Article Text

Abstract
Objectives To evaluate the effect of adding a 10-week treatment of adalimumab to a standardised treatment with corticosteroids on the ability to taper more rapidly corticosteroid doses in patients with newly diagnosed giant cell arteritis (GCA).
Methods Patients included in this double-blind, multicentre controlled trial were randomly assigned to receive a 10-week subcutaneous treatment of adalimumab 40 mg every other week or placebo in addition to a standard prednisone regimen (starting dose 0.7 mg/kg per day). The primary endpoint was the percentage of patients in remission on less than 0.1 mg/kg of prednisone at week 26. Analysis was performed by intention to treat (ITT).
Results Among the 70 patients enrolled (adalimumab, n=34; placebo, n=36), 10 patients did not receive the scheduled treatment, seven in the adalimumab and three in the placebo group. By ITT, the number of patients achieving the primary endpoint was 20 (58.9%) and 18 (50.0%) in the adalimumab and placebo arm, respectively (p=0.46). The decrease in prednisone dose and the proportion of patients who were relapse free did not differ between the two groups. Serious adverse events occurred in five (14.7%) patients on adalimumab and 17 (47.2%) on placebo, including serious infections in three patients on adalimumab and five on placebo. Two patients died in the placebo arm (septic shock and cancer) and one in the adalimumab group (pneumonia).
Conclusions In patients with newly diagnosed GCA, adding a 10-week treatment of adalimumab to prednisone did not increase the number of patients in remission on less than 0.1 mg/kg of corticosteroids at 6 months.
Clinical trial registration number NCT00305539.
- Giant Cell Arteritis
- Anti-TNF
- Corticosteroids
Statistics from Altmetric.com
Giant cell arteritis (GCA) is the most frequent form of vasculitis affecting the elderly. It is characterised by a granulomatous inflammation of the wall of large vessels. Corticosteroids are the key treatment of GCA, with quite high doses ranging from to 0.4 to 1 mg/kg per day.1 In GCA, corticosteroids have a very good efficacy; however, corticosteroids must be given for up to a year and sometimes more to control persistent activity or adrenal insufficiency. As a result, most patients develop glucocorticoid-related complications that cause important morbidity, disability and possible increased mortality.2–4 To date, except for a possible effect of methotrexate, which remains debated,5 no reliable glucocorticoid-sparing drugs have yet been identified.6–9
Immunohistological data demonstrated that tumour necrosis factor (TNF) is detected in giant cells and macrophages of intima and media of inflamed arteries, suggesting that TNF could be involved in the infiltration and arterial wall destruction characteristic of temporal arteritis.10 Some reports have suggested that anti-TNF therapy could be useful in cases of refractory disease or corticosteroid dependence.11–15 However, two randomised controlled trials have shown more contrasting results.16 ,17 Nevertheless, both trials were of a small sample size and evaluated the efficacy of anti-TNF in patients having a disease controlled by prednisone17 or having either corticosteroid-related side effects or cortico-dependence.16 Moreover, one of the trials assessed the efficacy of etanercept,14 which has been recognised not to be effective in controlling granulomatous inflammation in various other granulomatous diseases,18–20 due to its low stability binding on membrane TNF.21
We report the results of a randomised, placebo controlled, double-blind, multicentre trial assessing the effect of an adjunctive initial 10-week treatment with placebo or adalimumab to a standardised treatment with corticosteroids on the ability to taper more rapidly corticosteroid doses in patients with newly diagnosed GCA.
Patients and methods
Design
We designed a multicentre, randomised, double-blind, placebo controlled study to determine whether a short initial treatment with adalimumab added to a standardised programme of corticosteroid therapy in patients with newly diagnosed GCA would help to decrease corticosteroid requirement without increasing the relapse rate: HECTHOR (Humira* pour l'Epargne CorTisonique dans la maladie de HORton).
The study protocol was approved by the institutional review boards or committees for the protection of persons at the individual study sites. The study was conducted according to the current regulations of the International Conference on Harmonisation guidelines, and the principles of the Declaration of Helsinki. All patients provided written informed consent before participating in any protocol-specific procedures. Patients were enrolled from 16 June 2006 to 25 May 2010, and the last patient completed the study on 11 April 2011.
Setting
The study was conducted in 23 departments of rheumatology or internal medicine in France.
Participants
To be eligible for the study, patients had to be older than 50 years, have had a diagnosis of GCA according to the 1990 American College of Rheumatology Hunder criteria.22 If patients had started corticosteroids before randomisation, the dosage might be less than 1 mg/kg per day and it might have been initiated for less than 14 days before random assignment. The presence of typical findings of GCA on temporal biopsy was initially mandatory for inclusion in the trial. However, due to the slow progression of recruitment, the protocol was amended after the inclusion of 25 patients on 28 November 2007, and temporal artery biopsy was performed for all patients but its positivity was not mandatory to be eligible if the patients fulfilled Hunder criteria.
Patients were excluded if they had GCA-related visual symptoms (such as transient or permanent visual loss or diplopia) or had received anti-TNF or other forms of immunosuppressive therapy (such as methotrexate, azathioprine or other cytotoxic agents).
We excluded patients with: serious or chronic infections in the previous 30 days or who had required antibiotics in the previous 14 days; opportunistic infections; cancer or lymphoproliferative disorders within the 5 years before screening (with the exception of treated and cured squamous or basal cell carcinoma of the skin); a history of moderate to severe congestive heart failure or demyelinating disease; a recent stroke; current signs or symptoms of severe, progressive, or uncontrolled disease; evidence of active tuberculosis or latent tuberculosis (as defined by tuberculin skin test >5 mm or positive interferon gamma release assay); active chronic hepatitis B or C or HIV.
Randomisation and intervention
Adalimumab regimen
Patients were randomly assigned in a 1:1 ratio to receive subcutaneous injection of adalimumab 40 mg or placebo at weeks 0, 2, 4, 6, 8, 10 in addition to prednisone (starting dose 0.7 mg/kg per day). The drug and placebo were indistinguishable in appearance. Randomisation was performed by use of a computer-generated list. Allocation to treatment group was performed by using a central randomisation procedure after facsimile verification of the correctness of inclusion criteria. Patients, investigators and study personnel were blinded to treatment assignments during the study. The time between randomisation and the first injection of the study drug was a maximum of 7 days.
Prednisone regimen
Prednisone was tapered progressively according to a standardised protocol (table 1). At each time point, prednisone could be decreased if patients had no clinical symptom and a C-reactive protein (CRP) level less than 15 mg/L. In cases of relapse (see definition below), the prednisone dose was increased to the immediately previous dose for 4 weeks and then further decreased according to the standardised schedule. In cases of active disease despite this protocol or in the case of relapse, the treatment schedule was left to the discretion of the physician in charge of the patient.
Prednisone decrease schedule
Additional treatments
As some data suggested that low-dose aspirin decreases the rate of visual loss and cerebrovascular events in patients with GCA,23 all patients received low-dose aspirin (80–250 mg/day) during the first 3 months of the trial, with proton pump inhibitors if necessary. For preventing bone loss, all patients received a once-weekly administered bisphophonate dose associated with vitamin D (400UI/day) and calcium (1000 mg) supplementation.
Outcomes and measurements
The primary endpoint was the percentage of patients in remission with less than 0.1 mg/kg per day of prednisone at week 26. The secondary objectives were to assess the decrease in prednisone dose during the first 6 months of treatment, the proportion of patients who remained relapse free at 1 year, and the safety of a 10-week treatment with adalimumab in patients with GCA.
Remission was defined as the disappearance of clinical symptom and a CRP less than 15 mg/L. Relapse was defined as the reappearance of GCA-related clinical symptoms or an increase in CRP greater than 15 mg/L, at two time points at 1 week apart without any other obvious aetiology.
Statistical analysis
Sample size
The study was designed with a planned sample size of 100 patients (50 in each group). According to a literature review,3 it was suspected that the percentage of patients achieving remission at 6 months with a prednisone dose below 0.1 mg/kg per day was approximately 40%. Adjunction of adalimumab would be considered as clinically meaningful if this proportion rose to 70% of patients. The power calculations were based on a bilateral χ2 test, with a type I error rate of 5%. To detect such a difference with a power of 80%, 42 patients in each arm was necessary. This number was increased to 50, with regard to the expected loss to follow-up rate. However, the rate of enrolment was slower than expected, and thus the sponsor asked for the termination of inclusions before the completion of the 100 planned patients in the study.
Primary endpoint
The analysis was done according to the intention-to-treat principle. The proportion of patients maintaining remission at week 26 with a prednisone dose below 0.1 mg/kg per day was compared between the two groups using a logistic regression model with random effects at the centre level. If the prednisone dose at week 26 was not available, the patient was considered a non-responder to conform to the intention-to-treat principle. As a sensitivity analysis, a per-protocol analysis with only patients having received the planned treatment was performed.
Secondary endpoints
The primary analysis was repeated for the proportion of patients maintaining remission at week 52.
The decrease in prednisone dose was compared between the two groups over the 26 and 52-week periods. This difference between groups was analysed using a linear model with random effects at the patient and centre levels. Inference was based on the restricted maximum likelihood solution. The model incorporates all available data for each patient into the analysis provided all patients had baseline data. It provides a likelihood function for the observed data from which treatment effects and other parameters can be estimated, with no additional steps being required to allow for missing data (under the hypothesis that missing data were missing at random). This model thus compared the mean adjusted difference at weeks 26 and 52 between the two groups
Time to first relapse was analysed using Kaplan–Meier survival. The time to first relapse was defined as the number of days between the date of first relapse and the date of inclusion. For those who did not relapse, time to first relapse was censored using the date of their final study visit. To assess difference, a linear rank test stratified on the centre was used.
All tests were two tailed; p values less than 0.05 were considered significant. Data analysis involved the use of SAS V.9.3 for Windows and R V.2.15.1.
Results
Patient characteristics
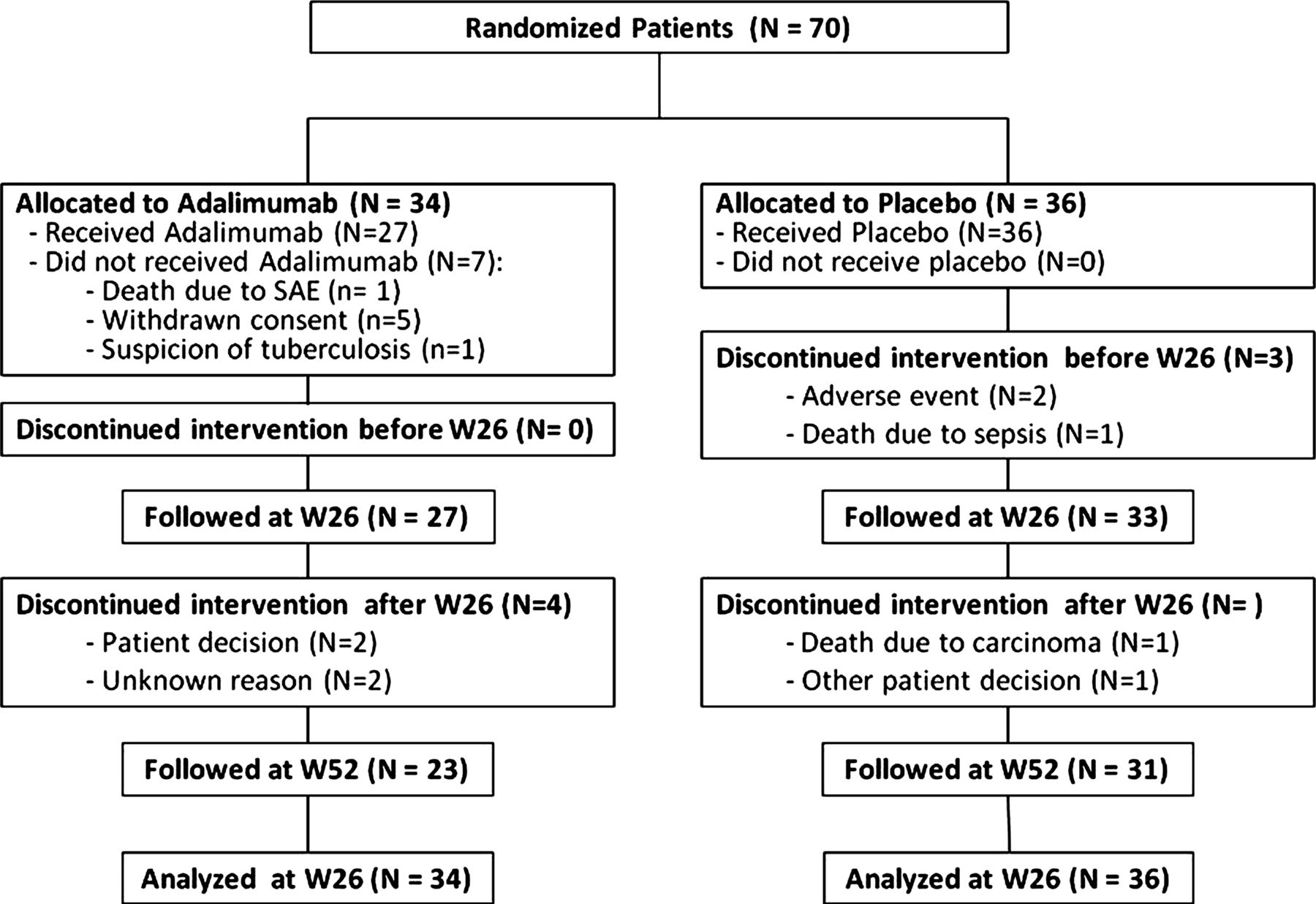
Seventy patients were enrolled, 34 in the adalimumab group and 36 in the placebo group (figure 1). Baseline demographic and disease characteristics of the treatment groups were similar (table 2). Fifty (71.4%) patients had typical findings of GCA on baseline temporal artery biopsy.
Patient characteristics

Flow of participants. SAE, serious adverse event; W, week.
Ten patients did not receive the scheduled treatment until the 26-week assessment, seven in the adalimumab and three in the placebo group. In the adalimumab group, all seven patients did not receive any drug injection: five withdrew consent (one of whom died 2 months later from arterial ischaemia due to GCA), one died from pneumonia 2 months after random assignment, and one was suspected of having tuberculosis on chest CT scan and was thus finally excluded after randomisation without having received any treatment dose. In the placebo group, two patients stopped the treatment because of adverse events (one infectious cellulitis at week 2 and one felt faint at week 6), and one died from septic shock at week 4. The three patients who died before week 26 were considered non-responders for the primary outcome. For the remaining seven patients who did not receive the scheduled treatment, the primary outcome at week 26 was obtained.
Efficacy
All followed patients in both groups improved after the initiation of glucocorticoid therapy with regression of all reversible manifestations. The number of patients in remission at 26 weeks with a prednisone dose less than 0.1 mg/kg was 20/34 (58.9%) and 18/36 (50.0%) in the adalimumab and placebo arm, respectively (OR 1.43, 95% CI 0.54 to 3.80, p=0.46). A per-protocol sensitivity analysis on the 60 patients having received the planned treatment also gave non-significant results: 63.0% and 51.5% in the adalimumab and placebo arm, respectively (OR 1.60, 95% CI 0.55 to 4.67, p=0.38). A post-hoc analysis on the 50 patients with positive biopsy did not see any difference in the number of patients in remission at 26 weeks with a prednisone dose less than 0.1 mg/kg between groups: 15/22 (68.2%) and 14/28 (50.0%) in the adalimumab and placebo arm, respectively (OR 2.14, 95% CI 0.64 to 7.19, p=0.21). At week 52, 14/22 (63.6%) and 22/31 (71.0%) patients, in the adalimumab and placebo groups, respectively, were in remission with a prednisone dose less than 0.1 mg/kg (OR 0.72, 95% CI 0.21 to 2.42, p=0.58).
At inclusion, the mean prednisone daily dose was 0.70 mg/kg±0.08 in the adalimumab arm and 0.70±0.07 in the placebo arm. The mean change of prednisone daily dose over time is illustrated in figure 2. At week 26, the mean prednisone daily dose was 0.12 mg/kg±0.05 in the adalimumab arm and 0.13 mg/kg±0.07 in the placebo arm. The mean prednisone daily dose decreased to 0.10 mg/kg (±0.1) in both groups at week 52. The adjusted between-group difference over the week 26 period was −0.01 mg/kg per day (95% CI −0.07 to 0.05, p=0.77), and −0.02 (95% CI −0.10 to 0.07, p=0.71) over the 52-week period.

Mean prednisone daily dose from baseline until week 52 in adalimumab and placebo arms.
Seventy relapses were observed in 46 patients (20/27 in the adalimumab group and 26/35 in the placebo group). In Kaplan–Meier survival analysis, 76.0% and 71.8% of patients relapsed in the adalimumab and placebo groups, respectively. Among them, 14 patients had two flares and five patients had three flares. Among the 70 flares, 36 (51.4%) were diagnosed on an increase in CRP levels, 24 (34.3%) on the reappearance of clinical symptoms and 10 (14.3%) on both. Among the 34 relapses with clinical signs (with or without elevation of CRP), 13 and 21 occurred in the adalimumab and placebo groups, respectively (p=0.91). Overall, the number and repartition of relapses diagnosed on clinical, biological or both signs did not differ between the placebo and adalimumab groups.
The median time to first relapse was 24 weeks (95% CI 17 to 31) in the adalimumab group and 17 weeks (95% CI 11 to 29) in the placebo group, and did not differ between the two groups (figure 3, p=0.51).

{kind=link}
{kind=link}
{kind=link}
Survival curves of first relapse by group according to the Kaplan–Meier method.
Safety
In the adalimumab group, 24 (70.59%) patients experienced at least one adverse event compared to 35 (97.22%) in the placebo group (table 3). Serious adverse events occurred in five (14.71%) and 17 (47.2%) patients in the adalimumab and placebo arms, respectively. Two patients died in the placebo arm, one at week 4 from septic shock and one at week 26 from cancer. In the adalimumab group, one patient died at week 8 from severe pneumonia with septic shock; however, because consent was withdrawn, he had not received any injection of the study drug. Serious infections occurred in three patients in the adalimumab arm (one shingles and two pneumonia) and in five patients in the placebo arm (one pneumonia, one cellulitis of the forearm, one diarrhoea due to Campylobacter jejuni infection, one diverticular sigmoiditis and one septic shock). Cancer was observed in one patient in each group (one breast cancer in the adalimumab group and one lung adenocarcinoma in the placebo group).
Adverse events
Discussion
This study confirms that the majority of patients with GCA improved with an initial 0.7 mg/kg per day prednisone treatment, but that only half of them are in remission with less than 0.1 mg/kg per day by week 26. The initial adjunction of adalimumab therapy did not allow for a more rapid tapering, or a significantly greater number of patients who could reduce their oral glucocorticoid dosage to 0.1 mg/kg per day by week 26, compared with those given placebo injections. In addition, it did not allow for a lower relapse rate or a delayed time to first relapse, and it was not associated with a worse safety profile in this elderly population.
In most patients, prednisone alone was sufficient to allow for satisfactory clinical control of the systemic inflammation. However, the disease is often persisting or relapsing, as evidenced by the difficulties in reducing the prednisone doses below the level of 0.1 mg/kg per day (primary outcome achieved in only 50% of the patients) and the very high rate of relapses in the present study.
It is widely established that treatment with corticosteroids must be tapered, but no consensus exists on how rapidly it should be done. In clinical practice, up to 40–48% of patients with GCA have relapsing disease and require corticosteroid therapy for several years.3 ,24 Most relapses occur during the first 2 years of treatment.
Our study has a number of limitations. First, the planned protocol for prednisone tapering was quite rapid and probably includes less prednisone than is generally used in clinical practice, at least in some European countries. It is the reason why we decided to exclude patients with visual symptoms. The schedule of adalimumab may also be discussed. In some granulomatous diseases (Crohn's disease), a higher dose (40 mg weekly) may be requested. However, GCA concerns elderly patients with comorbidities, and higher doses could have been more toxic. The adalimumab 10-week regimen may also be questioned, but in vasculitis a short course of high immunosuppression may be enough to break inflammation and to allow faster tapering of corticosteroids, which was our objective. Also the definition of relapse in the present study was quite large and clinical relapses might be diagnosed on rather vague and non-specific symptoms without an increase of acute-phase reactants and/or a mild increase of acute-phase reactants. This definition of flare may have resulted in a high estimate of disease flares. Finally, we stopped the inclusion before having reached the planned number of patients, decreasing the power from 80% to 72%. However, even if we had included more patients, the chance to show any difference between the two groups was unlikely to occur. Also, seven patients in the adalimumab group did not receive the planned treatment; however, if the seven patients were all responders, the primary endpoint would never have been reached (data not shown).
Two other placebo controlled trials have tested the hypothesis that anti-TNF agents could reduce corticosteroid exposure in patients with GCA: one study evaluating the effect of infliximab in 44 patients newly diagnosed with GCA,17 and a smaller study evaluating the effect of etanercept in 17 patients in remission with GCA and experiencing corticosteroids side effects.16
The first trial included patients who had already obtained remission with corticosteroids. As in our study, the corticosteroid dosage was tapered rapidly (such that all patients stopped receiving steroids within 6 months), but anti-TNF was administered for a much longer period (22 weeks). That study failed to demonstrate any effect of infliximab on relapse prevention or corticosteroid intake. A similar protocol conducted in patients with polymyalgia rheumatica failed to demonstrate the efficacy of infliximab in preventing relapse.1
The second trial showed a significant corticosteroid-sparing effect of etanercept, and four out of eight (50%) and two out of nine (22.2%) in the etanercept and placebo groups, respectively, were able to discontinue corticosteroids (difference not reaching significance). That trial involved a different patient population and the anti-TNF regimen was much more prolonged (12 months’ duration) than in our study.
Based on those results and that of the present study, and as is stated in the European League Against Rheumatism recommendations,25 it is likely that anti-TNF agents might not be used widely in GCA patients. However, in our study, we excluded severe patients with GCA-related visual involvement or cerebrovascular accidents and we restricted inclusion to patients with new-onset never-treated GCA. Therefore, it could not be excluded that anti-TNF agents might be interesting in more severe or refractory or cortico-dependant GCA patients.
Our results are quite reassuring regarding the safety profile of anti-TNF treatment, even in this aged and at-risk patient population. It may be due to the use of a short 10-week anti-TNF treatment regimen. This original regimen might be interesting as an induction treatment in some severe forms of inflammatory diseases potentially sensitive to anti-TNF therapy even in at-risk patients and even in association with high-dose steroids.
Except for a possible effect of methotrexate,5 no other medication had proved its efficacy in reducing exposure to corticosteroids in patients with GCA. The growing understanding of the pathogenesis of GCA has led to a re-evaluation of the involvement of different cytokines.26 Beyond the possible involvement of TNF in pathogenesis of GCA, there is also evidence for the involvement of interleukin (IL)-6.27–29 As suggested by recent reports of the efficacy of tocilizumab (anti-IL-6 monoclonal antibody) in patients with refractory/relapsing disease, the blockade of IL-6 is under investigation to evaluate clearly the potential benefit of this drug in both GCA and polymyalgia rheumatica.30–32
Conclusion
In patients with GCA, a 10-week treatment of adalimumab, associated with a classic dose of steroids did not allow for a greater number of patients in emission with less than 0.1 mg/kg of steroids at 6 months, and was not associated with a corticosteroid-sparing effect or a lower rate of relapse. The safety profile of this short-term regimen of anti-TNF therapy was quite reassuring in this group of aged patients with comorbidities and co-treatments, which is encouraging for future and ongoing trials of other biological agents in GCA.
Acknowledgments
The authors are indebted to all investigators of the study (list below), to Isabelle Hoffman and the staff from URC Paris Nord. List of investigators: Daniel Adoue, Department of Internal Medicine, Toulouse, France; Erik Arnaud, Department of Internal Medicine and Gerontology, CHU de Nîmes, Nîmes, France; Claude Bachmeyer, Department of Internal Medicine, Hopital Tenon, Paris, France; Jean-Francois Besancenot, Department of Internal Medicine, Dijon, France; Boris Bienvenu, Department of Internal Medicine, Caen, France; Gilles Bolla, Department of Internal Medicine and Rheumatology, Cannes, France; Bernard Bonnotte, Department of Internal Medicine and Immunology, Dijon, France; Gregoire Cormier, Department of Rheumatology, La Roche sur Yon, France; Emmanuelle Dernis, Department of Rheumatology, Le Mans, France; Robin Dhôte, Department of Internal Medicine, Bobigny, France; Olivier Fain, Department of Internal Medicine, Bondy, France; Jean-Louis Feldmann, Department of Rheumatology, Argenteuil, France; Nicole Ferreira-Maldent, Department of Internal Medicine B, Tours, France; Philippe Goupille, Department of Rheumatology, Tours, France; Loïc Guillevin, Président of the Groupe d'Etudes et de Recherche sur les Vascularites; David Launay, Department of Internal Medicine, Lille, France; Sylvie Le Seaux, Department of Internal Medicine, Draguignan, France; Philippe Letellier, Department of Internal Medicine, Caen, France; Florence Lévy-Weil, Department of Rheumatology, Argenteuil, France; Denis Mulleman, Department of Rheumatology, Tours, France; Laurent Perard, Department of Internal Medicine, Lyon, France; Thomas Quémeneur, Department of Internal Medicine and Nephrology, Valenciennes, France; Jean Taillandier, Department of Gerontology, Villejuif, France; Philippe Vanhille, Department of Internal Medicine and Nephrology, Valenciennes, France; Remi Vatan, Department of Internal Medicine, Laval, France.
References
Supplementary materials
Lay summary
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Handling editor Tore K Kvien
-
Contributors Study conception and design: XM and PR. Acquisition of data: all authors and all authors listed in the acknowledgements. Analysis and interpretation of data: all authors. Drafting and revising of the manuscript: RS, XM and all authors. Final approval: all authors.
-
Funding This study was sponsored by Assistance Publique-Hopitaux de Paris and received an unrestricted research grant from Abbott. Abbott did not play any role in the design, conduct, interpretation and reporting of the study.
-
Competing interests EH received consulting fees/lecture honoraries (less than €10 000 each) from Roche, Abbott. XP has been an investigator and national coordinator of studies evaluating adalimumab therapy in rheumatoid arthritis, which were partially funded by Abbott, and is the investigator of a study evaluating tocilizumab in giant cell arteritis, which is funded by Roche.
-
Ethics approval The study protocol was approved by the institutional review boards or committees for the protection of persons at the individual study sites. The study was conducted according to the current regulations of the International Conference on Harmonisation guidelines and the principles of the Declaration of Helsinki.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.