Article Text

Abstract
Objectives Patients with rheumatoid arthritis (RA) have a higher mortality than the general population, and this increased mortality is related to demographic and disease variables. N-terminal pro-brain natriuretic peptide (NT-proBNP) is a predictor of mortality both in general and patient populations, but has not been shown to predict mortality in patients with RA. This study examines whether NT-proBNP can further improve the prediction of mortality in RA.
Methods 182 patients with RA of 5–9 years disease duration were comprehensively examined in 1997. Serum samples were frozen and later batch analysed for NT-proBNP levels and other biomarkers. Adjusted univariate and logistic regression analyses were performed with death within the 10-year follow-up period as the dependent variable. Significant predictors were also examined as dichotomised variables.
Results Mortality was predicted in univariate analyses by the following variables: age, sex, homozygosity for HLA-DRB1 shared epitope alleles, Health Assessment Questionnaire, 28-joint Disease Activity Score (DAS28) and NT-proBNP. A multivariate model with age, sex, DAS28 and NT-proBNP as independent variables showed the greatest discrimination.
Conclusion NT-proBNP provided incremental information in the prediction of mortality in this cohort of patients with RA.
Statistics from Altmetric.com
Introduction
Mortality in patients with rheumatoid arthritis (RA) is increased compared with the general population by at least 50%.1,–,3 The excess mortality is largely due to cardiovascular disease (CVD), but malignancies and infections are also increased.1 The absolute risk of death from CVD is highest for elderly men with RA whereas the relative risk is highest for young women.4 Established predictors for all-cause mortality in patients with RA are age, male sex, physical function, comorbidities and rheumatoid factor (RF).1 5 A homozygote shared epitope (SE) genotype has been found to be associated with premature death, and specifically death from ischaemic heart disease.6,–,8 Inflammatory markers such as C reactive protein (CRP) and erythrocyte sedimentation rate (ESR) have also been shown to be important risk indicators in RA, pertaining to general mortality, CVD mortality and cardiovascular events.9 10
The level of N-terminal pro-brain natriuretic peptide (NT-proBNP) predicts all-cause and cardiac mortality in the general population, as well as in cohorts of patients with heart failure and stable coronary heart disease.11,–,14 NT-proBNP has been found to be increased in patients with RA and is cross-sectionally associated with the level of inflammation.15 16 As far as we know, NT-proBNP has not been investigated as a predictor of mortality in patients with RA.
Our hypothesis was that NT-proBNP is an independent predictor of 10-year mortality in patients with RA. We have thus examined the incremental value of NT-proBNP in the prediction of mortality in RA across a panel of established and potentially novel risk factors.
Material and methods
Patient cohort
One hundred and eighty-two patients with RA participated in the 5-year follow-up of the EURIDISS study in 1997. Data from this comprehensive visit are used as the baseline for the analyses in this paper.17 The patients were diagnosed according to the 1987 American College of Rheumatology criteria.18 The mean age at baseline was 55.7 years (range 27.3–74.7), mean disease duration was 7.1 years (range 4.76–9.4) and 134 (74%) were women. Eighteen patients (17%) reported previous CVD. At the 10-year follow-up in 2007, 31 (17%) of the patients had died.
Baseline variables 1997
A questionnaire recording data on demographics, comorbidities and health status was completed by patients in collaboration with the study nurse. Health status was measured by the Stanford Health Assessment Questionnaire (HAQ), a multidimensional questionnaire that captures patient functioning in several areas of daily life,19 and by the generic Nottingham Health Profile (NHP).20 A checklist modified from Arthritis Impact Measurement Scales was used to assess the presence of 16 possible comorbidities including patient self-reported presence of hypertension, angina, myocardial infarction or other cardiac diseases and diabetes, without any diagnostic specifications.21 The trained study nurse also performed a clinical examination for the presence of nodules and joint swelling and the composite Disease Activity Score was calculated (DAS28 consisting of tender joint score, swollen joint score, ESR and patient visual analogue scale for global assessment).22 Biomarkers were examined from blood (DNA) and serum samples that had been frozen at −70°C: anti-cyclic citrullinated antibody (anti-CCP) by ELISA (Inova Diagnostics, San Diego, California, USA), high sensitivity CRP by phyCardioPhase, nefelometry (Dade Behring, Deerfield, Illinois, USA) and RF IgM using the in-house ELISA method.
NT-proBNP was measured using a Modular E170 device (Roche Diagnostics, Mannheim, Germany). The coefficient of variation on batch analyses was 1.4%. DRB1 sequencing was performed using BigDye Terminator V3.1 chemistry (Applied Biosystems, Foster City, California, USA) on an ABI 3730 DNA Analyzer (Applied Biosystems) followed by allele assignment (AssignSBT V.3.2.7; Conexio Genomics, Applecross, Australia). SE was defined as the following alleles: 0101, 0102, 0401, 0404, 0405, 0408, 1001 and 1402.
Haemoglobin and ESR were analysed at the time of examination.
Outcome measures
The patients were registered as dead at the 2007 follow-up study on the basis of information from the Norwegian National Population Register.
Statistical analyses
Baseline demographic disease activity, comorbidities, health status variables and levels of soluble biomarkers were compared between patients who had died at the 10-year follow-up and the survivors using the χ2 test, Student t test or Mann–Whitney U test as appropriate. Two-tailed p values are reported.
The associations between baseline variables and 10-year mortality were examined in a logistic regression procedure that was adjusted for age and sex. Variables that were significantly skewed were transformed into the natural logarithm (CRP, ESR, NT-proBNP) or dichotomised at the median (NHP and HAQ). Anti-CCP and IgMRF levels were classified as elevated if ≥25 U/ml. Separate models were constructed for associated variables. Finally, a multivariate stepwise backward regression model was constructed that initially included all variables that were significant at the p≤0.15 level. The validity of the final model was confirmed by performing sensitivity analyses with NT-proBNP dichotomised according to the age and sex-specified 95th percentile in healthy blood donors,23 and by forcing baseline CRP and history of CVD into the model. Previously excluded variables of baseline disease activity were also re-entered into the final model to check for possible confounding. To verify that the models were not overfitted, variables that were significant predictors of mortality in the separate models were dichotomised at the median and, for each predictor, a sum variable was constructed that also included age and sex (eg, age > median =1 + female sex =1 + HAQ ≤ median = 0). NT-proBNP was then added to the logistic models that included one such sum variable and improved prediction was assessed by examining the CI of the receiver operating characteristics (ROC) curves. The relationship between NT-proBNP and mortality was additionally explored using fractional polynomial analysis in STATA. In addition, we checked for model lack of fit by applying the Hosmer–Lemeshow goodness-of-fit test to the final model and, finally, we plotted Cook's distances and repeated the final step of the analyses after the removal of outliers. When not otherwise mentioned, the analyses were performed using SPSS Version 14.
Results
Of the 182 patients, 31 had died during the 10-year follow-up period. Details of missing data are given in table 1. Complete baseline data for variables included in the final model were available for 117 patients, 21 of whom had died during the 10-year follow-up period. These patients were similar to the main cohort with regard to age and level of IgM RF, anti-CCP, HAQ and DAS28, but fewer women had participated in the complete data collection (complete data were available for 76.6% of men vs 60.0% of women, p=0.04).
Comparison of baseline variables between patients who were dead (n=31) and those who were alive (n=151) after 10 years of follow-up
Bivariate analyses
As expected, the patients who had died were older, more often male, had a higher frequency of CVD-related comorbidities and poorer functional status (HAQ and NHP) at baseline. They also had higher baseline levels of DAS28, and NT-proBNP, CRP and ESR levels were borderline significantly increased in patients who died (p=0.08 and p=0.06, respectively; table 1).
Logistic regression
Significant and borderline predictors of 10-year mortality are shown in table 2. In the demographic model, homozygous SE adjusted for age and sex correctly predicted 8 of 29 deaths. Level of education was not a significant predictor of mortality (OR 0.90, 95% CI 0.32 to 2.49). Among the variables of disease activity, only DAS28 was a significant predictor with a prediction of 10 of 30 deaths. The rejected variables were nodules (OR 1.20, 95% CI 0.39 to 3.65), anti-CCP (OR 1.60, 95% CI 0.54 to 4.77) and IgM RF (OR 0.85, 95% CI 0.30 to 2.37).
Logistic regression models for the prediction of death during 10-year follow-up (OR (CI) and p value)
None of the comorbidities were significant predictors at p≤0.05, although a history of myocardial infarction approached this level. Neither hypertension (OR 1.32, 95% CI 0.45 to 3.85) nor diabetes (OR 1.11, 95% CI 0.26 to 4.77) contributed to the model. The dichotomised variables reflecting health status (NHP and HAQ) were both significant in the adjusted analysis, but NHP was surpassed by HAQ in a multivariate ‘health status model’ and lost significance. A high NHP score adjusted for age and sex predicted 7 of 27 deaths (OR 3.22, 95% CI 1.18 to 8.80) whereas a higher HAQ score predicted 16 of 30.
NT-proBNP was found to be an independent predictor in the ‘biomarker model’ predicting 12 of 23 deaths. LnCRP was also a near-significant predictor of death in the age and sex-adjusted model (OR 1.48, 95% CI 0.95 to 2.31) but did not perform when NT-proBNP was included in the model. LnESR (OR 1.42, 95% CI 0.80 to 2.51) did not carry significance in the model.
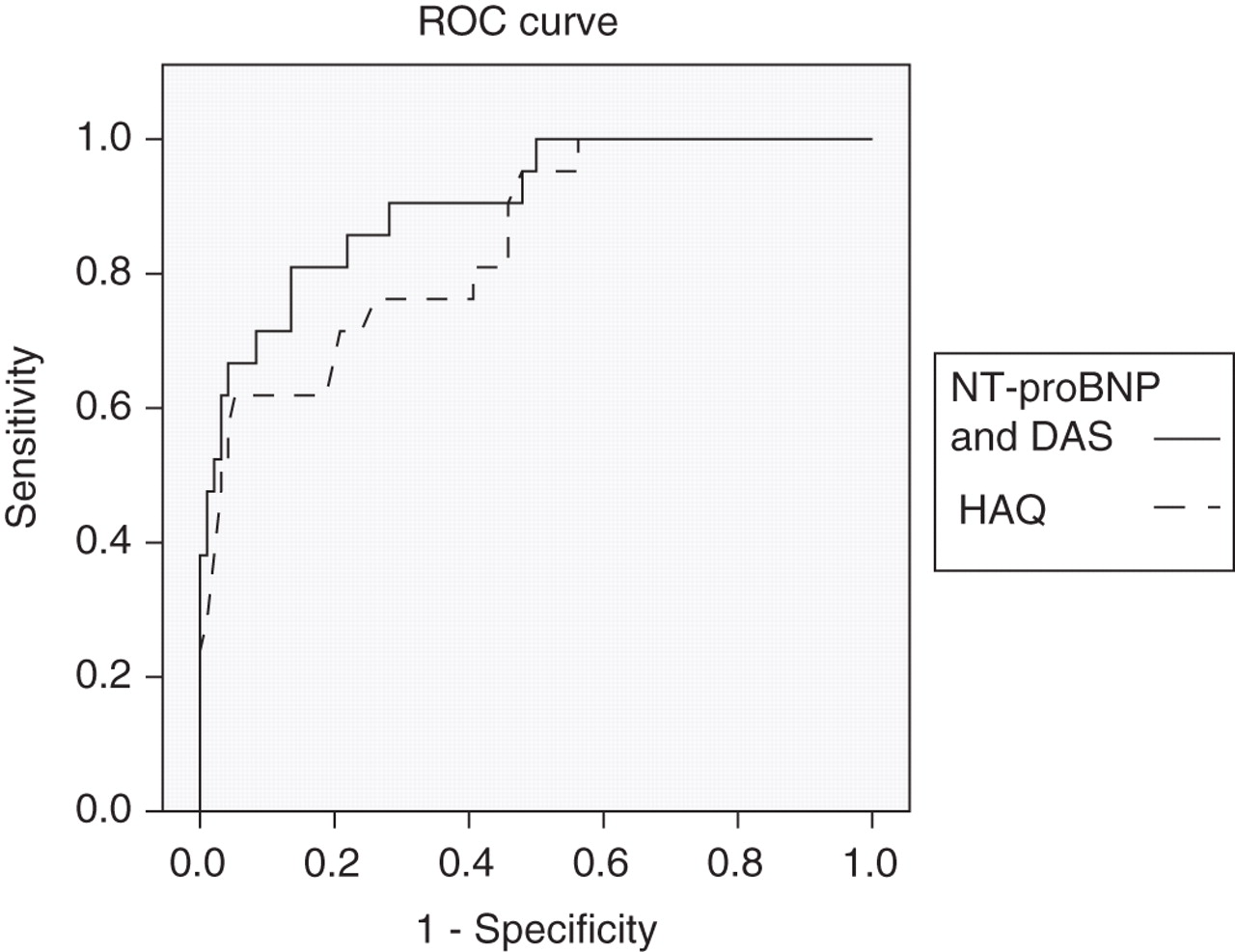
The final model included DAS28 and NT-proBNP and predicted 14 of 21 deaths. The positive predictive value of the model was 74% and the negative predictive value was 93%. The ROC curves comparing the final model with the health status model showed that the combination of DAS28 and NT-proBNP had the greatest area under the curve (AUC), although the CIs were overlapping and the difference was thus not significant (figure 1).

{kind=link}
Receiver operating characteristics (ROC) curves comparing the performance of two models predicting mortality after 10 years. Models adjusted for age and sex. Area under the curve for N-terminal pro-brain natriuretic peptide (NT-proBNP) and Disease Activity Score (DAS) model 0.91, for Stanford Health Assessment Questionnaire (HAQ) model 0.85.
The sensitivity analyses supported the main results. NT-proBNP categorised according to the age and sex-specific 95th percentile provided by the manufacturer in package inserts (based on samples from 2264 blood donors and patients aged between 18 and 65 and free from CVD)23 was a slightly poorer predictor of death than the continuous variable (sensitivity 62%, specificity 95%, accuracy 89%). The final model was not significantly altered by forcibly re-entering previously rejected variables (including self-reported CVD and hypertension), and no other variables were found to be significant predictors of the outcome nor to be confounders of the included variables. Consecutive models that each included one sum variable showed that NT-proBNP remained a significant predictor of mortality and contributed significantly to each model (data not shown). According to the fractional polynomial analyses, the relationship between NT-proBNP and death was best described by a linear equation. The model exhibited no evidence of lack of fit (Hosmer–Lemeshow, p=0.46) and was not substantially changed after the removal of three outliers.
Discussion
Our results show that NT-proBNP is an independent predictor of 10-year mortality in this cohort of patients with longstanding RA. Established risk factors for RA mortality were also significant predictors in our cohort and the HAQ score, adjusted for age and sex, had the highest single variable discriminatory power.
Biomarkers are quantifiable biological parameters that serve as important indices of healthy or pathological processes.24 Biomarkers reflecting RA disease activity can be grouped into two clusters, the variables in each cluster being mutually closely correlated. One cluster includes variables that describe patient-centred outcomes; these may be derived from patient self-reported questionnaires of which the HAQ score is an example. The other cluster includes measures of RA disease-centred outcomes such as ESR, CRP, RF and radiographic joint erosions. In general, patient-centred outcomes are reported to be better predictors of mortality than disease-centred variables1 although, to our knowledge, they have not previously been compared with SE or NT-proBNP. NT-proBNP as a single variable (adjusted for age and sex) had approximately the same predictive ability as the HAQ score. The final model that included DAS28 was superior to other models, although the CIs of the ROC curves were not significantly different.
NT-proBNP is a validated marker of heart failure that has been shown to complement traditional risk factors as an independent predictor of all-cause mortality in a community cohort.25 This biomarker is the biologically inactive N-terminal fragment of the active hormone BNP and is part of a family of natriuretic peptides that cause vasodilation, natriuresis and smooth muscle modulation in response to myocardial stretch.26 NT-proBNP and BNP release may also be upregulated by proinflammatory cytokines.27 It is thus possible that measures of inflammation or RA disease activity could attenuate the link between NT-proBNP and mortality. In the failing heart, NT-proBNP levels can accordingly be reduced by medication that improves cardiac function28 and, interestingly, a recently published paper found that NT-proBNP is also reduced in patients with RA by treatment with a tumour necrosis factor α inhibitor.29 In our final model, NT-proBNP was maintained as a significant predictor of mortality when self-reported CVD, self-reported hypertension and current inflammation were forcibly imputed into the model.
The observed yearly all-cause mortality in this cohort was 1.7%. A 4% yearly mortality has been observed in another Norwegian study on data collected from 1977 to 1992, two decades prior to our inclusion date.3 Our observed yearly mortality was also lower than the 2.4–2.5% observed in the Minnesota cohort, although our data are within the CIs of the Minnesota findings.30 The average age in these cohorts seems comparable, and we believe that the lower mortality observed in our study might be explained by the more recent data collection, mirroring the reduced mortality seen in the general population. The EURIDISS study is an inception cohort that specifically included patients with >5 and <10 years of disease duration and, as death in RA has been found to be increased early in the disease course, this may have biased our results towards a lower mortality.31
One strength of our study is the prospective longitudinal design with subsequent batch analyses of baseline soluble biomarkers. The results of this study confirm several previous findings concerning predictors of mortality in RA, providing validity to our findings. The main weakness of this study is the sample size which may lead to a type II statistical error regarding less powerful predictors. Hypertension and presence of diabetes were not significant predictors of mortality in our models, and this may well be due to the low number of patients with these conditions. We chose to use the 1997 examination as the baseline as information on CVD had been collected at this time point. However, we do not have details of ventricular function, renal function, lipid levels or smoking habits from this visit, all of which are possible predictors and confounders. Ideally we should have entered NT-proBNP into multivariate models that already included composite and extensively validated scores, such as the Framingham score, in order to discern whether NT-proBNP can further improve prediction of mortality in addition to these widely used predictors. Lack of knowledge about the cause of death prohibited subgroup analyses but, because of the limited number of patients, the cohort would not have been eligible for robust subgroup analyses according to cause of death.
In summary, NT-proBNP compared favourably with the established predictors of mortality in this cohort of patients with RA. The resultant model gave an improved sensitivity, specificity and the highest AUC of the ROC analysis. Additional studies are encouraged to replicate and further explore the value of NT-proBNP as a prognostic biomarker in RA.
Acknowledgments
The authors thank Benedicte Lie and Siri T Flåm for genotyping the patients with regard to HLA-DRB1 and Petter Mowinckel for providing statistical expertise. They also thank Roche Diagnostics, Mannheim, Germany for providing the kits for NT-proBNP testing (Dr B Trauth).
References
Footnotes
-
Funding This study was supported by grants from the Eastern Norway Regional Health Authority. The data collection in EURIDISS was supported by The Research Council of Norway, The Norwegian Rheumatism Association, The Norwegian Women Public Health Association, the Grethe Harbitz Legacy and the Marie and Else Mustad's Legacy.
-
Competing interests None.
-
Ethics approval The project was approved by the Norwegian Regional Committee for Research Ethics.
-
Patient approval Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.