Article Text

Abstract
Objectives To use prospectively registered data from the Danish nationwide rheumatological database (DANBIO) to describe disease activity, clinical response, treatment duration and predictors of drug survival (ie, number of days individual patients maintained treatment) and clinical response among patients with ankylosing spondylitis (AS) receiving their first treatment series with a tumour necrosis factor α (TNFα) inhibitor.
Methods 842 TNFα inhibitor naive patients with AS were identified in DANBIO. Clinical response, drug survival and predictors thereof were investigated. ‘Clinical response’ was defined as a 50% or 20 mm reduction in Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) within 6 months compared with baseline. Achievement of a BASDAI <40 mm within 6 months was used as a second response parameter.
Results 603 patients (72%) were men, disease duration 5 (1–13) years (median (IQR), age 41 (32–50) years. 445 (53%) received infliximab, 247 (29%) adalimumab and 150 (18%) etanercept. Parameters at baseline/1-year follow-up were: C-reactive protein (CRP): 14 (7–27)/5 (2–10) mg/l, BASDAI 59 (44–72)/21 (8–39) mm, Bath Ankylosing Spondylitis Functional Index (BASFI) 50 (34–67)/24 (9–45) mm, Bath Ankylosing Spondylitis Metrology Index 40 (20–50)/20 (10–40) mm. Within 6 months, 407/644 patients (63%) achieved a clinical response. Median drug survival was 4.3 years. One- and 2-year survival rates were 74% and 63%, respectively. Baseline characteristics associated with longer drug survival were male gender, CRP >14 mg/l and low visual analogue scale fatigue (Cox regression analysis). Age, TNFα inhibitor and methotrexate use were insignificant. CRP >14 mg/l, lower BASFI and younger age at baseline was associated with clinical response and achievement of a BASDAI <40 mm (logistic regression analysis).
Conclusion TNFα inhibitors provide a rapid and sustained decrease of disease activity among patients with AS in clinical practice. Factors associated with continued treatment, clinical response and achievement of a BASDAI <40 mm were identified.
Statistics from Altmetric.com
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory rheumatic disease affecting 0.1–1.4% of the population.1 Several placebo-controlled randomised trials have shown excellent efficacy of tumour necrosis factor α (TNFα) inhibitors in AS,2,–,8 and the drugs are recommended for the treatment of patients with continuously active disease.9 10
Randomised clinical trials generally include relatively homogeneous patient-populations who fulfil a strict set of inclusion criteria and are followed up for a limited time period. Many patients treated with biological agents in ‘real life’ would have been excluded from clinical trials owing to advanced age, comorbidity or polypharmacy.11 Thus, data from observational registries on postmarketing use provide a valuable supplement to the knowledge from clinical trials about drug tolerability, drug survival, drug effects and adverse effects.12,–,16
Currently, the reported real-life data for TNFα inhibitor use among patients with AS are mainly retrospective analyses of patient files or small observational studies.13 14 17,–,20 Although prospective rheumatological registries have been established in several countries and may serve as research tools,11 21,–,24 only two clinical registry reports on patients with AS have been published25 26 and neither of them assessed predictors of treatment response and drug survival.
The Danish nationwide rheumatological database (DANBIO) prospectively registers treatment and disease activity in patients with rheumatological disease treated with biological drugs. The mandatory reporting of biological treatment to the database makes coverage and completeness of data high.27 28 The registry currently includes up to 8 years of follow-up. Several papers have previously described DANBIO data in patients with rheumatoid arthritis,16 27,–,31 whereas data for patients with AS have not been published until now.
Our aims were based on DANBIO data to report drug efficacy and drug survival as well as to identify baseline predictors of drug survival in Danish patients with AS receiving their first treatment course with a TNFα inhibitor in routine care.
Patients and methods
Patients
DANBIO is a Danish nationwide rheumatological database that collects data on patients treated with biological and other disease-modifying antirheumatic drugs (DMARDs). More than 90% of the patients who are prescribed biological treatment are included in the database.27 28 By 15 November 2008, 5366 patients receiving biological treatment had been registered in DANBIO. Among these, 842 patients were diagnosed with AS and included in this study (table 1).
Patient characteristics
The DANBIO data available in patients with AS were baseline demographics including patient age, gender, disease duration, previous or current treatment with methotrexate (MTX) or other DMARD. Disease activity parameters are prospectively reported to DANBIO by an online system and include visual analogue scales (VAS) for pain, patient's global score and fatigue score. Registrations of Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI) and Bath Ankylosing Spondylitis Metrology Index (BASMI) were introduced in year 2003.31 A doctor or a trained nurse measures the BASMI score and registers the C-reactive protein (CRP) level.32 Data collection occurs two to four times annually. HLA-B27 status is not registered in the database.
Methods
Disease activity and clinical response
Disease activity was evaluated by the CRP, VAS scores, BASDAI, BASFI and BASMI at 0, 2 and 6 weeks, 6 months, 1, 2, 3, 4 and 5 years after initiation of anti-TNF treatment (table 2). Drug efficacy was primarily evaluated by ‘clinical response’ (reduction in BASDAI of at least 50% or >20 mm compared with baseline according to the ASAS guidelines (BASDAI 50%/20 mm response)).33 34 Arbitrarily, we classified patients as ‘responders’ if they achieved a clinical response (yes or no) at least at one registration during the first 6 months' treatment. As a second measure of drug efficacy, we identified the number of patients having a BASDAI score <40 mm at least once during the first 6-month treatment.
Disease activity at baseline and during follow-up
Treatment duration
Drug survival was calculated as the number of days individual patients maintained treatment. The start date was the date of the first given dose and the stop date was the date of the first missed dose. All observations were censored at 15 November 2008. Reasons for drug discontinuation were registered.
Queries were sent to treating hospitals about 139 patients who had had no follow-up since 30 June 2008 and no registrations of stopping date. Subsequently, data on treatment duration was complete in 803 of 842 patients (95%). In the 39 patients with incomplete follow-up, data were censored according to the last visit registered in DANBIO.
Ethics
The DANBIO database has been approved by the Danish Board of Health and the Danish Data Registry. The registration of data among patients treated with biological agents does not require patient consent. Publication of data does not require approval by the ethics committee.
Statistics
All statistical analyses were done by SPSS software (version 16.0, SPSS, Chicago, Illinois, USA). Demographic and descriptive data are presented as median and range. Groups were compared by non-parametric testing (unpaired data: χ2 and Mann–Whitney tests, paired: Wilcoxon signed ranks test). Kaplan–Meier plots, log rank tests and Cox regression analyses were used for drug survival analysis. We converted each of the continuous baseline variables BASDAI, BASFI, BASMI and VAS scores into quartiles in order to visualise Kaplan–Meier drug survival curves. CRP was converted into a binary variable (below/above the median value 14 mg/l). Logistic regression analysis was used for the identification of factors associated with (a) clinical response and (b) BASDAI score <40 mm within 6 months of treatment. The factors with least significance were excluded stepwise (backward selection), leaving only statistically significant factors in the model. In the Cox and logistic regression analysis, gender, type of TNFα inhibitor, baseline CRP and baseline MTX use were included as categorical variables, whereas patient age and baseline BASDAI were continuous variables. All interactions involving sex, patient age, disease duration, MTX use and drug type were tested. Each interaction pair was included in the overall statistical model and thereafter excluded in the backward selection process if the interaction was statistically insignificant. A p value <0.05 was considered statistically significant.
Results
Patient characteristics
The number of patients with AS initiating their first treatment series with TNFα inhibitors increased over the years. The majority of patients received infliximab (table 1). A total of 310 patients (37%) withdrew from TNFα inhibitor treatment. Table 1 shows reasons for drug discontinuation. Of the 238 cases with a known reason for withdrawal, lack of efficacy (115/238 patients, 48%) was the most prevalent reason, whereas 69 patients (69/238, 29%) stopped owing to adverse effects. Details of the adverse events were provided in several cases and included infections (13 patients), cardiovascular events—for example, hypertension, palpitations, angina (six patients), rashes (nine patients) or anaphylaxia (three patients) and other allergic reactions (five patients).
At baseline, 343 patients (41%) received concomitant MTX. Among infliximab users, 254/445 (57%) received MTX compared with 40/150 (27%) and 49/247 (20%) among patients receiving etanercept and adalimumab, respectively. Thus MTX use was more prevalent among patients receiving infliximab than among those receiving adalimumab or etanercept, both at baseline (χ2 test, p<0.001) and during the whole period of observation (p<0.0001).
Baseline BASMI and CRP were significantly higher in men than women, whereas women had higher thorax excursion range, BASDAI, BASFI and VAS scores (Mann–Whitney test, all p<0.05, figure 1). Age (41 vs 41 years) and disease duration (6 vs 4 years) were similar among men and women (Mann–Whitney test, p>0.05).

Baseline disease activity for men (black bars) and women (grey bars). *p<0.05. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; BASMI, Bath Ankylosing Spondylitis Metrology Index; CRP, C-reactive protein; VAS, visual analogue scale.
Therapeutic effect
All outcome parameters decreased during follow-up (follow-up vs baseline, Wilcoxon test, all p<0.05) and thorax excursion increased (follow-up vs baseline, p<0.05) (table 2). At 6 months, CRP levels in men had decreased more than in women (10 vs 3 mg/l respectively, Mann–Whitney, p<0.001), whereas the decrease in BASDAI levels was similar among men and women (27 vs 22 mm respectively, p=0.09).
At baseline, 644 of the 842 included patients (76%) had a BASDAI score registered. Among these, 407 patients (63%) achieved a clinical response (BASDAI 50%/20 mm response) at least once during the first 6 months and 456 (71%) achieved a clinical response at least once during the whole treatment course. In 338 patients (52%), the majority (>50%) of registered BASDAI scores during the observation period were compatible with clinical response.
Overall, 794 patients (94%) had at least one BASDAI registration at baseline or during follow-up. Among these, 528 patients (66%) had at least one BASDAI score <40 mm during the first 6 months' treatment and 554 patients (70%) had at least one BASDAI score <40 mm during the whole treatment course. In 445 patients (56%), the majority of registered BASDAI scores during the observation period were <40 mm.
Drug survival
The patients were treated for a total of 1513 patient-years. Median drug survival was 4.3 years. Unadjusted 1- and 2-year retention rates were 74% and 63%, respectively.
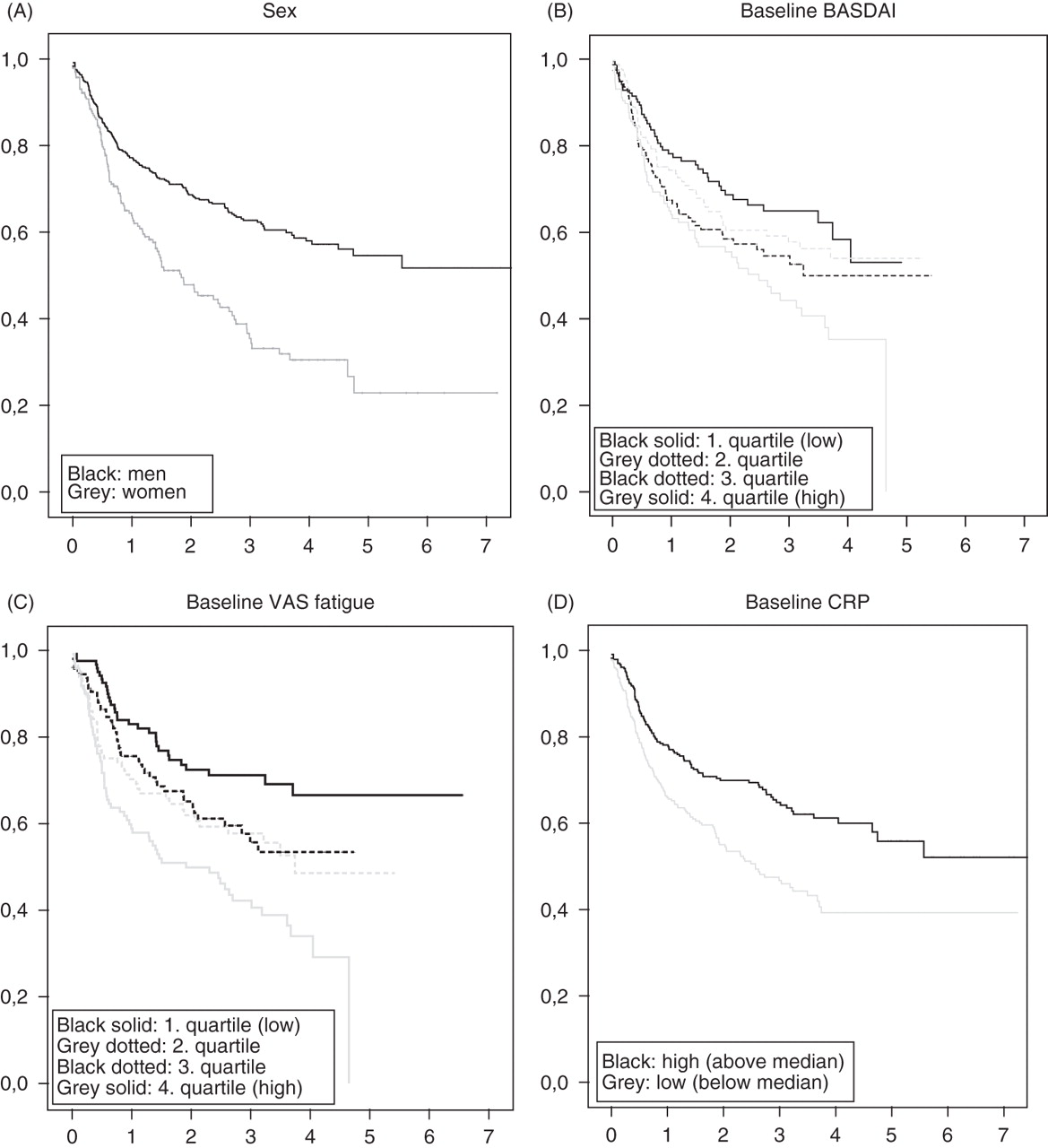
The crude retention rates were similar among patients receiving infliximab, adalimumab and etanercept (p=0.2). As shown in figure 2, male gender (panel A, log rank test p<0.0001), low baseline BASDAI (panel B, p<0.007), low VAS fatigue (panel C, p<0.0001) and CRP >14 mg/l (panel D, p<0.0001) were all associated with improved drug survival. Similar results were found for low BASFI (p=0.003), whereas baseline VAS pain (p=0.09), VAS global (p=0.08) and BASMI (p=0.9) did not affect drug survival.

{kind=link}
{kind=link}
Crude survival curves of tumour necrosis factor α inhibitor drug use according to (A) sex; (B) baseline BASDAI; (C) baseline VAS fatigue; (D) baseline CRP. x-Axis, treatment duration (years); y-axis, cumulated survival rate. BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; CRP, C-reactive protein; VAS, visual analogue scale.
Baseline disease parameters and patient characteristics were included in a Cox regression analysis in order to identify baseline factors associated with drug survival. Baseline VAS pain and VAS fatigue were strongly intercorrelated (Spearman's r>0.84, p<0.0001) and so was baseline BASDAI and VAS pain/VAS global (both r>0.72, p<0.0001). Thus, VAS pain and VAS global were excluded from the regression analysis. In the final model, male gender, low baseline VAS fatigue and high CRP were associated with better drug survival, whereas patient age, type of biological drug, baseline MTX use, BASDAI, BASFI and VAS fatigue were not associated (table 3).
Baseline predictors of discontinuing treatment with tumour necrosis factor α inhibitors
In a stratified multiple Cox regression analysis including only side effects as the event causing drug termination, sex was the only significant statistical predictor (female gender p<0.001, HR=3.37, 95% CI 2.10 to 5.41). Similarly, including only lack of treatment effect as the event causing drug termination, CRP ≤14 mg/l (p=0.006, HR=1.98 (1.22 to 3.2) and higher baseline VAS fatigue (p<0.001, HR=1.25/cm (1.11 to 1.39)) were statistically significant factors.
Prediction of clinical response and achievement of BASDAI <40 mm
In a logistic regression analysis (backward stepwise selection) with clinical response (BASDAI 50%/20 mm response) as the dependent variable, CRP >14 mg/l (OR=0.45 (low vs high) (95% CI 0.31 to 0.64) p<0.001), lower baseline BASFI (OR=0.87/cm increase (0.78 to 0.97) p=0.008) and younger age (OR=0.98/year increase (0.97 to 0.99/year) p=0.03) were associated with clinical response, whereas biological drug, gender, disease duration, BASFI, BASMI, VAS scores and baseline MTX use were without statistical significance (all p>0.05). The analysis was adjusted for the baseline BASDAI level.
In a similar logistic regression analysis (backward selection) with achievement of BASDAI <40 mm at least once during 6 months' treatment as the dependent variable, CRP >14 mg/l (OR=0.39, 95% CI 0.26 to 0.60, p<0.001), lower baseline BASFI (OR=0.86, 0.77 to 0.99, p=0.02) and younger age (OR=0.98/year, 0.97to 1.00/year, p=0.048) were predictive of the patient achieving BASDAI <40 mm. Biological drug, gender, disease duration, BASFI, BASMI, VAS scores and MTX use were without significance (all p>0.05).
We tested for interactions between baseline BASDAI, age, disease duration, biological drug, MTX use and gender, and no statistically significant interactions were found.
Discussion
This report from a nationwide prospective registry of 842 patients with AS receiving their first treatment series with a TNFα inhibitor documents the efficacy of anti-TNFα treatment in clinical practice. The measures of disease activity showed a rapid and sustained decrease and almost two-thirds of patients achieved a clinical response within 6 months. Male gender, low baseline VAS fatigue and baseline CRP >14 mg/l were associated with longer treatment continuation, whereas younger age, lower BASFI and higher baseline CRP levels predicted good treatment response.
Our cohort of patients followed for up to 8 years represents the largest cohort of TNFα inhibitor treated patients with AS with the longest observation time reported till now. Only few have previously published prospective real-life data in patients with AS. Carmona and Gómez-Reino found a 1-year TNFα inhibitor survival rate of 88% among 657 Spanish patients with AS,26 whereas a Norwegian study among 249 patients with AS reported a survival rate of 77.5%18 —a number very similar to the 74% found in our study. A Finnish group did not report survival rates but stated that 49/229 patients (21%) discontinued treatment within up to a 2-year follow-up.25 Thus, real-life retention rates of TNFα inhibitors among patients with AS seem uniformly high despite the fact that treatment strategy, attitudes and actions must be expected to vary considerably between countries.35 Observational data are difficult to compare with the tightly controlled setting of a randomised trial. However, in a randomised clinical trial, Braun et al reported that 54/69 (78%) patients with AS completed their first year of infliximab treatment4 and similarly, Davis et al found that 95/128 (74%) patients with AS completed 96 weeks of etanercept treatment.3 Thus survival rates seem similar across observational and randomised studies.
The treatment response with TNFα inhibitors was rapid and sustained. Among the patients with a BASDAI measurement at baseline, we found that 63% achieved good clinical response within 6 months' treatment. Until recently, only the total BASDAI score was registered in DANBIO and therefore a calculation of Assessment of SpondyloArthritis International Society response criteria ASAS20 or ASAS40,36 which includes relative or absolute changes in BASDAI question five and six, was not possible. This makes comparison to studies using ASAS response criteria difficult. Two other studies reporting real-life data found a similar response rate when using the BASDAI 50%/20 mm response parameter—namely, 71% among patients with AS treated with TNFα inhibitors12 or 60% within 3-month treatment with etanercept.25 In a recent open-label study among 1250 patients with AS treated with adalimumab, 57% achieved >50% reduction in BASDAI score within 3 months.37 In randomised controlled studies, 45–58% of patients achieve a 50% reduction in BASDAI.5,–,8 Individually tailored treatment, dose adjustments or concomitant use of DMARDs may, at least in part, explain why TNFα inhibitor treatment might perform better in clinical practice than in randomised trials.25
A high disease activity at baseline illustrated by a higher VAS fatigue was associated with shorter treatment duration. Others have previously reported a similar effect for a high baseline BASDAI.18 It is well known from previous studies that disease activity at baseline influences treatment outcome and drug survival, although results are not uniform.17 24 38,–,40 It has been speculated that high subjective disease activity scores might relate to late disease dominated by irreversible changes and thus a poorer treatment outcome. However, in this study we did not find any effect of disease duration on treatment outcome. Furthermore, patients with high baseline activity might have substantial relative improvements without necessarily achieving clinical remission.24 37
On the other hand, increased CRP levels at baseline were associated with longer treatment duration, good clinical response and achievement of a BASDAI <40 mm within 6 months. Similar results have previously been reported.37 39 CRP is a biomarker of inflammation and increased levels might identify patients with more active disease who are more likely to benefit from TNFα inhibitor treatment than patients with chronic, less inflammatory active disease.17 38 39
Concomitant MTX is not recommended during biological treatment of AS.10 However, 41% of our patients received MTX at baseline, and it was most prevalent among patients treated with infliximab. This is in agreement with previous studies reporting frequent use of MTX, especially among patients with peripheral joint disease or treated with infliximab.12 18 25 The influence of MTX on drug survival varies between studies. In our study, concomitant MTX use did not affect drug survival or treatment effects. A Norwegian study found similar results,18 whereas a French study reported poorer drug survival among MTX users.19 The non-randomised design makes interpretation difficult. Confounding by indication cannot be ruled out and MTX use may be a marker of more serious disease or in other ways reflect the patient's status—for example, peripheral joint involvement.35
Overall, the treatment with TNFα inhibitors was well tolerated and only a few patients stopped owing to adverse events. Our finding that drug termination occurred more frequently owing to lack of efficacy rather than adverse effects has also been reported by others,19 25 although results are conflicting.18 26
We found a significant difference in baseline disease activity between women and men. Furthermore, men responded better to treatment evaluated by the achievement of clinical response and reductions in CRP and BASDAI levels. One may hypothesise that women scored higher in the subjective parameters BASDAI, BASFI and VAS because of weaker musculoskeletal performance or a general tendency towards reporting poorer scores in questionnaires.18 40,–,42 Shorter treatment survival and poorer treatment outcome has been reported among female patients with AS18 26 or rheumatoid arthritis.18 24 40 Why women apparently respond differently to TNFα inhibitors is unclear, and any interactions between rheumatic disease, gender, sex hormones and TNFα inhibitors remain to be further investigated.40 43
We render the quality of data high. According to previous reports, >90% of Danish patients treated with biological agents are registered in the database,28 probably owing to the mandatory registration irrespective of a patient's consent. Thus, the coverage is much lower in databases using voluntary registration and requiring patient consent.26
In conclusion, this analysis of 842 patients with AS in a nationwide prospective database registry documents that TNFα inhibitors provide a rapid and sustained decrease in disease activity. The majority of patients achieved a good clinical response. Baseline CRP >14 mg/l and low VAS fatigue was associated with longer treatment continuation, whereas high CRP, low BASFI and younger age predicted good treatment response and achievement of BASDAI <40 mm. Men maintained treatment longer than women. Other parameters, including drug type and MTX use, did not significantly affect drug survival or treatment efficacy. The treatment was well tolerated and only a few patients stopped treatment owing to adverse effects.
References
Footnotes
-
Competing interests MLH has received consulting fees, speaking fees and/or research grants from Abbott, Centocor, Roche, Schering-Plough, UCB-Nordic and Wyeth (less than US$10 000 each), and on behalf of DANBIO, she has received grants from Abbott, Bristol-Meyers Squibb, Roche, Schering-Plough, UCB-Nordic and Wyeth (more than US$10 000 each). MO has received consulting fees, speaking fees and/or research grants from Abbott, Amgen, Bristol-Meyers Squibb, Centocor, Genmab, GlaxoSmithKline, Novo, Pfizer, Roche, Schering-Plough, UCB-Nordic and Wyeth (less than US$10 000 each).
-
Provenance and peer review Not commissioned; externally peer reviewed.