Article Text

Abstract
Background and objectives Therapeutic monoclonal antibodies are effective drugs for many different diseases. However, the formation of anti-drug antibodies (ADA) against a biological can result in reduced clinical response in some patients. Measurement of ADA in the presence of (high) drug levels is difficult due to drug interference in most assays, including the commonly used antigen binding test (ABT).
Methods We recently published a novel method which enables the measurement of complexed antibodies against adalimumab (an anti-TNF antibody) in the presence of drug. Here we use this pH-shift-anti-idiotype ABT (PIA) to measure anti-adalimumab antibodies (AAA) in 99 rheumatoid arthritis (RA) patients treated for up to 3 years with adalimumab.
Results 53 out of 99 RA patients produced AAA. In 50 of these PIA positive patients, AAA could be detected within the first 28 weeks of treatment. Patients in which AAA could be detected in the PIA after 28 weeks of treatment were more prone to declining adalimumab levels (<5 µg/ml) (p<0.01) and high AAA levels which could be detected in the ABT (p<0.05) at later time points. We observed transient AAA formation in 17/53 patients.
Conclusions Results show that AAA develop early in treatment. However, levels that completely neutralise the drug may be reached much later in treatment. Furthermore, the patients positive for PIA at 28 weeks have an increased chance to develop clinical non-response due to immunogenicity. In some of the patients, AAA formation is transient.
Statistics from Altmetric.com
Introduction
The introduction of therapeutic monoclonal antibodies has given a major boost to the treatment of diseases such as inflammatory bowel disease, ankylosing spondylitis, multiple sclerosis and rheumatoid arthritis (RA).1–6 In many cases these biological agents have proven to be very successful in clinical practice. However, in some patients clinical benefit diminishes in time, due to the formation of anti-drug antibodies as described for adalimumab, infliximab and natalizumab.6–10
In the case of adalimumab, the formation of anti-adalimumab antibodies (AAA) has been linked to lower adalimumab serum levels and loss of clinical response.4 ,7 ,8 ,11–14 In these studies, the reported frequency of AAA detection varies between 0.74% and 31.4%. This large variation may be caused by differences in patient groups, time of follow-up, timing of blood withdrawal, co-medication and drug dosing. In addition, different assay formats used for the measurement of AAA will also greatly affect results. Most studies on AAA formation use assays which are sensitive for drug interference, leading to false negative results for AAA in the presence of adalimumab and an underestimation of AAA formation.
Moreover, in previous studies using our standard antigen binding test (ABT), which is sensitive for drug interference, some patients appeared to be transiently positive for AAA. This might indicate that some people develop tolerance against adalimumab, as has been previously described for factor VIII.15 However, the disappearance of these antibodies is most often accompanied by an increase of adalimumab levels, which makes it impossible to distinguish between patients in which AAA truly disappear over time, and false negative results due to drug interference. To obtain insight into transient AAA formation and to enable the study of tolerance induction in these patients, an AAA assay is needed that does not suffer from drug interference.
Recently, we reported such a novel assay for the measurement of AAA: the pH-shift-anti-idiotype ABT (PIA). The assay is based on acid dissociation of adalimumab–AAA complexes and prevention of reformation by addition of excess rabbit anti-idiotype fab on neutralisation. This allows for the measurement not only of ‘free’ or excess AAA, but also of so-called ‘complexed’ AAA in the presence of adalimumab (≤24 µg/ml). Detection of AAA using PIA in a small group of 30 adalimumab treated RA patients showed AAA formation in 21 of these patients in the first half year of treatment.16
Here we tested 3-year follow-up samples of 99 adalimumab treated RA patients to investigate the time course of AAA formation and to study the frequency and clinical significance of complexed AAA. In addition, PIA measurements allow us to study potential tolerance induction in these patients.
Materials and methods
Patients
Sera were obtained in the first 3 years of adalimumab treatment from the first 99 consecutive RA patients of a prospective observational cohort as previously described.7 All patients had a disease activity score in 28 joints (DAS28) of ≥3.2 and fulfilled the American College of Rheumatology 1987 revised criteria for RA. Despite earlier treatment with two disease-modifying anti-rheumatic drugs, including methotrexate, all patients had active disease at the start of adalimumab (Abbott, Illinois, USA) treatment. This was according to the Dutch consensus statement on the initiation and continuation of tumour necrosis factor (TNF) blocking therapy in RA.17 All patients used 40 mg adalimumab every other week by subcutaneous injection. In patients with an inadequate response, as judged by the treating rheumatologist, dose could be increased to 40 mg every week (n=20). All blood samples were withdrawn just prior to the next adalimumab injection. Blood samples were withdrawn prior to the start of adalimumab treatment and at 4, 16, 28, 40, 52, 78, 104, 130 and 156 weeks after start of treatment. The study was approved by the ethics committee of the Slotervaart Hospital and the Jan van Breemen Research Institute/Reade.
Production of adalimumab F(ab')2 and rabbit anti-idiotype Fab fragments
Adalimumab F(ab')2 fragments and rabbit anti-idiotype Fab fragments, were prepared as described previously.16
Measurement of adalimumab concentration
Adalimumab levels were measured by ELISA as described previously.16
Measuring AAA by ABT
The test was essentially carried out as described previously.16 ,18 ,19 In short, antibodies were captured using protein A sepharose and AAA were detected using 125I labelled F(ab')2 adalimumab diluted in Freeze buffer (Sanquin). Antibody levels were compared to a standard serum containing AAA levels and expressed in arbitrary units (AU/ml). Patients were said to be positive for AAA if at one time point AAA were above the cut-off of 12 AU/ml. All baseline samples were below the cut-off of 12 AU/ml.
pH-shift-anti-idiotype ABT
Patient serum (30 μl) diluted 1/30 in PA buffer (phosphate buffered saline/0.3% bovine serum albumin) was mixed with 30 μl of 0.1 M glycine–HCl (pH 2.5). After 30 min incubation at room temperature 30 μl of rabbit anti-idiotype Fab (67 μg/ml diluted in PA) was added. Then the pH was neutralised by addition of 30 μl of 0.2 M Tris. AAA levels were measured in the ABT. Cut-off was determined to be 48 AU/ml, based on the measurements on all available pretreatment sera of the 99 patients (145 sera) (mean+3 SD). All baseline sera were below the cut-off in the PIA. Rheumatoid factor did not interfere with the measurements in the PIA.
Statistical analyses
To show differences between groups we used the independent sample t test, Mann–Whitney U or χ2 test as appropriate. For estimating the proportion of patients positive in the PIA or ABT we used a log rank test. For calculation of the predictive value of the PIA, a χ2 test was used.
Results
Patients
In this study we have followed the first 99 consecutive patients of a cohort of RA patients during 3 years of adalimumab treatment. The median follow-up was 156 weeks (IQR 40–156 weeks) and 58 patients completed the 3-year follow-up. Forty-one patients dropped out of the study: 16 due to treatment failure, 14 due to adverse events, while the remaining 11 stopped treatment due to other reasons such as relocation (n=5), unwillingness to participate (n=3) or loss to follow-up (n=3).
Time course of AAA development
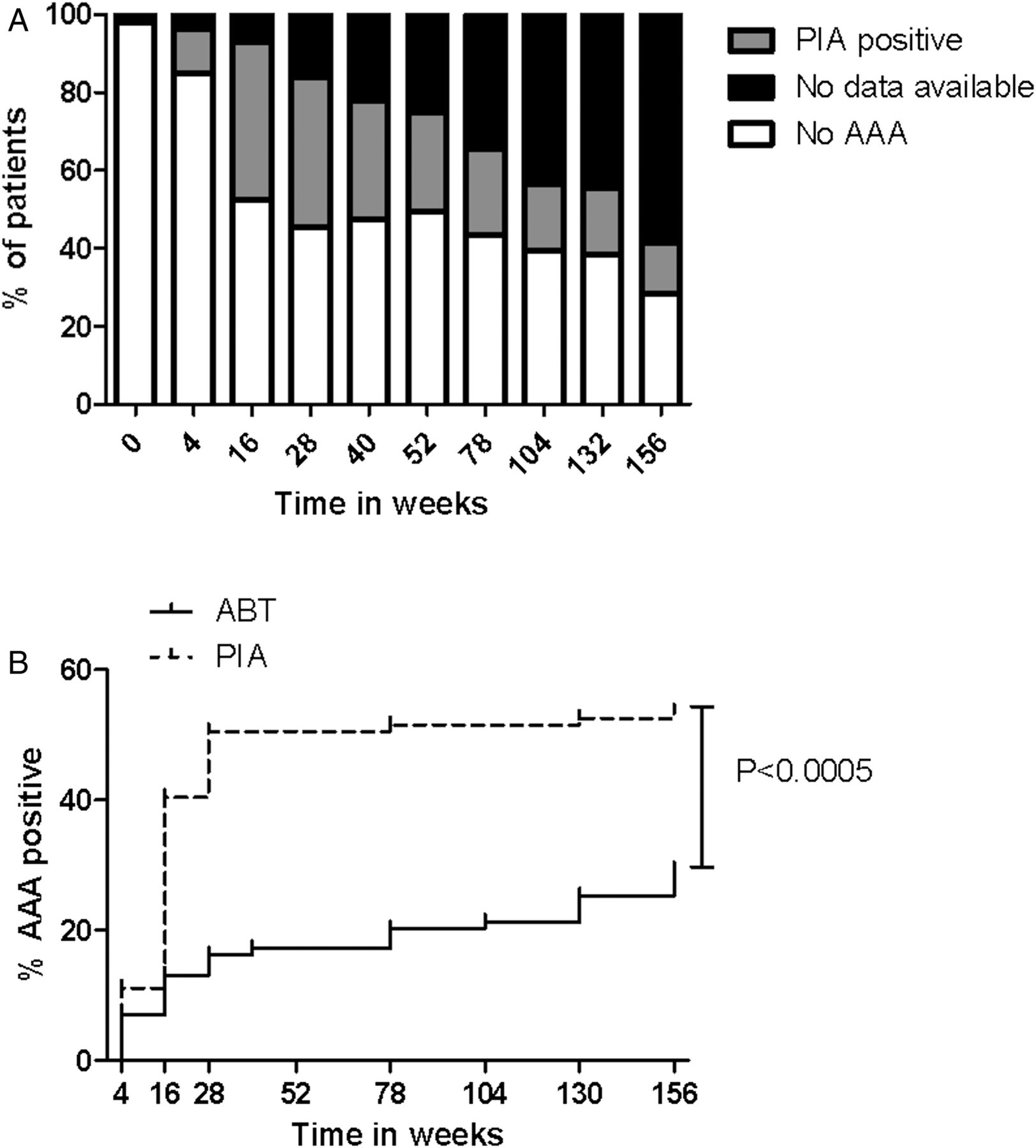
In 54% of the patients, AAA were detected at least once by PIA during 3 years’ follow-up. Figure 1A shows the number of patients that tested positive or negative at the different time points in the PIA. At baseline all patients tested negative in the PIA. In figure 1B the cumulative percentage of AAA positive patients is shown for the PIA and the for drug interference-sensitive ABT.16 ,20 The PIA is able to pick up AAA in more patients (54% vs 29%) and in many patients is able to do so at an earlier time point in comparison to the ABT (log rank test p<0.0005).

Long-term measurements of anti-adalimumab antibodies (AAA) in a group of 99 rheumatoid arthritis patients. (A) The number of patients in which AAA can be detected in the pH-shift-anti-idiotype ABT (PIA) (grey) or AAA negative patients (white) and the number of missing data (black) at the different time points during 3 years of follow-up. (B) The cumulative percentage of patients positive for AAA in the PIA (dotted line) and the antigen binding test (black line) during 3 years of adalimumab treatment. ABT, antigen binding test.
Furthermore, measurements with the PIA show that 51/53 patients (94%) producing AAA already do so in the first 28 weeks of treatment (figure 1B). Using the standard ABT, many patients appear to start making AAA at later time points. However, the present results imply that this refers to a point in time when AAA production exceeds adalimumab levels, since only in that case can AAA be measured in the ABT.21
We divided patients into three groups: patients negative for AAA at all time points in both assays, patients with ‘complexed AAA’ (negative in the ABT at all time points but positive in the PIA at least once), and patients positive for ‘free AAA’ (positive in the ABT at least once). All but two patients positive for free AAA were also positive for complexed AAA, as may be expected. These two patients were positive in the ABT at either one or two time points, but never in the PIA. For one of these patients, AAA levels were low (12 AU) and therefore might be undetectable in the PIA. For the other patient 153 AU could be detected in the ABT, but measurements in the PIA were negative. Baseline characteristics for the three groups described above as well as the total patient population are shown in table 1. Baseline C-reactive protein (CRP) and DAS28 were statistically lower in patients without AAA compared to patients with AAA. Furthermore, AAA negative patients and patients with complexed AAA had a significantly higher frequency and dose of concomitant methotrexate usage. Furthermore, methotrexate dose was lower in free AAA positive patients compared to patients with complexed AAA.21 ,22
Characteristics at baseline of patients who did or did not develop AAA during 3 years of follow-up
Clinical relevance of AAA measured in the PIA
Twenty-two out of 70 ABT-negative patients (thus either without AAA or having complexed AAA only) reached sustained remission during the follow-up period. Sustained remission is defined as patients who have a DAS28 of less than 2.6 at all consecutive measurements after a certain time point, with a minimum of two measurements of less than 2.6 for patients who discontinued treatment prematurely. In contrast, none of the 29 patients with free AAA reached sustained remission (p<0.001; figure 2A). Comparing PIA positive and PIA negative patients does not show a statistically significant difference in the number of patients reaching sustained remission (figure 2B). To further investigate this, PIA positive patients were subdivided into patients with both free and complexed AAA (PIA and ABT positive: n=27), and patients with only complexed AAA (PIA positive, ABT negative: n=26) (figure 2C). Patients with both free and complexed AAA were less likely to reach sustained remission, compared to PIA negative patients (p<0.01) and patients with only complexed AAA (p<0.001). There was no significant difference in clinical response between ABT negative patients and patients with complexed AAA (p=0.4).

The relationship between anti-adalimumab antibodies (AAA) formation in either the antigen binding test (ABT) or the pH-shift-anti-idiotype ABT (PIA) and clinical response. The percentage of patients who reached sustained remission (disease activity score in 28 joints <2.6) for patients with or without AAA at at least one time point during follow-up as measured in the ABT (A) and PIA (B) or patients with free and complexed AAA (PIA and ABT positive), only complexed AAA (PIA positive, ABT negative) or no AAA (PIA negative) during 3 years of treatment (C).
Predictive value of PIA measurements for future treatment failure
We investigated whether the presence of complexed AAA will eventually result in a stronger immune response capable of clearing adalimumab and leading to the presence of free AAA which can be detected in the ABT. Therefore we looked at all patients negative in the ABT after 28 weeks of treatment, who completed a minimal follow-up of 40 weeks (n=63) (figure 3A). These patients were divided into PIA-wk28 negative (n=38) and PIA-wk28 positive (n=25) patients based on measurements at t=28 weeks. In 3/38 of the PIA-wk28 negative patients, free AAA could be detected in the ABT during subsequent follow-up. In contrast, 9/25 of the PIA-wk28 positive patients developed free AAA in at least one available serum (p<0.01). There was no difference in length of follow-up between the four different patient groups (PIA-wk 28 positive/negative ABT positive/negative) This shows that PIA-wk28 positive patients have an increased chance of developing free AAA, which can be detected in the ABT (figure 3B).

The predictive value of measuring anti-adalimumab antibodies (AAA) in the pH-shift-anti-idiotype ABT (PIA) after 28 weeks of treatment. (A) Flow chart of the 99 patients in which the predictive value of measuring AAA in the PIA after 28 weeks was investigated. (B) The percentage of patients in which free AAA are detected during follow-up in PIA positive and negative patients after 28 weeks of treatment. (C) The percentage of patients having low adalimumab levels (<5 µg/ml) at the end of treatment in PIA positive and negative patients, as measured after 28 weeks of treatment. ABT, antigen binding test.
We also investigated whether PIA-wk28 positive patients have an increased chance of having low adalimumab trough levels (<5 µg/ml), as detected in the last available serum. As shown in figure 3C, 9/25 of the PIA-wk28 positive patients have low adalimumab levels at the end of treatment, while only 4/38 of PIA-wk28 negative patients have low adalimumab levels (p<0.05).
Transient AAA production
Using the ABT for the detection of AAA, we have observed transient AAA production in 11 of the 99 patients studied here (four representative patients shown in figure 4A,B). Antibody formation was considered to be transient if AAA measurements were above the cut-off at any time point during treatment and negative at the last available time point. This disappearance of AAA in the ABT is often accompanied by an increase of drug levels (n=10). Since the ABT is sensitive for drug interference, the ABT did not enable us to determine whether the disappearance of AAA was the result of a transient immune response, or the effect of false negative results due to drug interference. Measurements using the PIA show that in only four of these patients was the AAA response confirmed to be truly transient (two representative examples shown in figure 4A). In the remaining six patients AAA levels were being masked by increased drug levels (n=6) (representative figures shown in figure 4B). In two of these patients this could be explained by dose increase. The last patient was only weakly positive (12 AU/ml) in the ABT and no AAA were detected using the PIA (not shown).

The course of adalimumab levels and anti-adalimumab antibodies (AAA) levels as measured in the antigen binding test (ABT) and the pH-shift-anti-idiotype ABT (PIA) in single patients. All values below the cut-off of 12 AU/ml in the ABT or 48 AU/ml in the PIA are plotted as 5 AU/ml. (A) Two representative patients with transient AAA production measured in the ABT and PIA. (B) Two examples of patients with transient AAA production measured in the ABT and persistent AAA positivity in the PIA. (C) Two examples of patients negative in the ABT and transiently positive in the PIA.
The PIA also showed transient AAA formation in 13 patients in which no antibodies were detected in the ABT (figure 4C). There was no clear link between dose increase in some patients and transient AAA production. In total these data show that in 17/53 patients producing AAA, this antibody response was transient as measured by the PIA.
Discussion
Here, we present long-term data on AAA levels measured in the PIA in a group of 99 adalimumab treated RA patients and show that 53/99 patients produce AAA. We show that complexed AAA measured only in the PIA, are not linked to a reduction in clinical response, while AAA measured in the ABT are. Due to drug interference, the ABT can only detect AAA if adalimumab levels are low. Hence, it seems that the most important variable governing clinical response is the adalimumab concentration (figure 5). However, in patients who continue to make high levels of complexed AAA, functional adalimumab levels drop, eventually allowing for the detection of AAA in the ABT and leading to a loss of clinical response.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Model for the clinical effect of anti-adalimumab antibodies (AAA) development. We propose that AAA development only results in clinical non-response if it results in low functional adalimumab levels. ABT, antigen binding test; ADA, anti-drug antibodies; PIA, pH-shift-anti-idiotype ABT.
The question remains why some patients develop low levels of AAA which can only be detected in the PIA, while other patients develop higher levels of AAA which can also be detected in the ABT. The results shown in table 1 suggest that patients who produce high levels of AAA have a higher disease activity at the start of treatment and that concomitant methotrexate use lowers the risk of high level AAA production as previously described.6 ,23
Although not directly linked to reduced clinical response, AAA measurement using the PIA might provide a predictive tool for development of free AAA and loss of therapeutic levels of adalimumab. We find that in 94% of the patients positive in the PIA, AAA can be detected within the first 28 weeks of treatment. The detection of AAA in the PIA at 28 weeks of treatment is indicative for a future decline of adalimumab levels (<5 µg/ml) due to potentially increased AAA production. PIA measurements after 28 weeks might provide insight into which patients are at risk of developing free AAA. These patients might benefit from more close monitoring.
It would be very interesting to see whether there is a link between HLA types and AAA formation. Such a correlation has been described for the immunogenicity of factor VIII used for the treatment of patients with haemophilia.24 ,25 Some HLA types might have a higher affinity for adalimumab peptides, leading to more efficient peptide presentation and therefore increased AAA formation. Investigation of the HLA types that are linked to AAA formation might allow the identification of patients at risk of developing AAA. For at-risk patients it might be more beneficial to be treated with another available anti-TNF agent.
Our results suggest that many patients have complexed AAA. Previous data from our group show that these are present in the form of small immune complexes, which suggests that many patients are continuously exposed to large numbers of small immune complexes.26 We can only speculate what the effect of these complexes might be in clinical practice. On the one hand, small immune complexes might block FcγR, being too small to signal efficiently yet binding stronger than monomeric IgG. On the other hand, in systemic lupus erythematosus and serum sickness, long-term exposure to small immune complexes leads to an increased risk of type III hypersensitivity reactions. A recent paper has shown a link between AAA production and increased risk of thromboembolic events.27 It would be interesting to study whether this is correlated to the presence of small immune complexes in these patients.
Our data also show transient AAA production in 17/53 patients that were AAA positive. The median length between the first AAA positive serum sample and the first AAA negative thereafter was 50 weeks (range 12–114 weeks). Due to the large drop-out numbers and the extended time of AAA formation in transiently positive patients, we were not able to study the clinical relevance of transient AAA formation. Investigation of transient AAA production in more detail might allow us to investigate the possibility to induce tolerance as described for factor VIII.28 In factor VIII treatment, tolerance induction is achieved by long-term exposure to high levels of factor VIII (∼15 µg/kg every 12 h; Bonn protocol).15 However, because of the differences in dosing between adalimumab (40 mg every other week) and factor VIII (1.5–7.5 µg/kg every 2–3 days), such an immune tolerance induction protocol might be difficult to achieve for adalimumab treatment. Moreover, due to the possibility of switching towards other types of biological agents, the need of tolerance induction against adalimumab might be limited compared to factor VIII.
A previous study by Maini et al3 has shown that increased dosing of infliximab leads to reduced immunogenicity, suggesting that high levels of drug might induce tolerance in these patients. However, an alternative explanation for these results could be that, in patients receiving high drug dosing, the presence of residual drug levels might interfere with the detection of anti-infliximab antibodies. It would be very interesting to measure antibodies in these samples using an anti-infliximab PIA to confirm whether high dosing indeed reduces immunogenicity of therapeutic monoclonal antibodies.
In conclusion, this study, which follows AAA formation measured by the PIA in 99 RA patients, shows that the clinical relevance of measuring AAA in the PIA is limited, although it does have a predictive value. Importantly, PIA measurement gives insight in the immune response against adalimumab because it is able to detect AAA in the presence of adalimumab. It shows that 94% of the patients who produce AAA develop these antibodies in the first half year of treatment. Measurements with the PIA also allow the study of transient AAA formation, which we found in 32% of the AAA positive patients. Moreover, these data underline the importance of the quantity of an AAA response. Only the formation of high levels of AAA leads to low functional adalimumab levels and reduced clinical response.
Footnotes
-
Handling editor Tore K Kvien
-
Contributors Study concept and design: PAvS, CLK, TR, LA, GJW and DW Acquisition of data: PAvS and CLK. Analysis and interpretation of data: PAvS, CLK, TR, LA, GJW and DW. Clinical revision of the manuscript for important intellectual content: PAvS, CLK, TR, LA, GJW and DW. Obtained funding: GW. Study supervision: LA, GJW and DW.
-
Competing interests None.
-
Funding GJW reports having received a research grant from Wyeth Pharmaceuticals and honoraria for lectures from Amgen and Pfizer. LA has received honoraria for lectures from Abbott, Roche, and Pfizer. TR has received honoraria for lecture from Pfizer. Funding of this study was provided by an unrestricted grant of Wyeth Pharmaceuticals. Wyeth Pharmaceuticals had no involvement in the study design; in the collection, analysis, and interpretation of data; in the writing of the manuscript; or in the decision to submit the manuscript for publication.
-
Ethics approval The study was approved by the ethics committee of Slotervaart Hospital and the Jan van Breemen Research Institute/Reade.
-
Provenance and peer review Not commissioned; externally peer reviewed.