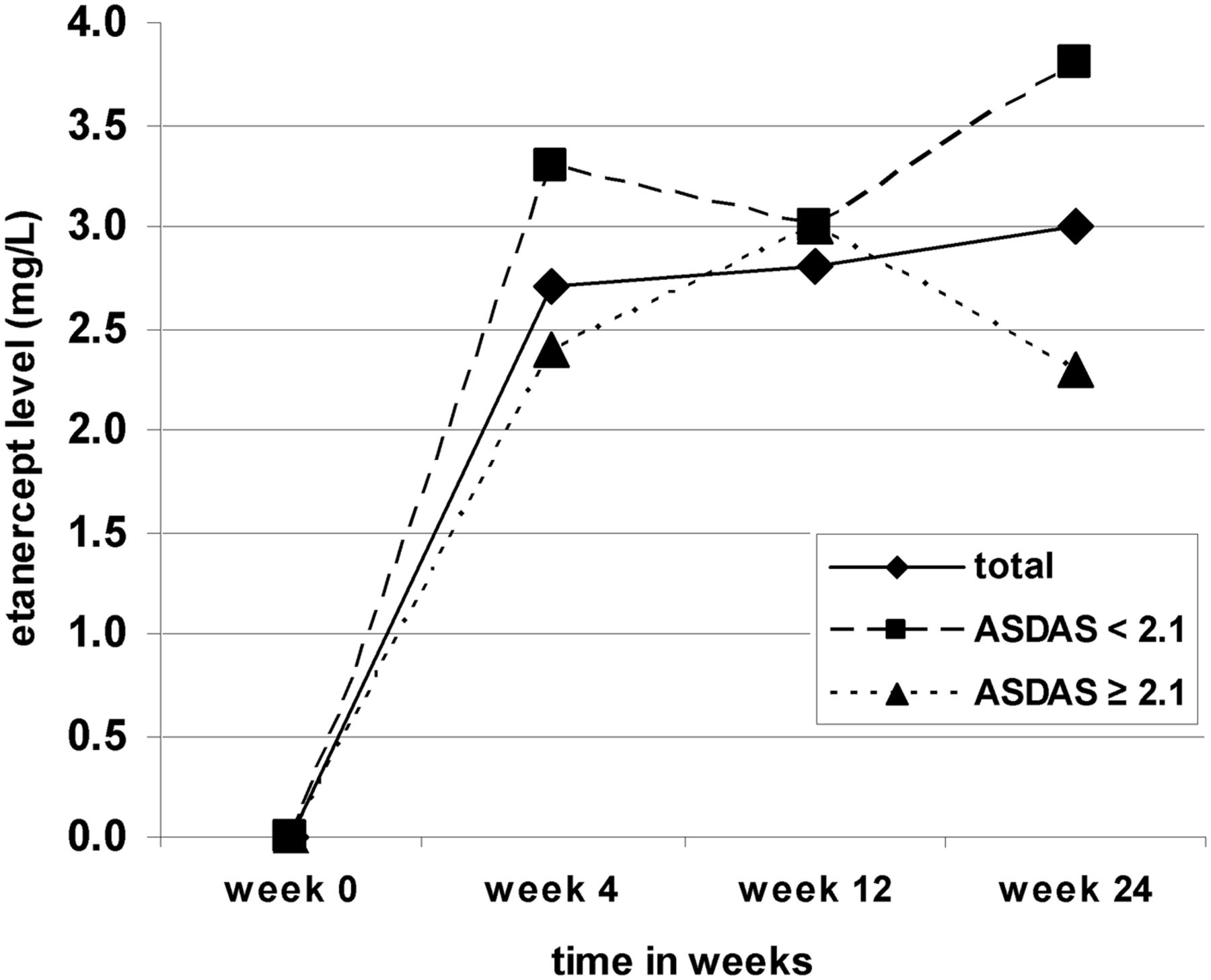
After 24 weeks 148 (91.4%) patients were still on etanercept treatment. In one patient etanercept dosing frequency was decreased to once every 2 weeks and none had a dose increase. At week 24 median etanercept level was 3.0 mg/L (IQR 1.8–5.0) and varied from undetectable to 9.7 mg/L. Etanercept levels at 24 weeks of treatment were significantly higher in patients with ASDAS<2.1 (3.8 mg/L; IQR 2.5–5.2) compared with patients with ASDAS≥2.1 (2.3 mg/L; IQR 1.2–3.4) (p<0.001) (figure 1).

Etanercept levels (mg/L) over time for patients with ankylosing spondylitis with inactive to moderate disease (ASDAS<2.1) and patients with high disease activity (ASDAS≥2.1). ASDAS, Ankylosing Spondylitis Disease Activity Score.
GEE analysis demonstrated a significant association between etanercept concentration and disease activity. ASDAS: regression coefficient (RC) −1.02, 95% CI −1.17 to −0.87, p=0.001, no confounding variables were found; BASDAI: RC −0.14, 95% CI −0.2 to 0.05, p=0.001, after correction for ESR; CRP: RC −0.01, 95% CI −0.02 to −0.004, p=0.001, after correction for BASDAI; ESR: RC −0.01, 95% CI −0.02 to −0.006, p=0.001, after correction for BASFI and age.
In addition, we stratified all patients into quartiles according to the etanercept level at 24 weeks of treatment (figure 2). The lowest quartile (etanercept level<1.8 mg/L) comprised 35% of all patients with ASDAS≥2.1 while the highest quartile comprised only 14%. The highest quartile (etanercept level≥4.6 mg/L) comprised 36% of all patients with ASDAS<2.1, which was statistically significantly more compared with the lowest quartile (p=0.001), which comprised only 15%. Patients of the highest quartile had a statistically significant lower BASDAI (5.4 (4–6.6)) and BMI (24.5 (22.4–26.1)) at baseline compared with patients of the lowest quartile BASDAI (6.4 (5.6–7.6)) and BMI (26.2 (23.6–30)) (respectively, p=0.03 and 0.02).

Percentage of patients with ASDAS<2.1 and ≥2.1 stratified according to etanercept levels at 24 weeks of treatment. Each group contains 25% of all patients. ASDAS, Ankylosing Spondylitis Disease Activity Score.
Figure 3 shows a concentration–effect curve of etanercept in patients with AS at 24 weeks of treatment. All 162 patients were stratified according to etanercept level (low to high) with each dot representing the mean etanercept level and correlating mean ΔASDAS per 11 patients; only the last dot represents 12 patients. The cut-off for clinically important improvement based on ASDAS is set at ΔASDAS≥1.1 points. Most dots are above this cut-off value, although a large variability is seen among patients which is represented by the SD. A clear therapeutic window could not be identified at 24 weeks in our cohort of patients with AS (figure 3).

{kind=link}
{kind=link}
{kind=link}
Etanercept concentration–effect curve in patients ankylosing spondylitis with at 24 weeks of treatment. ASDAS, Ankylosing Spondylitis Disease Activity Score. One dot represents the ΔASDAS per 11 patients; the last dot represents 12 patients.
Discussion
Our data of 162 patients with AS showed an association between etanercept level and ASDAS, BASDAI, CRP and ESR with a GEE analysis. Thirty-five per cent of patients with an ASDAS≥2.1 at 24 weeks of treatment had low etanercept levels (<1.80 mg/L), therefore further study is needed to determine whether these patients would benefit from a dose increase. A previous study of 108 patients with AS treated with etanercept 50 mg subcutaneously weekly showed that administration of etanercept 50 mg twice weekly in patients whose condition did not respond to initial treatment did not result in significantly higher response rates (76% vs 71%) compared with 50 mg subcutaneously once weekly, although drug levels were not taken into account.7 Possibly, patients with high disease activity who will benefit from a dose increase can be identified by measuring etanercept level. This strategy can only be cost effective if etanercept dose is also lowered in a selective group of patients with AS with low disease activity. Our data show that 36% of patients with high etanercept levels (>4.6 mg/L) had an ASDAS<2.1. Possibly, the dosing interval of etanercept can be prolonged in these patients without an increase in disease activity. This is currently a hot topic, since the costs of biological treatment increased enormously during the last decade. At the moment, limited data are available on success rates of etanercept interval prolongation and discontinuation in patients with AS with low disease activity.17 Our concentration–effect curve does not show clear cut-offs to identify the therapeutic window of etanercept in our AS cohort. For optimising etanercept treatment in patients with AS it is important to identify and validate the therapeutic window of etanercept, specified for AS, in a larger group of patients because it provides information, additional to clinical parameters, regarding undertreatment and overtreatment.
Data on etanercept level in association with response and disease activity in AS are limited and inconclusive. One study, in which 20 patients with AS were treated with etanercept, showed data comparable to our results. The authors found a significant negative correlation between etanercept level and CRP and ESR. However, unlike our data, their data did not show this correlation with BASDAI.10 Another study of 53 patients with AS could not detect a difference in etanercept levels between the responder and non-responder groups (based on BASDAI50 response criteria).9 Probably, patient numbers in these studies were too small to detect a significant difference for BASDAI and BASDAI50 response.
In this study ASDAS was used to assess disease activity because it also includes parameters of inflammation (ESR or CRP). This is important since suppression of inflammation is the mechanism of action in TNF-inhibition therapy. Our study shows that BMI, BASDAI, BASFI and HLA-B27 at baseline were statistically significantly different between groups. ASDAS has been developed recently and therefore limited data on predictors of response are currently available. Predictors for other response criteria are available but cannot directly be extrapolated.18 ,19 Increased levels of CRP or ESR have previously been described as predictors of ASDAS major improvement (ΔASDAS>2.0),18 however further research on predictors of ASDAS response is needed.
An important cause of non-response to adalimumab or infliximab treatment is subclinical drugs levels due to antidrug antibody (ADAb) formation in patients with AS.10 ,19 ,20 Etanercept is probably not or only marginally immunogenic, since we previously did not detect ADAbs against etanercept with an antigen binding test.8 Other studies have detected ADAbs against etanercept, however these ADAbs had no apparent effect on clinical outcome.21 Anti-etanercept antibodies were not investigated in the current study because the relationship between etanercept drug level and clinical outcome was the primary focus. Although immunogenicity is not an important factor in etanercept treatment, non-response is an issue in etanercept treatment too. Other factors influencing pharmacokinetics of etanercept, like concomitant DMARD use and patient-related factors, might be possible explanations for non-response to etanercept.22 In our study, patients with low etanercept levels at 24 weeks of treatment had a statistically significant higher BMI and BASDAI score at baseline compared with patients with high etanercept levels. BMI has been described as a factor influencing etanercept levels in patients with RA8 and AS,8 24 but data on this topic are inconclusive. Possible explanations might be the inflammatory effect of adipose tissue influencing target load24 or a difference in body distribution influencing the volume of distribution. The influence of concomitant DMARDs on etanercept level and response could not be studied here due to small numbers of patients using sulfasalazine or methotrexate.
There are some limitations to this study. First, missing BASDAI questionnaires or CRP measurement. The sensitivity analysis did not alter the results. Second, since etanercept is a drug administered at home there might have been some variation in trough level sampling.
In conclusion, our data show a clear association between disease activity, inflammatory markers and etanercept levels in patients with AS at 24 weeks of treatment. This indicates that therapeutic drug monitoring can be beneficial in addition to clinical measurements alone in characterising etanercept non-responders (low vs normal to high etanercept levels) and identifying responders in whom etanercept interval can be prolonged. However, further research on the possibilities of etanercept interval prolongation in patients with AS and low disease activity is needed.
Acknowledgments
The authors are grateful to the Clinical Research Bureau of the Jan van Breemen Research Institute|Reade, which received support from the Dutch Arthritis Foundation, for help in the conduct of the study. They thank the research nurses and medical doctors for performing clinical assessments. Finally, the authors wish to thank the technicians of Sanquin Diagnostics Services for performing the assays.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Contributors Study concept and design: ELK, MTN, IEvdH-B, DvdK, TR, GJW and CLMK. Acquisition of data: ELK and CLMK. Analysis and interpretation of the data: ELK, GJW and CLMK. Clinical revision and drafting of the manuscript for important intellectual content: ELK, MTN, IEvdH-B, DvdK, TR, GJW and CLMK. Obtained funding: MTN, GJW and CLMK. Study supervision: MTN, GJW and CLMK. Final approval: ELK, MTN, IEvdH-B, DvdK, TR, GJW and CLMK.
Funding Collection of the data and measurement of etanercept levels was funded by Pfizer (grant numbers WS2084734 and WS1420476).
Competing interests MTN reports having received consultancy fees from Abbott, Roche, Pfizer, MSD, UCB, SOBI and BMS, payment for lectures from Abbott, Roche and Pfizer. GJW reports having received a research grant from Pfizer (Wyeth) (paid to the institution) and payments for lectures from Pfizer and Amgen. CLMK reports having received payment for lectures from AbbVie and Pfizer. TR reports having received payment for lectures from AbbVie and Pfizer.
Patient consent Obtained.
Ethics approval The study was approved by the medical ethics committees of Jan van Breemen Research Institute|Reade and the Slotervaart Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.