Article Text

Abstract
Objectives To compare the effectiveness of adding synthetic disease-modifying antirheumatic drugs (sDMARDs) versus tumour necrosis factor α inhibitors (TNFi) to methotrexate (MTX) in patients with rheumatoid arthritis (RA) who were MTX inadequate responders (IR). Second, to examine outcomes in patients receiving MTX+TNFi for whom the MTX+sDMARD combination had also failed.
Methods Patients with RA (disease duration ≤ 5 years, MTX IR and naïve to other DMARDs) starting treatment with MTX+TNFi or MTX+sDMARDs were included. From the latter group a subgroup of patients who went on to receive MTX+TNFi was identified.
Results Patients receiving MTX+TNFi (n=98) and MTX+sDMARDs (n=129) had similar baseline disease activity when starting combination therapy (mean Disease Activity Score 28 (DAS28) = 4.90 and 4.96, respectively). Three- and 6-month effectiveness and 2-year drug survival were better for MTX+TNFi than for MTX+sDMARDs: mean ∆DAS28 was −1.61 versus −0.85 after 3 months (p<0.001) and −1.91 versus −1.03 after 6 months (p=0.01); DAS28<2.6 was reached by 29.0% versus 11.6% after 3 and 34.5% versus 12.9% after 6 months. Effectiveness was somewhat better with triple therapy than other MTX+sDMARD combinations but was generally inferior compared with MTX+TNFi. For the patients who received MTX+TNFi as a third step after MTX+sDMARDs had failed (n=38) there was a tendency towards lower remission rates, worse disease activity states and inferior drug survival compared with patients who received MTX+TNFi directly after the failure of MTX.
Conclusions Effectiveness was better for MTX+TNFi than for MTX+sDMARDs. Patients who started MTX+TNFi after two synthetic DMARD regimens had failed had a tendency to less favourable disease states after 3 months than patients who switched directly from MTX to MTX+TNFi.
Statistics from Altmetric.com
Introduction
Methotrexate (MTX) is currently the cornerstone in the treatment of rheumatoid arthritis (RA) and recommended as first-line therapy.1 2 Both the treatment recommendations from the European League Against Rheumatism (EULAR) and recently published recommendations for the use of MTX in rheumatic diseases advocate MTX monotherapy as the first choice rather than combinations of MTX with other synthetic disease-modifying antirheumatic drugs (sDMARDs),1 3 whereas the American College of Rheumatology recommends MTX or other DMARDs as monotherapy or MTX in combination with other DMARDs, depending on the disease duration and level of disease activity.2
The efficacy of adding a tumour necrosis factor α inhibitor (TNFi) to MTX in patients who are MTX inadequate responders (IR) is well established,4,–,9 whereas evidence for the efficacy of adding sDMARDs in MTX IR is less robust.9,–,13 In many countries it is currently required that two or more sDMARDs must have failed before initiation of TNFi therapy.14 In Norway the general requirement is moderate to high disease activity level and inadequate response to MTX in patients with RA.
The objective of this real-life register-based study was to compare the effectiveness of adding sDMARDs versus adding a TNFi to MTX in patients with RA who were MTX IR. A second objective was to examine the clinical outcomes in the subgroup of patients who received delayed MTX+TNFi after the sDMARD combination.
Methods
Setting
Since December 2000, adult patients (>18 years of age) with inflammatory arthropathies in five Norwegian rheumatology departments starting treatment with synthetic and/or biological DMARDs have been included in the NOR-DMARD register. The five centres together cover more than 1.4 million inhabitants, nearly one-third of the Norwegian population. The study design is a prospective multicentre longitudinal observational study with assessments at baseline, after 3, 6 and 12 months and then yearly. An overview of the register is presented in figure 1.

Overview of the NOR-DMARD register and patients included in the study. All included patients were patients for whom MTX monotherapy had failed but details on the initial MTX monotherapy were not available for all patients. AS, ankylosing spondylitis; DMARD, disease-modifying antirheumatic drug; IA, inflammatory arthritis; LEF, leflunomide; MTX, methotrexate; PsA, psoriatic arthritis; RA, rheumatoid arthritis; sDMARD, synthetic disease-modifying antirheumatic drug; SSZ, sulfasalazine; TNFi, tumour necrosis factor inhibitor.
Patients
For the current analyses we selected patients with RA who were included in the NOR-DMARD register before January 2010 for whom MTX monotherapy had failed (MTX IR) and thereafter started either MTX plus a TNFi or MTX plus one or more other sDMARDs (figure 1). The patients had to have disease duration of ≤5 years when starting combination therapy and no other DMARDs except MTX should have failed. The definition of ‘treatment failure’ was according to the treating physician and not standardised. We retrieved information about the initial MTX monotherapy treatment from data available in NOR-DMARD (baseline characteristics, MTX doses, time receiving treatment, effectiveness).
From the group of patients treated with sDMARD combinations we identified a subgroup of patients who started MTX+TNFi after the sDMARD combination had failed, and for these patients by definition two or more sDMARDs had failed including MTX (figure 1).
Assessments and outcomes
Baseline, 3- and 6-month assessments were included in the main analyses, while the drug survival analysis was based on 2-year data. Assessments included 28-swollen and tender joint counts (28-SJC and 28-TJC) performed by rheumatologists or trained research nurses, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), 0–100 mm Visual Analogue Scales for physician's assessment of global disease activity and patient's assessment of joint pain, fatigue and global disease activity (100 mm=worst score), and the modified Health Assessment Questionnaire.15 The Medical Outcomes Study 36-item Short-Form Health Survey (SF-36)16 17 was used to calculated physical and mental components summary scores (SF-36 PCS and SF-36 MCS, respectively) and SF-6D.18 The Disease Activity Score 28 (DAS28) with ESR19 and the Simplified Disease Activity Index (SDAI)20 were calculated. For each group we calculated proportions achieving a EULAR good response,21 as well as DAS28 remission (DAS28<2.6), DAS28 low disease activity (LDA) (DAS28≤3.2), SDAI remission (SDAI≤3.3) and SDAI LDA (SDAI≤11). Owing to the exploratory nature of the analyses, we did not select specific primary and secondary end points, but decided to focus on DAS28 changes and responses at 3 and 6 months, with the 3-month assessment as the primary end point. Information about date of, and reason(s) for, treatment termination was recorded for patients who discontinued treatment. Comorbidities were recorded at baseline and updated at each study visit. As a measure of burden of comorbidities we calculated the baseline Charlson Comorbidity Index (CCI).22 23
Statistical analysis
Continuous variables are presented as means (SD) if normally and medians (IQR) if non-normally distributed. Independent samples t test and Mann–Whitney U test were applied, as appropriate. Dichotomous variables are presented as frequencies and percentages and were compared by χ2 test or Fisher's exact test. For the comparison of 3- and 6-month effectiveness (mean changes, response and remission rates) between the MTX+TNFi and MTX+sDMARD groups we also applied analysis of covariance (continuous outcomes) and logistic regression analysis (dichotomous outcomes) adjusted for the propensity score quintile.24 Propensity scores were calculated by logistic regression analysis with treatment as the dependent variable and the following covariates: age, sex, centre, rheumatoid factor status and baseline 28-SJC, 28-TJC, ESR, CRP, physician global, patient global, pain and fatigue. Further details on the propensity scores are available in the online supplement (online supplementary text section 1). In the main analyses we performed no imputation for missing data, but we also analysed the data using the last observation carried forward (LOCF) approach to replace missing 6-month data with data from the 3-month assessment if available. Continuation of treatment (‘drug survival’) was examined by Kaplan–Meier analysis with log rank test for comparison of the MTX+TNFi and MTX+sDMARD groups. Additionally, we applied Cox regression analysis with adjustment for the propensity score quintile.
Further, disease states after 3 months of MTX+TNFi treatment were compared between patients who received MTX+TNFi directly after MTX had failed and patients who first received MTX+sDMARDs (‘early’ vs delayed initiation of TNFi treatment). We also compared the mean changes in disease measures of these two groups.
Statistical tests were two-sided with level of significance set at 0.05, without correction for multiple testing. Statistical analyses were performed using the Predictive Analytics Software program, version 17.0 (SPSS, Chicago, Illinois, USA).
Results
Demographics, medication and baseline characteristics
Data on 98 patients starting treatment with MTX+TNFi (etanercept n=40, infliximab n=28, adalimumab n=30) and 129 patients starting MTX+sDMARDs (sulfasalazine (SSZ) n=56, hydroxychloroquine (HCQ) n=27, SSZ and HCQ (triple therapy; SSZ and HCQ were simultaneously added to MTX) n=44, leflunomide n=2) were extracted from the register. Ninety-six per cent of patients were eligible for at least 6-months' follow-up. Patients receiving MTX+TNFi were somewhat younger (table 1). No patients with present or prior malignancy were registered in the MTX+TNFi group and five cases were registered in the MTX+sDMARD group, of whom two had been treated >5 years (17 and 26 years) before treatment start. Also, significantly more patients had thyroid disease in the latter group (11.6% vs 4.1%, p=0.04). There was no difference in the prevalence of other comorbidities, including cardiovascular disease. The CCI scores were not significantly different between the groups (table 1), and mean (SD) CCI scores were 0.22 (0.44) for MTX+TNFi versus 0.29 (0.56) for MTX+sDMARDs.
Demographics and baseline characteristics at start of combination therapy
The mean MTX doses in the MTX+TNFi/MTX+sDMARD groups were 17.0/16.5 mg at baseline, 16.2/17.0 mg at 3 months and 15.7/17.1 mg at 6 months. The proportions of patients who used prednisolone were 56%/59% at baseline, 45%/53% at 3 months and 43%/44% at 6 months. Among those patients who used prednisolone, mean doses were 7.3/7.0 mg at baseline, 6.1/6.2 mg at 3 months and 5.3/6.0 mg at 6 months.
Baseline disease activity and health related quality of life (HRQoL) measures for the MTX+TNFi and MTX+sDMARD groups are presented for all patients, as well as for patients included in the effectiveness analyses (table 1). Except for the above-mentioned difference in age, there were no statistically significant differences between the groups.
The initial MTX monotherapy
Details on the initial MTX monotherapy were available for 71 patients (72%) in the MTX+TNFi group and 97 patients (75%) in the MTX+sDMARD group. The available data did not indicate any major differences in baseline characteristics and responses to MTX monotherapy between the groups (table 2) . Further details are available in the online supplementary material (online supplementary text section 2).
Baseline at start of the initial MTX monotherapy
Effectiveness of the first combination therapy
The 3- and 6-month response and remission rates as well as changes in disease activity and HRQoL measures for MTX+TNFi and MTX+sDMARDs are shown in table 3. Responses were universally better for MTX+TNFi, and in the unadjusted analysis most differences were statistically significant. The mean (95% CI) group difference in ∆DAS28 was −0.75 (−1.15 to −0.36) at 3 months and −0.88 (−1.39 to −0.36) at 6 months in favour of MTX+TNFi. When adjusting for the propensity score quintile the statistical significance of the difference in some outcomes was lost, particularly at 6 months (table 3). Adjusting for age or the CCI did not influence the effectiveness analyses (data not shown).
Remission and response rates and changes in disease activity measures after 3 and 6 months of the first combination therapy
The results after applying the LOCF approach to replace missing 6-month data were similar to the results of the completer data analyses (online supplementary table S1). The responses were as expected of a somewhat smaller magnitude than with the completer data, but the difference between completer data and LOCF data were more pronounced for the MTX+sDMARD group, accentuating the statistical difference versus MTX+TNFi.
The MTX+sDMARD group consisted of four different MTX+DMARD combination therapies, and we performed exploratory analyses to examine potential differences between these treatments (table 4). Patients receiving MTX+SSZ+HCQ (triple therapy) had higher baseline disease activity than patients receiving other MTX+sDMARD combinations (mean DAS28 5.32 vs 4.77, p=0.02). Somewhat larger improvements in disease activity were observed for patients receiving triple therapy than for the other patients in the group, but triple therapy was generally inferior to MTX+TNFi (table 4).
Three- and 6-month effectiveness of triple therapy vs other MTX+synthetic DMARD combinations and MTX+TNFi
Retention to therapy
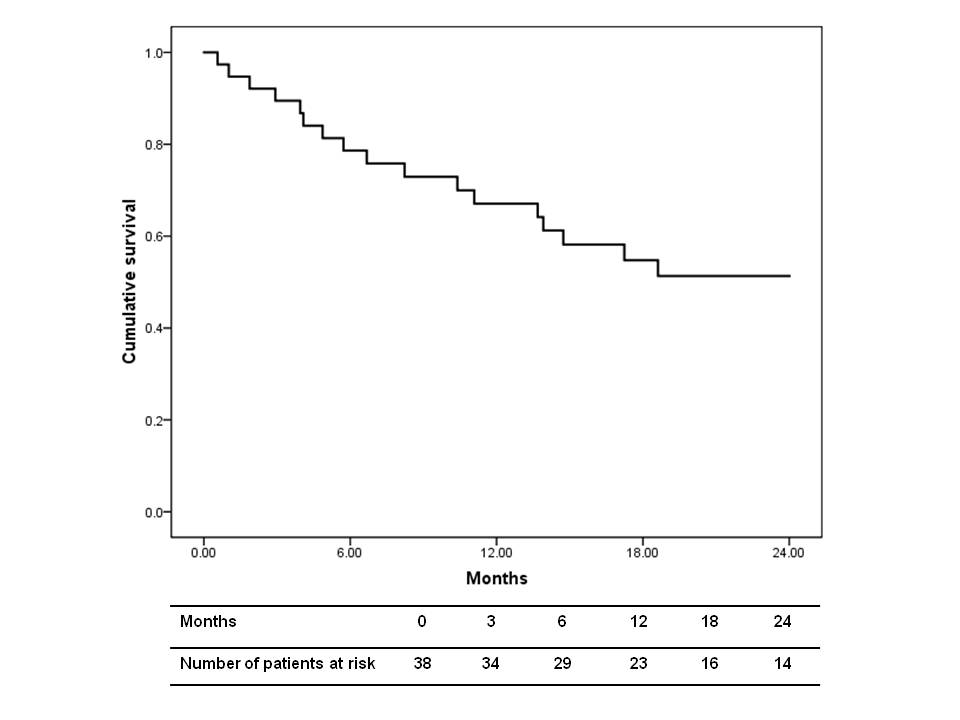
Retention to therapy was better for MTX+TNFi versus MTX+sDMARDs with estimated drug survival rates of 75% and 51%, respectively, at 1 year, and 66% and 38% at 2 years (p<0.001 for both comparisons; figure 2). The HR (95% CI) for discontinuation over 2 years was 0.42 (0.27 to 0.65) for MTX+TNFi versus MTX+sDMARDs, and the difference remained highly significant when adjusting for the propensity score quintile (HR=0.43 (0.26 to 0.70), p=0.001). Further details about reasons for discontinuation of treatment are outlined in online supplementary text section 3.

{kind=link}
{kind=link}
Kaplan–Meier plots over 2-year retention to therapy. The table shows the numbers of patients at risk at different time points during follow-up. Log rank test for 2-year drug survival: p<0.001. MTX, methotrexate; sDMARD, synthetic disease-modifying antirheumatic drug; TNFi, tumour necrosis factor inhibitor.
Delayed MTX+TNFi therapy
A subgroup of 38 patients subsequently switched to MTX+TNFi (etanercept n=13, infliximab n=16, adalimumab n=9) after MTX+sDMARDs had failed (figure 1). Median (IQR) disease duration was 1.08 (0.51–1.70) years when starting the first combination with MTX+sDMARDs and 2.08 (1.22–3.88) years when starting MTX+TNFi. Baseline values at the start of MTX monotherapy, MTX+sDMARDs and MTX+TNFi are shown in online supplementary table S2, and further details are available in the online supplementary text section 4.
The disease activity states and LDA and remission rates after 3 months of MTX+TNFi treatment are shown in online supplementary table S3. The statistical comparison of the delayed MTX+TNFi group with patients who received MTX+TNFi earlier was limited by the relatively small number of patients in the former group (31 of 38 patients had available 3-month data), but most differences were in favour of the ‘early’ MTX+TNFi group. In the ‘delayed’ MTX+TNFi group only 15.4%/7.4% achieved DAS28/SDAI remission at 3 months (online supplementary table S3), and changes in outcome measures from the start of MTX+sDMARDs to 3 months after start of MTX+TNFi were also numerically inferior to the 3-month changes observed in the ‘early’ MTX+TNFi group (online supplementary table S3).
Discussion
In this longitudinal observational study we compared the effectiveness of step-up therapy with TNFi versus sDMARDs in MTX IR, and found significantly better responses for the MTX+TNFi combination for most disease outcomes at both 3 and 6 months (table 3), as well as improved drug survival (figure 2). For the second objective regarding potential loss of clinical benefit in the patients who went on to receive MTX+TNFi treatment after the MTX+sDMARD combination had also failed, the results were less conclusive, partly owing to a reduced number of patients, limiting the statistical power. However, few of the patients in this group achieved clinical remission (online supplementary table S3) and drug survival was inferior compared with patients receiving MTX+TNFi directly after MTX monotherapy had failed (online supplementary figure S1).
The inferior clinical responses and higher discontinuation rates with the MTX+sDMARD combinations in this study are in concordance with results from the SWEFOT trial where patients with inadequate response (DAS28>3.2) after 3–4 months of MTX monotherapy were randomised to either MTX+infliximab or triple therapy.9 In contrast, the Treatment of Early Aggressive RA study showed similar mean DAS28 values over 2 years in patients receiving step-up therapy (step-up from MTX at 6 months if DAS28>3.2) with either triple therapy or MTX+etanercept.25 Few randomised placebo-controlled trials have examined the efficacy of step-up therapy with sDMARDs in MTX IR, but there is some evidence that step-up therapy with ciclosporin A,26 intramuscular gold27 and leflunomide28 is beneficial. These combination therapies were, with the exception of two patients receiving MTX+leflunomide, not used in our clinical setting. In a randomised double-blind, placebo-controlled trial O'Dell et al29 found better efficacy of triple therapy versus duo therapies with either MTX+SSZ or MTX+HCQ but this study included MTX naïve patients as well as MTX IR. Previously, a smaller randomised double-blind, placebo-controlled trial, also including a mixed group of DMARD IR, had shown better efficacy of triple therapy versus MTX monotherapy and SSZ+HCQ.30 Exploratory analyses of patients receiving MTX+sDMARD treatment in the current study also suggested a somewhat better effectiveness with triple therapy than with MTX+HCQ and MTX+SSZ, but groups were rather small and the responses were still inferior to those observed with MTX+TNFi treatment (table 4).
In the step-up combination arm of the BeSt study, the patients who did not reach the treatment goal of DAS<2.4 with MTX monotherapy received MTX+SSZ as a second step, and subsequently HCQ was added if the treatment goal was still not reached.31 In the BeSt study the strategies of step-up combination therapy or sequential monotherapy gave similar results but were both inferior for radiographic progression, and to some degree also, clinical responses, than initial combination therapy either with MTX+SSZ+high-dose prednisone or with MTX+infliximab after 1, 2 and 4 years of treatment.31,–,33 A publication with more detailed analysis of the two initial MTX monotherapy arms in BeSt concluded that subsequent treatment with sDMARDs was not likely to result in sustained LDA in MTX IR.11
Some limitations of our study warrant further discussion. This study was observational and not randomised and the choice of treatment strategy is likely to have been influenced by patient characteristics and other factors. However, except for slightly lower age, there were no statistically significant differences between patients for whom a TNFi was added versus patients for whom sDMARDs were added (table 1). It might be argued that patients with more severe disease were more likely to be prescribed MTX+TNFi therapy while patients with more favourable prognostic factors would be more likely to be prescribed MTX+sDMARDs—that is, confounding by indication. The addition of sDMARDs was a more common strategy in the early 2000s, and we also found a clear centre effect with the proportion of patients prescribed MTX+sDMARDs after failure of MTX monotherapy being higher in two of the five centres. To account for indication bias we used propensity score stratification/adjustment,24 and this adjustment reduced the statistical difference between treatment groups (table 3 and online supplementary table S1). The propensity score approach will only offer balancing of observed covariates and cannot replace randomisation. There is also a risk of overadjustment, especially in a situation with limited power such as in our study. The statistical significance of the superiority of MTX+TNFi over MTX+sDMARDs seemed to prevail in the adjusted analyses for most outcomes (table 3, online supplementary table S1). Further, for both groups, the decision to discontinue treatment was according to the treating physician and not standardised. Retention to therapy will always be influenced by other factors than efficacy and adverse events, such as expectations of both the patient and treating physician and the availability of other treatment options. Such factors must be kept in mind when interpreting the results.
The choice of type of MTX+sDMARD combination seemed to be influenced by local practice at the respective centres. For the choice of TNFi agent in the ‘early’ and ‘delayed’ MTX+TNFi groups there was no observed centre effect. Data from randomised placebo-controlled trials have indicated that adalimumab, etanercept and infliximab have similar efficacy in RA,4,–,6 but results from the Danish DANBIO register have suggested that the effectiveness of infliximab is somewhat lower than for the other two drugs.34 The distribution of various TNFi agents was not entirely equal in the ‘early’ and ‘delayed’ groups in this study, with infliximab constituting a higher proportion in the latter, and this difference might have influenced the observed effectiveness in favour of earlier MTX+TNFi treatment.
Among the patients who went on to receive MTX+TNFi after the MTX+sDMARD combination had failed, the majority of patients had discontinued the first combination due to lack of efficacy. These patients were thus a selected group of non-responders who might be less likely to respond to MTX+TNFi than the patients for whom MTX only had failed, and this might also partly explain the somewhat lower response rates observed in this group. The baseline characteristics of the patients in this ‘delayed’ MTX+TNFi group at the stage of initiation of the first combination therapy were, however, similar to the characteristics in patients in the ‘early’ MTX+TNFi group, and adjusting for baseline disease activity, disability or demographics did not significantly influence the results. The net loss from this delay to start MTX+TNFi treatment might be even larger in the form of increased radiographic progression during the prolonged period of non-effective treatment, and ideally radiographic data on these patients should have been available. For logistic reasons, radiographic data are not available in NOR-DMARD.
Despite the above mentioned limitations we believe that this study provides useful data from clinical practice on the effectiveness of adding sDMARDs to MTX in patients who are MTX IR, supplementing the results from recent randomised trials.9 25 31 Fewer than one in five of the patients assigned to this strategy achieved a good clinical response and clinical remission. Data on larger groups of patients, including imaging data, are needed to elucidate the potentially negative consequences of requiring failure of two versus one DMARD regimens before starting TNFi therapy.
Acknowledgments
The authors thank the patients for participating in this study, the local rheumatology staff for data collection and Inge C Olsen for helpful discussions about the statistical analyses.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
{kind=link}
Footnotes
-
Funding The work was supported by Eastern Norway Regional Health Authority. The Norwegian Disease-Modifying Antirheumatic Drug study has received unrestricted grant support from Abbott, Amgen, Wyeth, Aventis, MSD, Schering-Plough/Centocor, BristolMyers Squibb, UCB, Roche and the Norwegian Directorate for Health and Social Affairs.
-
Competing interests The NOR-DMARD register is financially supported by pharmaceutical companies but the sponsors are not involved in the analyses and presentation of data. Most of the authors have received speaker and/or consultancy honoraria from companies marketing biological DMARDs.
-
Ethics approval This study was conducted with the approval of the regional ethics committee and by the Data Inspectorate. Patients gave written informed consent before participation.
-
Provenance and peer review Not commissioned; externally peer reviewed.