Article Text

Abstract
Rheumatoid arthritis (RA) is a chronic inflammatory disease which is associated with an increased cardiovascular (CV) burden. Whether the risk is already present at the time of RA diagnosis remains a key area of debate. The aim of this review was to evaluate the existence of both subclinical CV changes, including endothelial dysfunction and atherosclerosis, CV risk factors, as well as CV disease manifestations such as coronary heart disease, myocardial infarction, congestive heart failure and CV death prior to RA diagnosis and during the first few years of the disease. The state of the endothelial function remains controversial in patients with newly diagnosed RA. Studies with impaired brachial artery vasodilatory responses at baseline showed a reversal of the dysfunction after 6–12 months of anti-inflammatory therapy. Morphological evidence of arterial wall atherosclerosis, measured by carotid artery intima-media thickness or the prevalence of carotid plaques, was already present during the first year following RA diagnosis. The risk of coronary heart disease and myocardial infarction is increased even prior to and, at the latest, within 1 year of the clinical onset of RA. The prevalence of hypertension was similar among patients with RA and controls. CV mortality may not increase within the first years of RA diagnosis. In conclusion, the CV risk seems to increase sooner after the RA diagnosis than previously thought. In addition to systematic CV risk assessment, patients with early RA might benefit from being targeted with stricter than conventional CV risk prevention and intervention.
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory disease associated with a wide spectrum of comorbidities especially of cardiovascular (CV) origin.1 These coexisting conditions have profound effects on different RA outcomes, including mortality, work disability and quality of life.2 ,3 Many cross-sectional and longitudinal studies have confirmed an increased risk of both atherosclerosis and consequent CV disease among patients with established RA,4 ,5 although contemporary early and effective RA drug therapy may reduce the excess CV mortality.6–8
During the past few decades it has become increasingly acknowledged that the early years of RA are of utmost importance with regard to many aspects of the disease; for example, effective drug therapy early in the course of the disease plays a pivotal role in halting the inflammation and erosive joint damage.9 ,10 This period of time just after the onset of RA when appropriate drug therapy elicits major clinical improvement is designated as the window of opportunity.11 ,12 Knowing this and the prevalence and severity of CV comorbidities complicating RA, an intriguing question arises: when does the increase in CV risk commence?
Although widely investigated, the underlying causes of the increased prevalence of CV disease among patients with RA remain to be fully elucidated.5 Information about the timing of increased CV risk in RA may help us to distinguish causal relationships from those with shared risk factors and aetiology.13 From this perspective, there are two different approaches to explaining the interplay between RA and CV disease. One scheme is that the CV risk accumulates during the RA disease course due to RA-specific factors such as immune dysregulation, systemic inflammation or treatment with oral glucocorticoids or non-steroidal anti-inflammatory drugs (NSAIDs). On the other hand, RA and CV disease may share risk factors such as genes, smoking or diet which could increase the CV comorbidity prior to the onset of RA.13–15 There is evidence concordant with both of these theories,14 ,16 ,17 suggesting a combination of the two modes of interaction.
We gathered and analysed the scope of data available on the existence of CV comorbidities prior to RA diagnosis and during the first few years of the disease. The present review highlights studies concerning both subclinical CV changes, including endothelial dysfunction and atherosclerosis, CV risk factors and CV disease manifestations such as myocardial infarction, coronary heart disease, congestive heart failure and CV death. CV effects of RA medications are summarised in applicable contexts. Our major aim is to bring attention to the high prevalence of CV comorbidities near the onset of RA and to help determine the temporal relation between increasing CV risk and RA symptom onset.
Search strategy and selection criteria
The literature search was performed using the Medline and PubMed databases. The search was conducted using multiple combinations of the following keywords and MeSH terms: ‘RA’, ‘CV disease’, ‘atherosclerosis’, ‘coronary heart disease’, ‘congestive heart failure’, ‘myocardial infarction’, ‘hypertension’, ‘hyperlipidemia’, ‘insulin resistance’, ‘recent-onset’, ‘early’, ‘newly-diagnosed’ and ‘disease duration’. The references of the detected articles were searched manually to find additional relevant reports. The retrieval of information was restricted to articles concerning CV disease prior to RA onset or during the early years of disease.
Definition of early RA
The development of established RA is a process demanding a varying period of time, even several years in some patients.18 The final outcome of inflammatory arthritis is difficult to predict at symptom onset: some patients have remission while others develop various clinical forms of chronic arthritis.18 As a consequence, it is challenging to compare studies with respect to disease duration.
The articles included in this review were heterogeneous in terms of the methods of identification of cases with new-onset arthritis. For example, studies conducted in the Norfolk Arthritis Register cohort included adults with ≥2 swollen joints lasting ≥4 weeks.19–21 This is a sensitive way of case identification and includes a large percentage of the future RA patients. However, the definition also recruits other forms of arthritis and patients who would subsequently attain permanent remission without disease-modifying antirheumatic drugs. Nevertheless, some of the included studies took this aspect into account by requiring the patients to meet classification criteria for RA afterwards21 or by excluding patients who subsequently developed conditions other than RA.20
Fulfilment of at least four out of the seven American College of Rheumatology (ACR) 1987 criteria was the method used in most of the studies included (tables 1 and 2). These criteria were not devised as diagnostic tools but for classification of patients with RA for scientific purposes.42 The sensitivity of the ACR 1987 criteria is therefore relatively low in the early phases of RA.43 If no limits for symptom duration before inclusion are confined, RA cohorts identified based on the ACR 1987 criteria are likely to include patients who have had the disease for a considerable period of time. However, it is reported that, in the Rochester Epidemiology Project RA cohort, the time from the first patient-reported joint swelling to meeting the ACR 1987 criteria was less than a week in 69% of the patients; 89% met the criteria within 6 months and 94% within 18 months.44
Studies on subclinical cardiovascular changes near the onset of rheumatoid arthritis (RA)
Studies on symptomatic cardiovascular (CV) disease near the onset of rheumatoid arthritis (RA)
In clinical work, rheumatologists may give the diagnosis of RA to patients without strict fulfilment of the ACR 1987 or ACR/European League Against Rheumatism (EULAR) 2010 criteria.18 As a consequence, the clinical diagnosis is prone to result in an RA population including earlier forms of RA than when using the ACR 1987 criteria, but still leaving out patients with mild symptoms of undifferentiated arthritis.
CV risk factors
Traditional CV risk factors
Hypertension is relatively common in RA, although whether it is more common than in the general population has not been elucidated.45 It has been suggested that hypertension among patients with RA might be underdiagnosed and insufficiently controlled.46 Higher disease activity has been associated with higher blood pressure, and successful anti-inflammatory therapy has been shown to reduce blood pressure.47
Few studies have focused on the prevalence of hypertension among newly-diagnosed RA patients, although hypertension has been a covariate in several reports. The presence of hypertension at the date of fulfilment of ACR 1987 criteria was evaluated in two Swedish cohorts as detected in the Hospital Discharge Register and as a self-reported condition.13 Both cohorts displayed a similar proportion of hypertensive subjects as controls (see supplementary online table S1). In a small case–control study comparing the extent and severity of coronary artery atherosclerosis in patients with established RA, patients with early RA and controls, the prevalence of hypertension was 67.6%, 38.6% and 38.4%, respectively.33
Two studies addressed the prognostic value of traditional CV risk factors such as hypertension in the evaluation of CV risk among patients with early RA; one detected hypertension in subjects who subsequently developed inflammatory polyarthritis19 and the other measured the blood pressure of RA patients at the time of fulfilment of the ACR 1987 criteria.37 Neither found differences between cases and controls.
Despite the methodological differences, all of these new-onset RA cohorts displayed a similar prevalence of hypertension in comparison with controls (see supplementary online table S1). This suggests that the increase in blood pressure in patients with RA, if it even exists, may require a considerable period of time to develop from the onset of RA. A recent 5-year prospective study following patients with new-onset RA showed an increase in the treatment of hypertension from 24.5% to 37.4%.48 It is possible that an increase in blood pressure after RA diagnosis arises from hypertension-inducing RA medications such as glucocorticoids, some disease-modifying antirheumatic drugs and NSAIDs in particular.45
Depressed levels of high-density lipoprotein (HDL) cholesterol invariably characterise early RA in different studies whereas the levels of total or low-density lipoprotein (LDL) cholesterol are not equally uniform. Some studies support a typical proatherogenic lipid profile in early RA, more specifically higher serum levels of total cholesterol, LDL cholesterol and triglycerides but lower serum HDL cholesterol,49 as well as smaller LDL particle size50 compared with controls. However, in other studies, patients with early RA have been characterised by relatively low concentrations of both total cholesterol and HDL cholesterol.51 A common element in these studies was a more atherogenic total cholesterol/HDL ratio among patients with early RA which improved with antirheumatic drug therapy and control of disease activity, regardless of the total or LDL cholesterol levels.49 ,51
Interestingly, 79 blood donors with forthcoming RA had a more atherogenic lipid profile than controls 10 years before the onset of RA symptoms (see supplementary online table S1).52 In multilevel regression analysis, C-reactive protein (CRP) only had a marginal influence on the differences in the lipid profiles. The authors hypothesised that a deterioration in the lipid profile might be aetiological for RA, for example, by modulating the susceptibility to inflammatory diseases, or these conditions would have a common or linked background.52 In another study the levels of total and LDL cholesterol decreased during the 5 years before the fulfilment of the ACR 1987 criteria in 577 patients with RA but not in 540 controls, whereas HDL cholesterol levels remained similar, resulting in a decrease in the atherogenic total cholesterol/HDL ratio before RA onset.53
There are suggestions that patients with early RA have higher fasting insulin levels and are more frequently insulin-resistant than controls, predisposing to CV events.54 Smoking is a clear risk factor for CV disease as well as anti-citrullinated protein antibody and rheumatoid factor (RF) positive RA,55 and smokers are more prevalent among RA patients than in the general population.56–58 Indeed, smoking might even be more prevalent among people who will develop RA in the future than among those who have already had the disease for some time, as indicated by a prospective study in which the prevalence of smoking decreased from 29.8% to 22.4% in the 5-year period after RA diagnosis.48 With regard to body composition, a large proportion of women with early RA had an unhealthy body composition phenotype, indicated by lower appendicular lean mass, higher body fat mass and higher truncal fat mass than controls.59 ,60
Non-traditional CV risk factors
Along with traditional CV risk factors, two main disease-related mechanisms have been shown to drive endothelial dysfunction and atherogenesis in systemic rheumatic diseases: the inflammatory and autoimmune pathways.16 ,61 They are induced well before the clinical onset of RA62–64 and are likely to expedite arterial wall damage from the early phases of the disease.65 They act synergistically with traditional CV risk factors in accelerating atherosclerosis in early RA: for example, both insulin resistance and atherogenic lipid levels have been shown to increase with higher CRP values.54 ,65 ,66
Elevated systemic inflammatory markers as well as other disease severity markers have been of interest as possible predictors of future CV events in early RA. For example, a raised erythrocyte sedimentation rate at baseline, a higher cumulative disease activity and progression of extra-articular disease were predictive of a new CV event in a 5-year prospective study among 442 patients with newly-diagnosed RA.48 Of the studies reporting an increased carotid intima-media thickness (IMT) or impaired vasodilatory responses among patients with early RA (figure 1, studies represented by red bars), many28 ,30–32 but not all22 ,26 showed that the subclinical CV changes correlated with CRP levels, erythrocyte sedimentation rate or disease activity score. Thus far, the evidence on the significance of these factors as promoters of CV disease in early RA is relatively scarce.
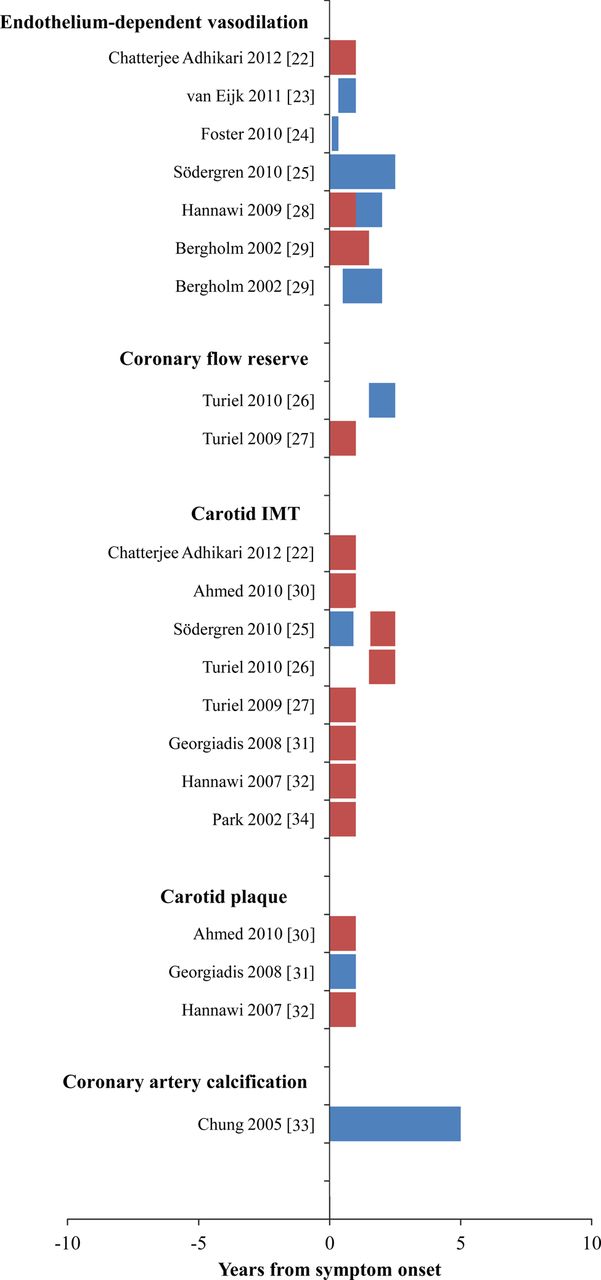
Overview of results of studies on subclinical cardiovascular (CV) changes near the onset of RA. A red bar represents an increased CV risk in terms of the parameter written above the bar in bold face whereas a blue bar represents a non-increased risk. The starting point and length of the bars represent the period of observation.
Immune-mediated mechanisms such as RF and antinuclear antibodies play a role in enhancing the CV risk in patients with established RA and among the general population.56 In early RA, antibodies against oxidised LDL30 and anti-modified citrullinated vimentin levels67 have been demonstrated to correlate positively with subclinical atherosclerosis. However, in the 5-year prospective study already mentioned, the incidence of overt CV events did not correlate with immunological mediators such as RF, anti-citrullinated peptide antibody and antinuclear antibodies during the first years of RA.48
RA medications play an important part in modulating the risk of CV events. A recent meta-analysis indicated that, although different NSAIDs have slightly different CV risk profiles, none of them is completely safe in CV terms.68 They might have unfavourable side effects such as hypertension or heart failure and they might weaken the beneficial antithrombotic effect of aspirin.69 COX-2 selective inhibitors and traditional NSAIDs do not seem to differ as promoters of thrombotic CV events.70 RA medications may also halt CV disease—in particular, methotrexate and tumour necrosis factor α (TNFα) inhibitors seem to reduce CV morbidity and mortality.6 ,71 ,72 Among patients with recent-onset RA, TNFα inhibitors reduce blood pressure47 but not the rate of clinical CV events.73
Subclinical CV changes
Pre-atherosclerotic processes
Endothelial dysfunction, the prime promoter of atherogenesis, precedes the development of morphological alterations in arterial walls and can be assessed by measuring endothelium-dependent vasodilatory responses.61 Functional impairment in endothelial activity has been commonly found to be more prevalent in patients with established RA than in healthy controls, and to be associated with inflammation74–76 as well as with certain genetic components.77 In the case of early RA, the state of endothelial function is still highly controversial (table 1, figure 1).
In three studies, patients with newly diagnosed RA showed significantly impaired brachial artery vasodilatory responses, 22 ,29 ,28 but the dysfunction was reversed after 6–12 months of anti-inflammatory therapy.28 ,29 Supporting these findings, Turiel and colleagues measured coronary flow reserve by means of echocardiography as a flow difference during dipyridamole infusion and baseline and found it to be reduced in patients with recent-onset RA.27 Even these changes improved after treatment with disease-modifying drugs and consequential control of inflammation.26 However, some studies among patients with long-standing and severe RA have only shown transient and reversible improvement of endothelial function following anti-TNF therapy.78 Also, endothelial dysfunction as well as carotid IMT have been demonstrated to increase with disease duration in patients with RA without clinically evident CV disease.79
The number of patients with early RA was very modest (roughly 20) in the abovementioned studies. Moreover, as reported recently by Södergren et al, brachial artery endothelium-dependent dilation was not compromised in a population of 79 RA patients with symptoms for less than 12 months or at follow-up in 18 months.25 The number of patients included in the study exceeded the sum of the patients in the reports mentioned in the previous paragraph. Furthermore, a recent small observational study among 18 RA patients with a median symptom duration of only 2 months revealed preserved micro- and macrovascular endothelial function but elevated levels of molecular markers of endothelial damage and abnormal endothelium-independent vasodilatory responses.24 With regard to skin microvascular dilation tests, no difference was found between controls and patients with early RA of low inflammation.23 Therefore, no firm conclusions about endothelial function during the first years of RA can be made.
Subclinical atherosclerosis
Measuring carotid IMT or coronary artery calcification is a non-invasive way of getting morphological evidence of arterial wall atherosclerotic damage. The values have been proved to be strongly associated with the risk of CV disease,80 ,81 and recent evidence shows that the internal carotid IMT offers additional value to the Framingham risk score when predicting CV events.82 Eight case–control studies with carotid IMT as a marker of atherosclerosis were included,22 ,25–27 30–32 ,34 and five of them found IMT to be significantly elevated in RA patients with a disease duration of less than 1 year (table 1, figure 1).22 ,27 ,30–32 In addition, one of the studies showed that carotid IMT continued to expand in RA of a longer duration.34 Comparably, coronary artery calcification may be more prevalent and severe in RA cohorts of long-standing disease in comparison with those with RA for less than 5 years.33
Even these RA populations were relatively small, mostly with about 40 patients (table 1). Furthermore, partly conflicting results have been published—the 79 patients with early RA already referred to regarding endothelial dysfunction had similar carotid IMT values to controls.25 However, a significant increase in the carotid IMT was demonstrated after 18 months of follow-up,25 suggesting accelerated atherogenesis early in the RA disease course.
When used in combination with carotid IMT values, carotid plaque prevalence is another marker of subclinical atherosclerosis and a predictor of ischaemic CV events.83 Two studies showed that plaques were more prevalent in early RA cohorts than among healthy controls,30 ,32 whereas one study found the prevalence to be similar among early RA cases and controls.31 As an aggregate, it seems that enhanced atherogenesis occurs soon after RA symptom onset (figure 1) and that this is subsequently ongoing.
Overt CV disease manifestations
Symptomatic CV disease
In terms of CV disease in general, CV admission rates in patients with inflammatory polyarthritis of less than 7 years have been shown to be twice as high as in the general population.35 A recent population-based cohort study in the framework of the Rochester Epidemiology Project evaluated the cumulative incidence of combined CV outcome and demonstrated an elevated absolute and relative 10-year risk of CV disease in 553 patients with recent-onset RA.36 The cumulative incidence of CV events rose steadily from the RA incidence date, and the increasing trend was notably sharper in patients with RA than in the general population, leading to a similar 10-year absolute CV risk among RA patients and non-RA subjects who were 5–10 years older.36
Coronary heart disease
Growing but still fairly limited evidence shows that the excess risk of coronary heart disease and myocardial infarction predates the full-scale establishment of RA. Again, within the Rochester Epidemiology Project, Maradit-Kremers et al reported that patients with RA were at an increased risk of coronary heart disease and myocardial infarction in the 2-year period before the fulfilment of the ACR 1987 criteria.40 On the other hand, Holmqvist and colleagues conducted a study on two large Swedish cohorts and found no evidence of an increased risk of ischaemic heart disease before the onset of RA symptoms,13 but the risk of myocardial infarction was significantly increased 1 year after RA diagnosis.39 In the latter studies, subgroups with and without RF displayed similar results.13 ,39 Recently, the findings of these studies were amplified in a Danish register study: a myocardial infarction OR of 1.7 was observed in patients with RA with treatment duration of less than 3 years.38 All in all, the timing of the rise of the risk of coronary heart disease and myocardial infarction is still controversial, although there are indications that the risk might increase slightly during the very first year after or maybe even prior to the clinical onset of RA (figure 2).

{kind=link}
{kind=link}
Overview of results of studies on symptomatic cardiovascular (CV) disease risk during the first decade of RA (ie, coronary heart disease, CV death and CV disease in general). A red bar represents an increased CV risk compared with controls whereas a blue bar represents a non-increased risk. The follow-up for the faded bars continues beyond the scale (tables 2 and 3).
Congestive heart failure
Limited evidence implies that patients with RA have an increased risk of developing congestive heart failure. The Rochester Epidemiology Project indicated that patients with RA may be at an increased risk of congestive heart failure soon after the onset of RA: the curves with cumulative incidence of congestive heart failure began to rise more sharply among the RA group than the non-RA group.41 Besides, a greater number of patients with RA than controls were excluded from the study because of pre-existing congestive heart failure, implying that the development of congestive heart failure might be accelerated even before disease onset. In this population of 575 patients with RA the relative risk of congestive heart failure remained fairly constant, almost twice as high as among the controls, throughout the long follow-up of 6–46 years.41
There are results from established RA cohorts which underline the contribution of disease-related processes in the increased risk of congestive heart failure. For example, several studies have found an association between diastolic dysfunction and RA disease duration.84–86 In contrast, disease severity rather than disease duration was also found to be associated with left ventricular diastolic dysfunction in a series of patients with RA without traditional CV risk factors.87 A more recent study from Rochester showed that some RA disease activity markers such as extra-articular manifestations, erythrocyte sedimentation rate and RF positivity increase while methotrexate reduces the risk of congestive heart failure.88
CV death
A recent meta-analysis of observational studies on CV mortality among patients with RA reported that RA is associated with a 50% increase in the risk of CV death in comparison with the general population.89 However, when considering only inception cohorts, the risk of CV death was not increased.89 Five articles found for the present review evaluated the risk of CV death among inception cohorts with some form of arthritis20 ,21 ,35 ,90 ,91 and three of these20 ,21 ,91 demonstrated CV death to be slightly increased during the first decade of the disease (table 3, figure 2).
Studies on cardiovascular (CV) death rate in arthritis inception cohorts
One study concluded that the highest rate of CV mortality was observed among RF-seropositive patients aged <55 years at symptom onset, the excess CV mortality among the RF-seropositive subgroup already being apparent 5 years after symptom onset.21 Recently, results from an English RA inception cohort reported that the mortality of patients with RA increased within the first 7 years of the disease, and coronary heart disease was mainly responsible for this reduced survival.91 On the other hand, an autopsy study indicated that coronary deaths are diagnosed less accurately in patients with RA than in non-RA subjects.92 A more frequent use of analgesics among patients with RA may suppress the ischaemic symptoms and hamper the clinical diagnosis of coronary heart disease.
However, several studies have shown contradictory results, demonstrating no increase in either CV or all-cause mortality in the first 10 years of RA.93–95 Thus, no definite conclusions on the relative CV death rate of patients with early RA can be made.90 ,91
Limitations of the study
The included articles were heterogeneous in several respects: there are differences in the definitions of RA, the selection of patients and controls, the length of follow-up, disease duration before study inclusion, methods of statistical analyses and CV outcome.
Final remarks and conclusions
CV risk assessment in patients with RA is a multifold issue. The recently published EULAR recommendations for CV risk management in patients with RA and other forms of inflammatory arthritis include an annual CV risk assessment and CV intervention along with early and effective antirheumatic treatment.96 Because the additional CV burden resulting from RA should be taken into account when using CV risk score calculators,36 these recommendations suggest a multiplication factor of 1.5 if the RA patient meets two of the following three criteria: (1) disease duration of more than 10 years; (2) RF or anti-cyclic citrullinated protein antibody positivity; and (3) the presence of certain extra-articular manifestations.96 However, these recommendations were derived mainly from mortality studies96 while symptoms of CV diseases, particularly those of coronary heart disease, manifest earlier. In addition, the increased CV burden seems not to be confined only to the RF-positive subgroup but to be elevated also among RF-negative patients.13 ,39 ,90 ,93 In the light of the present review, the abovementioned criteria might be insufficient to correct the CV risk estimates for patients with early RA.
Regarding the aetiology of RA-related CV comorbidity, a few concepts suggest the role of RA-specific processes as promoters of CV disease. The prevalence of CV changes was not as clearly increased in early RA as in established RA,33 ,34 indicating that the CV risk may accumulate with disease duration. Moreover, some reversal in the vessel wall changes was achieved after successful anti-inflammatory therapy.26 ,28 ,29 Equally noteworthy is the fact that the research settings enabled the observation of causal relationships between RA and CV disease generally better than of shared aetiological agents. Slight implications of excess CV burden preceding the onset of RA were noticeable,40 ,52 which supports the existence of similar predisposing factors between the conditions.
In conclusion, the prevalence of CV comorbidities increases in the proximity of RA diagnosis. Besides asymptomatic atherosclerosis which may accelerate in the preclinical phase of the disease, overt CV events occur at a higher than expected rate shortly after the first symptoms of RA. A window of opportunity exists with respect to RA-laden CV disease, and the window may already be closing at the time of RA diagnosis.12 ,36 Early CV risk detection as well as stricter than conventional prevention and intervention should be included in the management of RA as soon as the disease is diagnosed.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement - Online tables
Footnotes
-
Contributors AMK collected the data and drafted the manuscript with TVMN. MJK and AMK interpreted existing data and made critical revisions to the manuscript. All the authors have accepted the final version.
-
Funding The Onni and Hilja Tuovinen Fund, the Research Fund of the Päijät-Häme Central Hospital.
-
Competing interest None.
-
Patient consent Not obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.