Article Text

Abstract
Objectives To examine the rates of acute myocardial infarction (AMI) and ischaemic stroke (IS) and to examine the predictive value of total cholesterol (TC) and triglycerides (TG) for AMI and IS in patients with rheumatoid arthritis (RA) and people without RA.
Methods In the Apolipoprotein MOrtality RISk (AMORIS) Study 480 406 people (including 1779 with RA, of whom 214 had an AMI and 165 an IS) were followed for 11.8 (range 7–17) years. Cox regression analysis was used to calculate HR per SD increase in TC or TG with 95% CI. All values were adjusted for age, diabetes and hypertension.
Results The levels of TC and TG were significantly lower in patients with RA than in people without RA. Despite this, the rate of AMI and IS per 1000 years was at least 1.6 times higher in RA than non-RA. TC was nearly significantly predictive for AMI (HR/SD 1.13 (95% CI 0.99 to 1.29), p=0.07) and significantly predictive for future IS in RA (HR/SD 1.20 (95% CI 1.03 to 1.40), p=0.02). TG had no relationship to development of AMI (1.07, 0.94 to 1.21, p=0.29), but was weakly related to IS (1.13, 0.99 to 1.27, p=0.06). In contrast, both TC and TG were significant predictors of AMI and IS in people without RA.
Conclusions Patients with RA had 1.6 times higher rate of AMI and IS than people without RA. TC and TG were significant predictors of AMI and IS in people without RA, whereas the predictive value in RA was not consistent.
Statistics from Altmetric.com
Introduction
Patients with rheumatoid arthritis (RA) have a significantly higher risk of cardiovascular disease (CVD) than the general population, which is similar to that for patients with type II diabetes.1,–,6 The focus on the increased CVD risk in RA has been on heart disease,1 since RA patients are reported to have a two to three times increased risk of acute myocardial infarction (AMI) compared with the general population.1 3 7 However, the risk of stroke is also increased, in particular ischaemic stroke (IS).1 3 7 8
Approximately half of all deaths in people with RA are due to CVD.9 10 Previous reports have also shown an increased risk of classic risk factors.11 The influence of a genetic component exists that may interact with classic cardiovascular (CV) risk factors and chronic inflammation leading to a proatherogenic status in these patients.12 This increased rate of CVD is not explained by the traditional CV risk factors such as smoking, diabetes, hypertension and body mass index.3 7 13 Furthermore, there is an increase in lipid plaques in the carotid artery in RA.14 IS may therefore be another consequence of the accelerated atherosclerosis observed in RA. Total cholesterol (TC) is a well-known risk factor for future AMI in the general population, whereas reports have been inconsistent for IS.15,–,18
The relation of lipids to CVD in RA is not well described, despite the high risk of CVD in patients with RA and the fact that lipids are major factors in CV risk stratification. We had three main objectives in this study, which focused on potential differences between RA patients and people without RA who participated in the longitudinal Apolipoprotein MOrtality RISk (AMORIS) Study: firstly, to describe the levels of TC and triglycerides (TG); secondly, to determine the rate of AMI and IS; thirdly, to investigate the relation of TC and TG to future AMI and IS in both patients with RA and people without RA.
Materials and methods
The AMORIS population and patients with RA
The AMORIS Study population has been described previously.15 19 In short, the study included healthy subjects who went for a health check in outpatient clinics, mainly in the greater Stockholm area. The inclusion period was 1985–1996. Permission for this AMORIS Study follow-up was given by the ethics review board of the Karolinska Institute and the Swedish Data Inspection, which included linkage of the total AMORIS Study database to the Swedish national hospitalisation register. This register covers all discharges with International Classification of Diseases (ICD)-coded diagnoses from all Swedish hospitals regionally since 1964 and nationally since 1987 (figure 1). The individual personal number was used for the linkage. This linkage gave the opportunity to identify patients with an RA diagnosis according to the following ICD codes: ICD-8 (712.0) for 1969–1986, ICD-9 (714.0, 714.8, 714A, 714W) for 1986–1997 and ICD-10 (M05.*, M06.0) for 1997–2002. Follow-up lasted to and included 2002—that is, the average follow-up time was 11.8 (range 7–17) years.

AMORIS population flow chart for cardiovascular end points, blood sampling and extraction of patients with rheumatoid arthritis (RA), hypertension and diabetes and exclusion of patients with acute myocardial infarction (AMI) and ischaemic stroke (IS).
The linkage enabled exclusion of registered cases with non-fatal AMI as the primary or secondary diagnosis and also stroke events before entering the AMORIS Study and before AMORIS blood sampling. The validity of hospital discharge and mortality data in Sweden with regard to the AMI and IS diagnosis has been evaluated repeatedly and found to be high for epidemiological purposes.20,–,22
Outcomes
Linkage to registers also provided opportunities to identify relevant outcomes. From the Swedish national hospital discharge register and the Swedish national cause-of-death register, all hospital discharges and deaths with AMI (ICD-8 or ICD-9 with code 410 and ICD-10 code I21) and IS (see definitions below) as the diagnosis during follow-up in the AMORIS Study were extracted. The following ICD codes were used to identify patients who had had any kind of stroke: ICD-7, 330–334; ICD-8 or ICD-9, 430–438; ICD-10, I60–I69 and G45. IS was identified on the basis of ICD-7 (332), ICD-8 (432–434), ICD-9 (433–434) and ICD-1 (I63), and haemorrhagic stroke according to ICD-7 (331), ICD-8 and ICD-9 (431) and ICD-10 (I60–I64).
Lipid measurements
TC and TG were measured by standard methods. The validation procedures have been reported previously.19 23 As the quality control did not include double entry of laboratory measurements and levels, we defined ranges for acceptance of lipid levels as follows: TC, 2.0–30.0 mmol/l; TG, 0.1–4.5 mmol/l. In a subpopulation of 505 patients with RA compared with 149 938 subjects without RA, apolipoprotein (apo) B and apoA-I were also measured, in addition to low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C), which were calculated according to the Jungner formula.15
Confounding variables
Hypertension status was not recorded in these subjects. However, 2142 (1.4%) subjects were hospitalised at some time before blood sampling with a discharge diagnosis of hypertension and were classified as having hypertension (ICD-8 codes 400–404, ICD-9 codes 401–405, ICD-10 codes I10–I15), although it is realised that such a method grossly underestimates the hypertension prevalence compared with direct measurement of blood pressure. Diabetes was defined in a similar way for those with a discharge diagnosis of ICD-7 (code 260), ICD-8 (codes 250.0–259.9), ICD-9 (code 250), ICD-10 (codes E10–E14). In addition, those with a fasting glucose measurement >7.0 mmol/l were classified as having diabetes. We found 5647 (3.8%) patients with diabetes.
Statistical methods
All analyses were adjusted for gender (where appropriate) and presence of confounding comorbidities (diabetes mellitus and hospital-diagnosed hypertension) before blood sampling. Further adjustments were made for age at blood sampling for patients without RA, and for age at onset of RA in patients with disease onset after blood sampling in the AMORIS Study, and for age at blood sampling for those who already had RA before entering the study. Differences in mean levels of TC and TG between RA and non-RA subjects were examined for each sex by analysis of covariance using RA as the fixed factor. Rates of AMI and IS were calculated as the number of patients with AMI or IS per 1000 observation years. Age-adjusted rates were calculated by the indirect method using all the AMORIS Study population, including RA and non-RA subjects, as standard. Age groups chosen were <40, 40–49, 50–59, 60–69, 70+, and age at blood sampling was used for all subjects in these calculations. CI of the indirectly age-standardised rates using the whole AMORIS Study population as standard was performed by relating a Poisson-distributed variable to the degree of freedom in the χ2 distribution.24 AMI case death was calculated as the proportion of fatal cases out of all AMI cases, including both hospitalised and non-hospitalised fatal cases. Differences in case deaths between genders were analysed by the χ2 test. A Cox regression analysis was used to calculate HR per 1 SD increase in TC or TG with 95% CI. The TC and TG difference in HR/SD between RA and non-RA subjects was tested by an interaction test.
Results
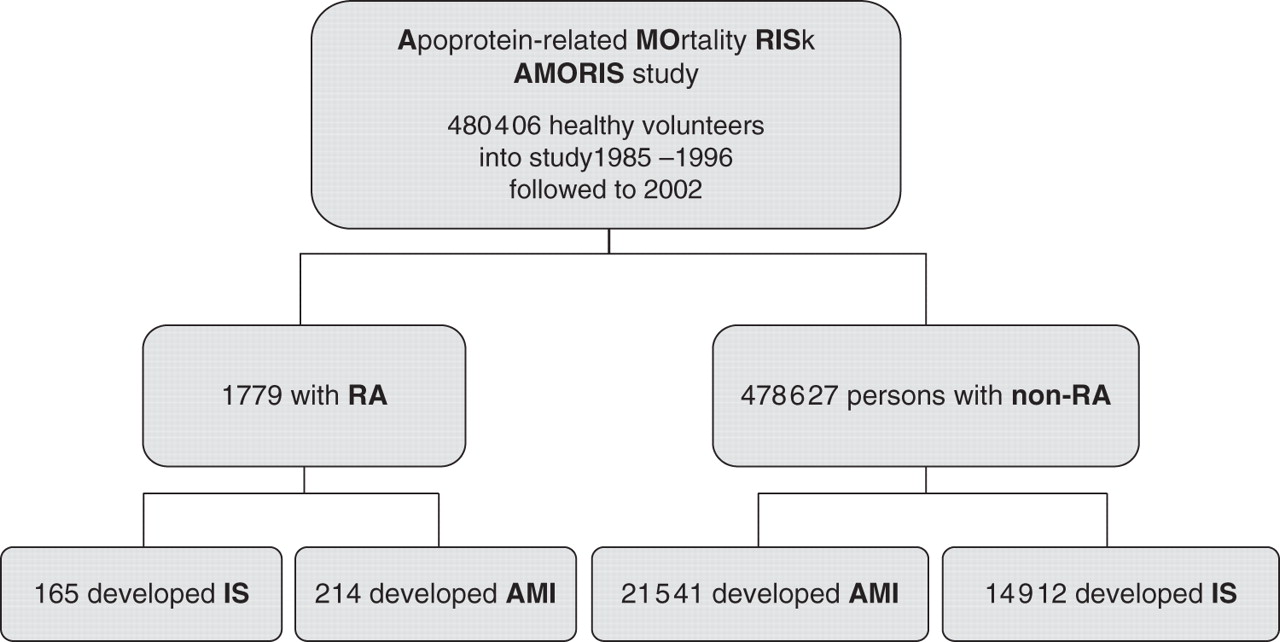
A total of 1779 people had RA, and 478 627 did not (figure 2). Female patients with RA were on average 8 years older than female subjects without RA, and male patients with RA were 7 years older than male subjects without RA. The RA population included 214 cases of AMI and 165 cases of IS, and the non-RA subjects included 21 541 who had had AMI and 14 912 who had had IS.

{kind=link}
{kind=link}
The AMORIS population. Cardiovascular end points for rheumatoid arthritis (RA) patients and non-RA persons. AMI, acute myocardial infarction; IS, ischaemic stroke.
Lipid levels
Both TC and TG were significantly lower in RA than non-RA, for both sexes, adjusted for age at onset of RA, hospital-diagnosed diabetes and hypertension (table 1). Patients with RA had hypertension and diabetes mellitus significantly more often than subjects without RA.
TC and TG in male and female subjects with and without RA
In a subsample of male patients with RA (n=163), it was found that the lower TC level (mean (SD) 5.66 (1.15) mmol/l) than in people without RA (6.00 (1.12) mmol/l) (p<0.0001) was partly due to significantly lower LDL-C (3.68 (0.97) vs 3.91 (1.01) mmol/l) (p=0.003) in RA vs non-RA, respectively) as well as lower non-HDL (4.30 (1.11) vs 4.60 (1.15) mmol/l) (p=0.0006). These findings were confirmed by lower apoB values (1.26 (0.32) vs 1.33 (0.33) g/l) (p=0.003). There was also a trend for lower HDL (1.37 (0.42) vs 1.40 (0.39) mmol/l) (p=0.26). However, apoA-I, the most important anti-inflammatory protein in HDL particles, was significantly decreased (1.32 (0.23) vs 1.37 (0.20) g/l) (p=0.01). Although not significant, similar trends for lower lipids and apolipoproteins were also observed in female patients with RA (n=342).
Rates of AMI and IS
The age-adjusted AMI rates were ∼1.7 times higher in patients with RA than in non-RA subjects (p<0.001). Of those with RA, men had AMI (both fatal AMI (FAMI) and non-fatal AMI (NFAMI)) more often than women (p<0.001), similar to the pattern in non-RA subjects. Furthermore, a higher AMI case death rate was observed in patients with RA than in non-RA subjects, and this difference was similar for both sexes (table 2).
Age-adjusted rates of AMI in patients with RA and in non-RA subjects per 1000 years
The rate/1000 years of any stroke in RA was higher in patients with RA than in non-RA subjects, but this was only significant for female patients with RA versus female subjects without RA (p<0.0001) (table 3). There was also a 1.6-fold higher rate/1000 years of IS in RA compared with non-RA. This increased rate/1000 years was significant for both sexes (p<0.0001). There were only 24 cases of haemorrhagic stroke. The unadjusted rate of haemorrhagic stroke/1000 years was not significantly higher in male patients with RA (1.04) than male subjects without RA (0.57) (p=0.17).
Age-adjusted rates of all strokes and IS per 1000 years
RA patients with IS more often had diabetes (n=15 (0.84%)) than subjects without RA (n=1 669 (0.35%)) (p=0.03). This pattern was similar for hypertension: RA (n=10 (0.56%)) vs non-RA (n=808 (0.17%)) (p=0.03). It was significantly more common for patients with RA than non-RA subjects to have both an AMI and IS (n=33 (1.85%) vs n=2293 (0.48%)) (p<0.0001).
Lipids as predictors of AMI and IS
HR/SD change in TC and TG for future AMI in patients with RA was nearly significant for TC (p=0.07) but not significant for TG (p=0.29) (table 4). Both lipid variables were significant predictors of AMI in non-RA subjects. An interaction test between the HR/SD of TC for future AMI in RA and non-RA was significant (p=0.003), meaning that the relation between TC and relative risk for AMI was significantly stronger in non-RA than RA subjects. The interaction test between TG for future AMI in RA and non-RA was not significant (p=0.33), meaning that the relationship between TG and future AMI was similar.
HR for AMI (a) and IS (b) by 1 SD of change in TC or TG adjusted for age, sex, hypertension and diabetes
TC was significantly predictive of future IS in patients with RA, as it was for those without RA (table 4), but the relationship between TG and IS was weaker in both populations. An interaction test between HR for future IS in RA and non-RA was not significant for either TC (p=0.42) or TG (p=0.81), meaning that relationships between TC and TG and IS in RA and non-RA were similar.
Discussion
The main findings in this study are that patients with RA had an increased rate of both AMI and IS, and that TC had a weaker association with future AMI in patients with RA than in non-RA subjects. TC had a weak positive relationship with future AMI in RA, while it was predictive of IS. In contrast, this and previous studies have shown that TC is a significant predictor of both future AMI and IS in non-RA.16 25 This difference in the association between TC and AMI may indicate that lipid lowering in patients with RA would have less effect than in people without RA. However, patients with RA have a much higher absolute risk of AMI and IS than people without RA, so a 1 mmol/l reduction in TC will be expected to save at least as many lives of patients with RA as those without. In addition, a retrospective analysis of the effect of lipid lowering by statins in RA patients with CVD showed that, despite patients with RA having lower lipid levels than those without RA, statins had the same lipid-lowering effect in both. Furthermore, the rate of CVD events after statin treatment was similar in RA and non-RA patients.26 Moreover, statins have anti-inflammatory effects, and hence a more pronounced CV risk-lowering effect could be anticipated. A prospective, randomised, placebo controlled trial with CV end points, such as the Trace RA Study,27 will answer this question, and give the opportunity to form guidelines for CVD prevention in patients with RA, similar to those for the general population.28 29 At present, only recommendations for CV risk management are available for patients with RA.30
Lipid profiles in RA are inconsistent, with various studies reporting increased, decreased or similar levels of TC and TG in comparison with control subjects.31,–,35 These discrepancies may be related to differences in populations studied, disease severity or disease duration. Low lipid levels in RA have been linked to severity of the disease, in particular the inflammatory status.36 37 Also, in other inflammatory joint diseases, such as psoriatic arthritis38 and ankylosing spondylitis,39 an inverse relationship between inflammatory status and lipid levels has been reported. There is unfortunately no information about disease severity or C-reactive protein levels in the AMORIS Study register.
The altered lipid profiles in RA occur as a result of the rheumatoid inflammatory process,40 indicating that the properties of the lipoprotein moieties are altered. The lipid profile in RA on the whole is atherogenic. Clinical studies have indicated that small, dense LDL particles are associated with higher risk of CVD,41 because of their high affinity for proteoglycans in the extracellular matrix of the arterial wall, as well as their high susceptibility to oxidative modification.42 43 Oxidative stress plays a key role in the pathogenesis of atherosclerosis44 and has been shown to be increased in RA.45 The lower TC with lower LDL and apoB levels in patients with RA in the AMORIS Study, together with the higher AMI rate, points to altered LDL type towards small, dense atherogenic LDL particles, which has also been demonstrated in patients with RA by Hurt-Camejo and coworkers.40 In addition, the low HDL and apoA1 (in the subpopulation of the AMORIS Study) indicates a lower antiatherogenic capacity of HDL. Several studies have shown that the properties of HDL are altered in RA, becoming less antiatherogenic with a lower antioxidative and anti-inflammatory capacity.46,–,48 Hypothetically, a less antiatherogenic HDL may be a feature in patients with RA in this study, who despite low TC and TG levels had a higher rate of AMI and IS.
The strength of this study is the prospective design. Our study followed 480 406 people for 12 years and included 1779 patients with RA, with 214 cases of AMI and 165 of IS. It is, to our knowledge, the first study to relate TC and TG levels to AMI and IS in patients with RA. There are power limitations with the HR/SD of TC and TG for future AMI in the RA population, and a post hoc power calculation showed that three times as many cases of AMI were needed to attain 90% power for TC having significant future prediction of AMI in RA. Interestingly, TC in our RA population tended to be more strongly related to IS than to AMI, which is clearly the opposite of findings in the general population. Although larger prospective studies investigating TC as risk factor for AMI in RA are warranted, such studies will be difficult to perform because of the low prevalence of RA in the community.
A limitation of this study is that only a subgroup was analysed for lipoprotein components. Therefore more detailed studies on lipoprotein components, comprising levels and function of apolipoproteins, are needed to shed light on their altered mechanistic function and relation to CVD in RA. Another limitation of this study is that data on treatment and traditional risk factors were not available. It is noted that discharge diagnosis of hypertension grossly underestimates the prevalence of hypertension compared with direct measurement. Furthermore, our data did not include smoking, which is a well-known CV risk factor. However, several large studies have shown that the predictability of lipoprotein components versus lipids for future AMI in the general population is not much affected by adjustment for multiple traditional risk factors.49,–,52 Thus it is not likely that the presence of risk factors would have had a major impact on our results.
The AMORIS Study relies on hospital-diagnosed data and may not have the same internal validity as randomised, placebo controlled, end point trials, which often operate with independent blinded end point committees with standardised criteria in their evaluations. Furthermore, our observations may not represent today's mortality from AMI in RA. More effective disease activity control by disease-modifying antirheumatic drugs may affect mortality in this patient population.53 54 The use of modern biological agents in the treatment of RA may shift this trend even more.55 Biological agents were not commonly used before 2002. Thus our results reflect the prebiological treatment period.
Despite lower levels of TC and TG, we found a higher rate of AMI and IS in patients with RA, and associations between TC and future AMI differed between patients with RA and people without RA. Our results indicate that TC levels have more limited value for prediction of future AMI and IS in RA than in the general population.
References
Footnotes
-
Funding This work was supported by grants from the Gunnar and Ingmar Jungner Foundation for Laboratory Medicine, Stockholm, Sweden.
-
Competing interests None. Johannes Bijlsma was the Acting Editor.
-
Ethics approval This study was conducted with the approval of the ethics review board of the Karolinska Institution.
-
Provenance and peer review Not commissioned; externally peer reviewed.