Article Text

Abstract
Objective To investigate the effect of tumour necrosis factor (TNF) antagonist treatment of patients with rheumatoid arthritis (RA) on sick leave (SL) and disability pension (DP) in a population-based setting in southern Sweden.
Methods All patients with RA in the South Swedish Arthritis Treatment Group register living in the county of Skåne (population 1.2 million), who started their first treatment with a TNF antagonist between January 2004 and December 2007 and were 18–58 years at treatment start (n=365), were identified. For each patient with RA, four matched reference subjects from the general population were randomly selected. Data were linked to the Swedish Social Insurance Agency register and the point prevalence of SL and DP as well as days of SL and DP per month were calculated from 360 days before until 360 days after treatment start.
Results At treatment start 38.6% of the patients with RA were registered for SL. During the first 6 months this share dropped to 28.5% (decrease by 26.2%, p<0.001). This level remained stable throughout the first treatment year. Comparing patients with RA to the reference group the relative risk of being on SL was 6.6 (95% CI 5.2 to 8.5) at initiation of anti-TNF treatment and 5.2 (95% CI 4.0 to 6.8) 1 year after that. The corresponding figures for DP were 3.4 (95% CI 2.7 to 4.2) and 3.2 (95% CI 2.7 to 3.9).
Conclusions There was a marked decline in SL during the first 6 months of TNF antagonist treatment in patients with RA in southern Sweden, maintained throughout the first year, which was not offset by a corresponding increase in DP.
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) most often results in a substantial deterioration of physical function, leading to work disability and employment loss.1,–,4 The corresponding decrease in productivity constitutes a considerable limitation for the patient as well as an economic burden to society.5,–,7
RA management of today focuses on early aggressive pharmacological treatment.8 The introduction of tumour necrosis factor (TNF) antagonists has played a major role with better control of symptoms, halting of radiological progression and improvement of functional capacity and health related quality of life.9,–,14 Reports on the effect of anti-TNF treatment on work disability have, however, been conflicting depending on the setting and study design.15,–,21
Studies investigating the impact of anti-TNF treatment on work outcomes have been based mainly upon self-reported measures. However, well validated register data could potentially provide more relevant information.
The objective of this study was therefore to investigate the effect of TNF antagonist treatment of patients with RA on real life data on sick leave (SL) and disability pension (DP), in a population-based setting in southern Sweden, as compared to a matched reference group from the general population.
Methods
Data on SL and DP
All residents in Sweden aged 16–64 years can be granted economic security from the Swedish Social Insurance Agency (SSIA) in the case of work incapacity due to sickness, disability or injuries. For the first day of sickness, the qualifying day, no benefit is paid. From the 2nd to the 14th day sick pay is obtained directly from the employer.
From day 15 of sickness, economic compensation is provided by the SSIA in the form of sickness benefit. It is generally limited to 1 year and is payable as full, three-quarters, half or one-quarter benefit, depending on the reduction in work capacity. For individuals who have a permanent or long-term incapacity for work, DP can be obtained. This benefit can be granted for either a limited or an indefinite period and is payable as full, three-quarters, half or one-quarter benefit, owing to the extent of the reduction in work capacity.
In this study SL was defined as days with sick pay or sickness benefit of any degree registered by the SSIA. The first 2 weeks of sickness were included only if the disease period lasted for more than 14 days (otherwise the days were not registered by the SSIA and could not be counted). Analogously, DP was used for days with DP with any degree of compensation registered by the SSIA. In contrast, net days of SL or DP encompass the degree of compensation (full, three-quarters, half or one-quarter) including a transformation of part compensation days into full compensation days. Net days furthermore only include days when the benefit has been provided by the SSIA (as for SL, excluding all disease episodes shorter than 15 days). Cases of SL and DP of any cause were included in the study.
All data on SL and DP were taken from the SSIA register covering 100% of those receiving reimbursement from the SSIA. This register is available through the MORSE project.22
Patients
Subjects eligible for this study were patients in the South Swedish Arthritis Treatment Group (SSATG) register, having a diagnosis of RA according to the treating doctor. The SSATG is a clinical protocol for monitoring the performance of biological treatment of patients with rheumatological diseases involving 11 rheumatology units in southern Sweden. It was set up in 1999 and today constitutes a large, prospective, population representative cohort comprising approximately 4300 patients of which almost 2700 are patients with RA (November 2009).23,–,25 In a previous validation study 98% of the patients with RA in this register fulfilled the American College of Rheumatology RA classification criteria,24 26 and the coverage was calculated to be between 90% and 95% of all TNF blocking drugs used for rheumatic diseases in the county of Skåne (population 1.2 million).25 The SSATG register only encompasses patients treated with biological drugs.
We identified all patients with RA in the SSATG register living in the county of Skåne, who started their first treatment with a TNF antagonist between January 2004 and December 2007 (the recruitment period) and were aged 18–58 years at treatment start. All data from the three TNF blockers used (adalimumab, etanercept or infliximab) were merged. The upper age limit in the RA cohort was chosen to exclude old-age pensioners and individuals whose benefit might be converted to old-age pension during the study period. The recruitment period was selected to reflect a period when the usage of TNF inhibitors had reached a level similar to that seen in more recent years. According to the Swedish treatment guidelines there are suggestions, but no specific level of a disease activity measure is required for start of anti-TNF treatment.27
Data were then linked to the SSIA register, being sequentially anonymised. The proportion of patients with ongoing SL (the point prevalence) was computed for 1 day every 30th day from 360 days before until 360 days after treatment start (the study period), the same procedure being carried out for DP. In addition we calculated net days per month of SL and DP, respectively, during the study period. Calculations were performed for the whole cohort and for men and women separately. All calculations were carried out using an intention to treat approach.
For each patient with RA, four subjects from the general population matched for sex, age, area of residence and time were drawn from the Swedish Population Register, forming a reference group. The population register is the civil registration of vital events (eg, births, deaths, marriages) of the inhabitants of Sweden administered by the Swedish tax agency. Data were again linked to the SSIA register, being sequentially anonymised. The point prevalence of SL and DP were computed in the same way as for the patients with RA.
Statistics
For differences in baseline characteristics between men and women independent samples t tests, or Mann–Whitney U tests where appropriate, were used for analysis. Changes in SL and DP point prevalence were assessed by McNemar's test, whereas changes in SL and DP net days per month as well as changes in 28-joint Disease Activity Score (DAS28) and Health Assessment Questionnaire (HAQ) were analysed by paired samples t test. Differences between men and women in SL and DP point prevalence were assessed by χ2 test, while differences regarding SL and DP net days per month were analysed by independent samples t test. Work disability outcomes are subjected to secular trends caused by overall changes in society such as new political policies. In order to adjust for such trends, relative risks for being on SL were calculated by dividing the point prevalence of patients with RA with that of the reference group. The 95% CIs for point prevalences, net days and relative risks were computed using methods described by Altman.28 Statistical analyses were conducted using SPSS V.17.0 (SPSS, Chicago, Illinois, USA). All tests were two-tailed and p values <0.05 were considered significant.
Results
Patient characteristics
We identified 365 patients with RA (82% women). When initiating anti-TNF treatment 70.1% of the patients were on methotrexate (MTX) (with a mean dose of 17.5 mg (SD 5.2)), 9.6% had sulfasalazin and 8.8% took antimalarial drugs. In all, 97.5% had tried at least one disease-modifying antirheumatic drug (DMARD) and 62.8% had tried at least two DMARDs when initiating anti-TNF therapy. Women had significantly higher HAQ and global visual analogue scale, but significantly less swollen joints and a lower C reactive protein than men. No other significant sex differences were found (table 1). In the matched reference group the proportion of women (82%) was identical and the mean age (46.1 years (SD 10.1)) was almost identical to the RA cohort.
Characteristics and clinical outcomes for patients with RA starting anti-TNF therapy January 2004 to December 2007 in the county of Skåne, Sweden
During the first treatment year 92 patients (25.2%) discontinued treatment (34 patients due to adverse events, 32 due to treatment failure and 26 due to other reasons). Etanercept was the most commonly used drug (57.3%) followed by adalimumab (27.9%) and infliximab (14.8%). During the first treatment year there was also a significant decrease in DAS28 (mean difference 2.0, p<0.001) and HAQ (mean difference 0.31, p<0.001) results.
Point prevalence of work disability
During the year before initiation of anti-TNF treatment the SL point prevalence increased in the RA cohort reaching 38.6% (95% CI 33.6 to 43.6) at treatment start (figure 1). Following treatment start a significant decrease (p<0.001) was seen already after 1 month, the share dropping to 28.5% (23.9 to 33.1) at 6 months. This level remained fairly stable throughout the first treatment year being 29.6% (24.9 to 34.3) at 12 months. Changes in SL point prevalence were significant (p<0.001) for the year before and the year after treatment start. In contrast, SL point prevalence for the reference group was stable during the same periods with no statistically significant changes.

Point prevalence of sick leave for patients with rheumatoid arthritis (RA) and a matched reference group from the general population with 95% CIs. Values are given for the period from 360 days before until 360 days after initiation of anti-tumour necrosis factor treatment. p Values indicate statistical comparisons 360 days before treatment start versus treatment start and treatment start versus 360 days thereafter for patients with RA and the reference group, respectively.
Regarding DP there was a continuous increase in the point prevalence for patients with RA and the reference group during the study period (figure 2). The point prevalence for patients was 31.0% (95% CI 26.2 to 35.7) 1 year before starting treatment, 34.2% (29.4 to 39.1) at treatment start and 38.4% (33.4 to 43.3) 1 year thereafter. The corresponding figures for the reference group were 9.3% (7.8 to 10.7), 10.1% (8.6 to 11.7) and 11.8% (10.2 to 13.5). Changes in DP point prevalence for patients with RA and the reference cohort were significant (p<0.001) the year before treatment start and the first treatment year. In relative numbers the changes in DP point prevalence for patients with RA and the reference group were similar, although the absolute changes were larger for the RA cohort.
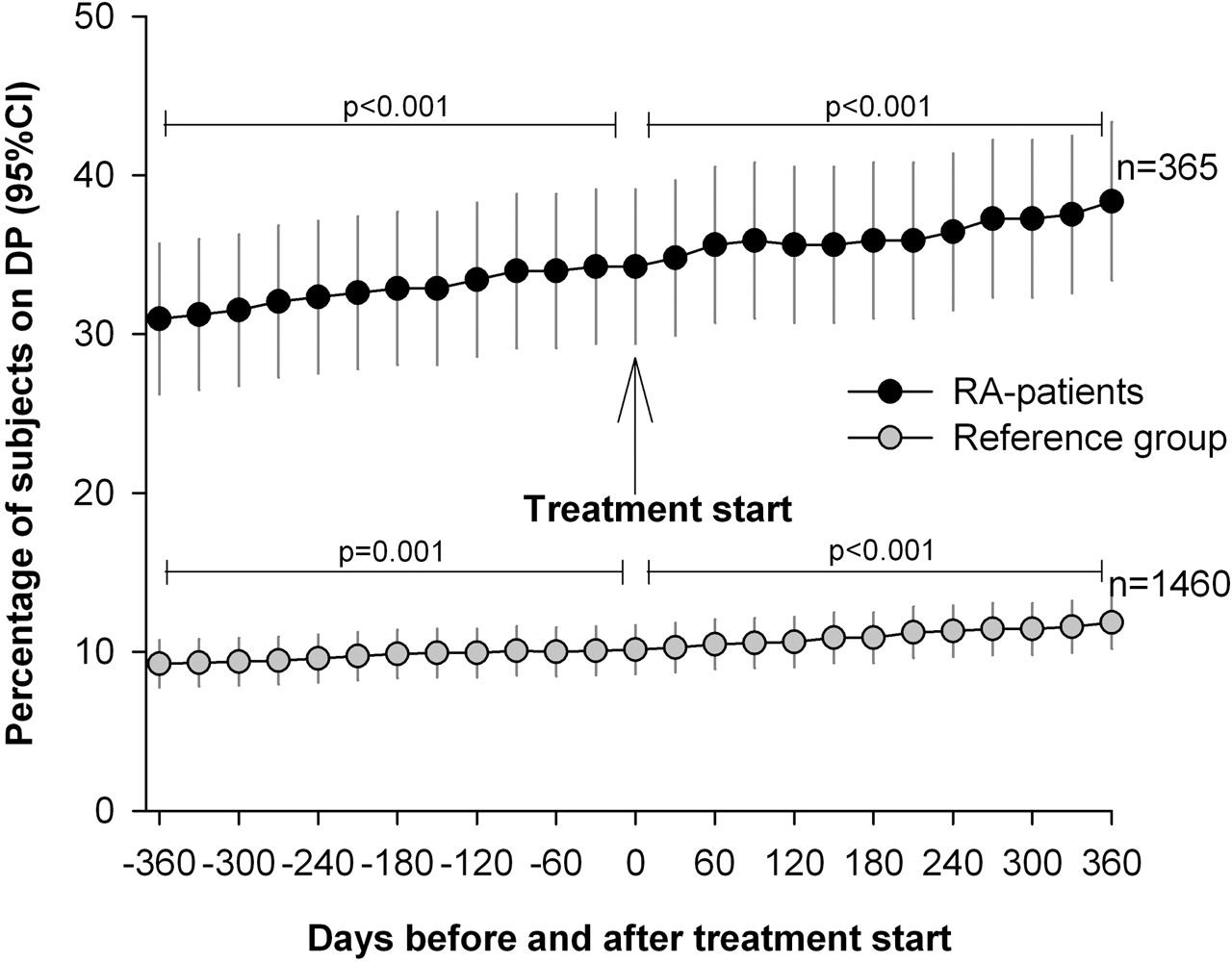
Point prevalence of disability pension for patients with rheumatoid arthritis (RA) and a matched reference group from the general population with 95% CIs. Values are given for the period from 360 days before until 360 days after initiation of anti-tumour necrosis factor treatment. p Values indicate statistical comparisons 360 days before treatment start versus treatment start and treatment start versus 360 days thereafter for patients with RA and the reference group, respectively.
Relative risks of work disability
Comparing the patients with RA to the reference group the relative risk of being on SL was 4.0 (95% CI 3.0 to 5.2) 12 months before starting TNF antagonists increasing to 6.6 (5.2 to 8.5) at treatment start. At 6 months thereafter the relative risk had fallen to 5.1 (3.9 to 6.6), being 5.2 (4.0 to 6.8) at 12 months. The relative risk of being on DP for patients with RA was stable during the study period and was 3.3 (2.7 to 4.2) 1 year before treatment start, 3.4 (2.7 to 4.2) at treatment start and 3.2 (2.7 to 3.9) 1 year after treatment start. In absolute numbers, the decrease in SL point prevalence from treatment start until day 360 for the RA cohort was 9.0% and the increase in DP point prevalence was 4.1%. Adjusting those figures by subtracting the absolute changes in SL and DP for the reference group, respectively, yielded an adjusted absolute decrease in SL of 8.9% and an adjusted absolute increase in DP of 2.4% during the first treatment year.
Net days of work disability
The mean number of SL and DP net days per month (ie, accounting for whether the days were full time or part time) for patients with RA are shown in figure 3. SL net days per month increased for patients during the year before initiation of anti-TNF treatment, reaching 9.3 days on average (95% CI 8.0 to 10.6) the first month after treatment start (p<0.001). A decrease was then seen, numbers dropping to mean 6.5 days (5.4 to 7.7) the seventh month after treatment start (a decrease by 29.7%, p<0.001). The level then stabilised, being 6.6 days on average (5.5 to 7.8) the 12th month after treatment start. Regarding DP net days per month there was a steady increase during the study period, being 6.6 days on average (5.5 to 7.8) 12 months before treatment start, 7.4 days (6.2 to 8.5) the first month after treatment start and 8.2 days (7.0 to 9.4) the 12th month after treatment start. Changes in DP net days per month during the year before and the year after initiation of treatment were significant (p<0.01). On bivariate analysis the change in SL net days from treatment start until day 360 was significantly correlated with the change in DAS28 (rs=0.16, p=0.043) during the same period, but not with the change in HAQ. For detailed information on a combined measure of SL and DP net days per month, see the supplementary material.

{kind=link}
{kind=link}
{kind=link}
Mean net days of sick leave and disability pension per month with 95% CIs for patients with rheumatoid arthritis (RA). Values are given for the period from 360 days before until 360 days after initiation of anti-tumour necrosis factor treatment.
Sex differences
Women had higher numbers of SL net days per month throughout the study period than men. The differences were statistically significant 1 year before treatment start (5.6 days vs 2.8 days, p=0.02), 1 year after treatment start (7.2 vs 4.0, p=0.01) but not at treatment start (table 2). Women also showed a trend towards overall higher SL point prevalence, but the differences were not statistically significant (table 3). Regarding DP, women had a higher point prevalence and more DP net days per month than men during the study period, but no statistically significant differences were detected.
Mean net days of SL and DP per month with 95% CI for patients with RA, stratified by sex
Point prevalence (%) of SL and DP for patients with RA and a matched reference group from the general population, stratified by sex
Discussion
The main finding in this study was a continuous increase in SL point prevalence among patients with RA the year before initiation of TNF antagonists, followed by a rapid decrease (26.2%, p<0.001) during the first 6 months of therapy. The level of SL point prevalence was then maintained throughout the first treatment year. In contrast, the point prevalence of SL for the reference group was almost unchanged during the same period. Analysing SL net days per month in patients with RA, changes of similar magnitude as those seen for SL point prevalence were detected during the study period.
Although we cannot exclude a regression to the mean effect when aggregating data, the reduction in SL during the first anti-TNF treatment year must be considered as a conservative measure in this cohort of patients who were severely ill, since there was a steady increase in SL prior to initiation of therapy. Even a stabilisation of the SL level could have been deemed as a successful outcome. Furthermore, by using an intention to treat analysis our results included subjects who discontinued treatment during the study period and should therefore be considered as a conservative measure also in this regard. It has previously been shown that a new more effective treatment can reduce SL, regardless of the type of medication.29 In the present study practically all patients had had an adequate course of conventional DMARDs when starting anti-TNF therapy, yielding the conclusion that anti-TNF agents have an effect on SL of its own in this RA cohort which has responded poorly to other drugs.
Regarding DP there was a steady increase in the point prevalence for patients with RA during the whole study period, seemingly unaffected by the initiation of TNF inhibitors. In the present time perspective this was not unexpected since obtaining DP can be regarded as a more static condition than being on SL, often mirroring irreversible work incapacity. In our data this is supported by the fact that only one patient with RA and one subject in the reference group came off DP during the first treatment year. As for the reference group, there was also a continuous increase in DP point prevalence during the study period. Since DP is strongly correlated with age in the general population this could, to a great extent, be explained by the fact that all subjects became 2 years older.30 The relative changes in DP point prevalence for patients with RA and subjects from the general population were similar, but the absolute changes were larger for the patient cohort.
Comparing patients with RA to the reference group, the relative risk of being on SL increased markedly the year before treatment start followed by a considerable reduction during the first 6 months of treatment. This level was then maintained throughout the first year. In contrast, the relative risk of being on DP was almost unchanged during the study period. Furthermore, the observed absolute decrease in SL point prevalence among patients with RA was considerably larger than the simultaneous absolute increase in DP point prevalence. This, together with the fact that initiation of anti-TNF treatment did not seem to affect the trend in DP point prevalence, indicates that the decrease in SL during the first treatment year was not offset by a corresponding increase in DP.
Women showed consistently higher numbers of SL and DP net days per month as well as a higher SL and DP point prevalence during the study period, though only differences in SL net days were statistically significant. The gender difference was expected in view of higher numbers of SL and DP among women in the general population.30 31 It was also expected due to overall higher HAQ values for women in the current study (HAQ having shown strong association with work disability).32 Longer delays in referrals to a specialist and less access to joint replacement surgery in women patients with RA may also have played a role.33,–,35
The results in this study correspond to findings in some previous studies, investigating the effect of TNF inhibitors on work outcomes. The level of reduction of work disability was similar to that seen in a recent observational Swedish study, although the outcome variable was self-assessed hours worked per week.15 Our findings are also congruent with the results of a randomised controlled trial (RCT) showing that treatment with adalimumab plus MTX resulted in significantly less employment loss than MTX plus placebo after a period of 56 months,16 as well as with the results of an open-label extension study showing that patients who were employed and receiving adalimumab were able to work 7.3 months longer than the matched control group treated with DMARDs during a 2-year follow-up period.17
In contrast our results conflict with the findings in an RCT showing no significant difference in actual employment between patients with RA who were MTX naïve receiving MTX plus infliximab and those receiving MTX plus placebo, although the patients given MTX plus infliximab had a significantly higher probability of maintaining employability.18 The present results also differ from the findings in a more recent, observational study showing no difference in employment loss between patients with RA treated with TNF antagonists and matched controls. However, the mean disease duration in that study was 12 years for anti-TNF users, compared to a little over 4.5 years in our study, and TNF inhibitors seemed to have a protective effect in the subgroup with less than 11 years disease duration.20
A major strength of the current study is the inclusion of objectively assessed data on SL and DP from an independent source as well as the truly population-based design. The introduction of a matched reference group from the general population confers adjustment for secular trends and also facilitates comparisons with other countries.
The present study has limitations. First, periods of sickness shorter than 15 days were not registered by the SSIA and hence not included. Regarding DP this should not be a problem since periods shorter than this are extremely uncommon. As for SL, it is reasonable to assume that short periods of benefits in most cases could be attributable to intercurrent infections or injuries, thus being evenly distributed throughout the study period with no differences between patients with RA and the reference group.
Second, patients were only followed for 1 year after initiation of TNF antagonists, making evaluations of long-term benefits regarding work disability hazardous. Considering results in other studies where longer follow-up periods have been used we believe that the reduction in SL is of more permanent character, possibly being even more pronounced later on.15 17
Third, patients with RA included in this study were selected and representative only for the part of the RA population in working ages eligible for treatment with biological drugs. They were employment aged due to inclusion criteria and had high disease activity, and it cannot be ruled out that there was also a bias in treating patients more actively if there was a threat of losing work ability.
In conclusion, this study demonstrates a significant reduction of almost 30% in SL (real life data) during the first 6 months after initiation of TNF antagonists in a population-based RA cohort aged 18–58 years in southern Sweden, maintained throughout the first treatment year. This decrease was not due to secular trends, nor did it seem to be offset by a corresponding increase in disability pension.
Acknowledgments
We are indebted to all colleagues and staff in the South Swedish Arthritis Treatment Group for cooperation and data supply.
References
Supplementary materials
Web Only Data ard.2009.127852
Files in this Data Supplement:
{kind=link}
Footnotes
-
Funding This study was funded by unrestricted grants from The Swedish Research Council, Region Skåne, The Swedish Social Insurance Agency, Lund University, Lund University Hospital, Österlund and Kock Foundations, The Swedish Rheumatism Association and King Gustav V 80-Year Fund.
-
Competing interests None.
-
Ethical approval This study was approved by the Institutional Review Board of Lund University, Sweden.
-
Provenance and peer review Not commissioned; externally peer reviewed.