Article Text

Abstract
The characteristic radiographic hallmarks of chronic gouty arthritis are the presence of macroscopic tophi and erosions with overhanging edges and relative preservation of the joint space. In recent years there has been more insight into the processes underlying the development of bone erosions in gouty arthritis. This review discusses the mechanical, pathological, cellular and immunological factors that may have a role in the pathogenesis of bone erosions in gouty arthritis. It highlights the evidence suggesting that monosodium urate crystal deposition is associated with the presence of underlying osteoarthritis and the important role of osteoclasts and the receptor for activation of nuclear factor κ B (RANK) and RANK ligand (RANK–RANKL) pathway in the pathogenesis of gouty erosions. Gouty arthritis is primarily driven by interleukin 1β (IL-1β). IL-1β has been implicated in bone destruction and erosions in other inflammatory arthridities. Thus, future IL-1 inhibitors may prevent and treat erosion formation due to tophaceous gouty arthritis. This review discusses imaging modalities and highlights ultrasongraphic evidence suggesting a significant relationship between the presence of the gouty tophus and bone erosions as well as the frequent presence of persistent low-grade inflammation in asymptomatic chronic tophaceous gouty arthritis on high-resolution ultrasonography. It is the tophus eroding the underlying bone that is pivotal for the development of bone erosions in gouty arthritis.
Statistics from Altmetric.com
Introduction
In 1859 Garrod1 proclaimed that ‘the deposited urate of soda may be looked upon as the cause, and not the effect, of gouty inflammation’. This statement remains as true today as it was then. The association between gouty arthritis and monosodium urate (MSU) crystal deposition has been clearly established. Gouty arthritis results from a chronically increased uric acid pool and is the most common inflammatory arthritis in men aged >40 years.2 It has been described as a chronic disease characterised by four distinct stages. These include (1) asymptomatic hyperuricaemia; (2) acute gouty attacks; (3) an intercritical period in which the gouty patient has already had a gouty attack but is free of acute attacks; and (4) advanced destructive gouty arthritis. It has recently become clear that, during the intercritical period when the patient is asymptomatic, chronic inflammation is often present.3
In this paper we review the recent insights into the complex mechanical, pathological, cellular and immunological processes leading to bone erosions in gouty arthritis and appraise how ultrasonography has improved our understanding of processes leading to bone erosions in gouty arthritis.
Association of gouty arthritis with osteoarthritis
In 1957 Sokoloff4 proposed in his paper on the pathology of gouty arthritis that ‘commonly, tophi communicate with urates on the articular surface through defects in the articular cartilage in the osteoarthritic joint’. Further, he stated that tophaceous deposits can erode into the bone, cartilage and tendons, causing significant structural damage.4
MSU crystal deposition is associated with the presence of osteoarthritis (OA). Joints affected by OA are more predisposed to having MSU crystal deposition in patients with gouty arthritis. Garrod5 examined postmortem the first metatarsophalangeal (MTP) joints of 40 patients who had a hallux valgus deformity. These patients did not suffer from gouty attacks during their lifetime. Using polarised light microscopic inspection of fresh tissue sections cut by hand with a razor blade to identify MSU crystals, he found 2 of the 40 patients to have MSU crystal deposition.6
Simkin et al7 suggested that MSU crystal deposition in the distal interphalangeal (DIP) joints occurred largely due to pre-existing OA in these joints. They hypothesised that transient increases in the urate concentration of resolving synovial effusions resulting from the differential permeability of synovium to urate and water in OA-affected joints might encourage nucleation and precipitation of MSU crystals. Others have also reported gouty arthritis in interphalangeal nodal hand OA.8,–,10 A significant association with OA was seen in a study by Roddy et al11 at the first MTP joint, mid foot, knee and DIP joints. Roddy et al11 found a strong association between joint sites affected by acute attacks of gout and the presence of clinically apparent OA. They hypothesised that OA may result in changes in tissue factors—either an increase in promoters or a reduction in inhibitors of crystal nucleation and growth—which might predispose to MSU crystal deposition. Why some OA joints are favoured to have tophi above others could be due in part to increased stress on the involved joint and changes in joint pressure. For example, patients with OA of the first MTP, a common site for tophi, have significantly greater maximum forces and peak pressures under the hallux during gait than patients without OA of the first MTP.12
The increased incidence of MSU crystal deposition and gouty arthritis with ageing13 may be related to the changes that occur in cartilage and connective tissues. The proposed mechanisms facilitating crystal deposition include a reduction in blood flow that may cause a local increase in MSU crystal formation,14 as well as changes in the relative proportions of the glycosaminoglycans and proteoglycans15 and an increase in the intracellular and extracellular lipid content of the articular cartilage.16 Burt and Dutt17 found that chondroitin sulfate and phosphatidylcholine fostered crystallisation of MSU crystals in vitro resulting in MSU crystal deposition in tissues. Chondroitin sulfates and phosphatidylcholine are normal constituents of the matrix of joint tissues and hyaline cartilage. They are continuously released into the synovial fluid where their concentration and sulfation pattern reflect joint tissue metabolism. Both OA and ageing may cause changes that contribute to MSU deposition by reducing inhibition to MSU crystallisation and/or activation of promotors of MSU nucleation.
Histopathology
Most patients with hyperuricaemia never show evidence of urate crystallisation or develop gouty arthritis. Urate deposition, when it occurs, is usually in connective tissues. MSU crystals are found in cartilage, tendon sheaths, synovial fluid and subcutaneous tissue.4 Avascularity of connective tissues, especially cartilage, is often held as the main predisposing factor for urate deposition. However, MSU crystals may deposit in the synovial membrane which is moderately vascular, especially when it is inflamed.13 The earliest articular changes result from crystal deposits. These tophi ‘soon spread on to and over the joint surface until the articular cartilage looks’ as if it is ‘coated with sugar-icing’.18 Tophi can be intra-articular, periarticular or extra-articular.
A tophus is composed of MSU crystals in a matrix of lipids, protein and mucopolysaccharides.4 Gouty tophi are characterised by foreign body granulomas consisting of mono- and multinucleated macrophages surrounding deposits of MSU microcrystals.19 Several zones have been identified within the tophus.20 These include a central zone that consists of a MSU crystal deposit surrounded by a cellular zone, the corona zone. Large numbers of macrophages, mast cells and plasma cells were detected within the corona zone of the tophus.20 The cells of the corona zone form a well-defined compact zone which is demarcated from both the central MSU crystal deposit and the surrounding fibrovascular zone.
It is proposed that the granulomatous response in bone and joints leads to erosions and bone destruction. Erosion formation mediated by granulomas has been described in sarcoidosis and tuberculosis. Interleukin 1 (IL-1), a proinflammatory cytokine which contributes to granuloma formation in other diseases such as tuberculosis, may be contributing to tophus and erosion formation in gouty arthritis.21 The cells surrounding the crystals in the tophus are fibrocytes, macrophages, other mononuclear cells and some foreign body giant cells. The tophus can erode the underlying bone possibly via an IL-1-driven mechanism. It often appears as a relatively discrete soft tissue nodule adjacent to a bony erosion.22 Tophi in subchondral bone are associated with collapse and resorption of trabeculae producing a punched out-like space as seen in conventional x-rays and tissue specimens. In addition, subperiosteal marginal MSU deposits have been seen.23 Dalbeth et al24 found a close relationship between the presence of subcutaneous tophi and CT abnormalities and suggested that subcutaneous tophi serve as a marker of underlying joint and bone damage in gout. They proposed that the intraosseous tophi were extensions of chronic granulomatous synovitis within the joint or that the MSU crystal burden affects the magnitude of associated synovitis. In summary, tophi may precede the development of bone erosions with subsequent invasion of the tophus into bone leading to bone erosions. The overhanging appearance of erosions in gout fits well with a mechanical origin, the overhanging border being more likely to be produced by the lateral push of the tophi growing inside the erosion and producing it than from an eroding process from the bone surface, a mechanism more likely in rheumatoid arthritis (RA).
Cellular mechanisms
In a normal physiological state there is a balance between old bone that is resorbed and new bone that is formed. Osteoclasts, which are of the monocyte macrophage lineage, are responsible for bone resorption and erosion formation.25 Marrow stromal cells or their osteoblast progeny express two molecules essential for osteoclastogenesis. These are the macrophage colony-stimulating factor (M-CSF) and the receptor for activation of nuclear factor κ (RANK) B ligand (RANKL). The soluble decoy receptor osteoprotegerin (OPG) competes with RANK for RANKL. Relative expression of RANKL and its antagonist OPG controls osteoclastogenesis.25 The RANK–RANKL pathway is important for bone remodelling under both physiological and inflammatory conditions.
Joint destruction has been extensively studied in RA and is characterised by destruction of articular cartilage and by excessive bone resorption.26 The cellular mechanisms of cartilage and bone destruction have been studied in humans and experimental models of RA. These studies27,–,30 found mature osteoclasts to be prominent at bone erosion sites in RA inflamed joints. Accumulation of osteoclasts in inflamed joints leads to an imbalance between bone resorption and bone formation and promotes an unfavourable bone homoeostasis.31 Blocking essential molecules for osteoclastogenesis or using mice deficient in osteoclasts revealed the essential functions of osteoclasts in triggering inflammatory bone erosions.32 Thus, it has been shown that erosions are not formed when osteoclasts are effectively blocked or genetically depleted, despite the presence of synovial inflammation.
In gouty arthritis, local production of enzymes within the tophus that degrade bone and cartilage matrix may contribute to the development of erosions. Matrix metalloproteinases (MMPs) are implicated in unmineralised cartilage erosion formation while osteoclasts resorb calcified bone matrix and are implicated in bone erosion formation.33 Schweyer et al34 have shown that there is continuous recruitment of macrophages into the gouty tophus. These macrophages produce the proinflammatory cytokine tumour necrosis factor (TNF) as well as two TNF-inducible lytic enzymes, MMP-2 and MMP-9.31
In patients with gouty arthritis, osteoclast-like cells were found to be prominent within tophi and at the interface between soft tissue and bone.35 MSU crystals can reduce the anabolic effects of osteoblasts, thereby contributing to damage to the juxta-articular bone.36 Peripheral blood monocytes from patients with severe erosive gouty arthritis transformed into osteoclast-like cells following stimulation with RANKL and M-CSF.35 Thus, MSU crystals seem to alter the RANKL–OPG balance within stromal cells, thereby indirectly promoting osteoclastogenesis in patients with gouty arthritis. The expression of RANK–RANKL–OPG within the tophus or bone itself remains to be investigated. Could treatments directed at blocking the osteoclast differentiation or activity help prevent or retard the progression of bone erosions in gouty arthritis?
Proinflammatory cytokines
The increase in proinflammatory cytokine levels in active inflammation plays an important role in bone damage. Proinflammatory cytokines such as TNFα, IL-1, IL-6 and IL-17 as well as M-CSF are potent inducers of RANKL expression and thus can enhance osteoclast differentiation. TNFα acts on osteoclast precursors in addition to its inflammatory action,37 while IL-1α and IL-β act directly on osteoclasts. It is important to note that TNF is a potent inducer of IL-138 which itself is a crucial mediator in the pathogenesis of bone destruction in inflammatory arthritis. IL-1β is a crucial factor in preclinical models of inflammation-induced bone erosions.
IL-1 is a key molecule in TNF- and RANKL-induced osteoclast formation.39 40 It regulates RANK expression and thereby affects the susceptibility of osteoclasts not only to RANKL but also to TNF, which works through RANKL induction as well.40 The effects of the IL-1 receptor antagonist IL-1Ra on surrogate markers of bone erosion and cartilage damage appear to be superior to its effects on inflammation.41 Beneficial effects on joint inflammation and cartilage and bone destruction have been observed in an animal model of inflammatory arthritis in which the animals were treated with IL-1Ra.42 In another study,43 administration of IL-1 antibodies prevented bone and cartilage destruction whereas inhibition of TNFα failed to do so and only decreased synovitis in an animal model of collagen-induced arthritis. This study supported the importance of IL-1 in bone destruction and erosions in inflammatory arthritis. It is important to note that IL-1 has the potential to induce osteoclast differentiation independent of RANKL/RANK interaction. IL-1 was found to directly induce osteoclastogenesis through the IL-1R type 1 receptor whose expression is, in turn, upregulated by osteoclast-inducing factors such as RANKL and TNFα.44 In RA, blockade of both IL-1 and TNFα activity can reduce joint inflammation and retard the progression of bone erosions.45
It has become apparent as a result of recent renewed interest that the inflammatory process in gouty arthritis is primarily driven by IL-1β.46 MSU crystals stimulate IL-1 release by monocytes and synovial mononuclear cells47 as well as the cryopyrin (NACHT domain-, leucine-rich repeat- and PYD-containing protein 3) inflammasome, an intracellular multiprotein complex. Cryopyrin regulates activation of the protease caspase-1 which, in turn, controls the activation of IL-1β. Once caspase-1 becomes active it cleaves the pro-IL-1β molecule to release the shorter mature p17 form which constitutes the active IL-1β molecule (figure 1).46 The release of IL-1β46 48 promotes neutrophil influx into the joint and joint inflammation ensues. In addition, it is of utmost importance that a large number of cells expressing IL-1β are present within the tophus itself.49

Activation of the cryopyrin (NLRP3) inflammasome by monosodium urate (MSU) crystals triggers the production of interleukin 1β (IL-1β).
Literature examining the role of TNFα in gout is scarce. Several case reports discuss the benefit of TNF inhibition in chronic tophaceous gout.50,–,52 Animal studies by So et al53 showed the effectiveness of IL-1 inhibition in preventing neutrophil trafficking to the peritoneum, whereas TNF inhibition aggravated neutrophil influx. This is in contrast to results reported by Chapman et al54 who found that TNF inhibition inhibited MSU crystal-induced endothelial activation, as evidenced by scintigraphy, in a porcine monarthritis model. These differences may be due to differences in the TNF inhibitors used. More studies are needed to evaluate the use of TNF blockade in gout.
Drug treatment of acute gouty arthritis using IL-1 inhibition
Most patients with acute gouty arthritis can be managed effectively with non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids and/or colchicine. However, many patients have comorbidities or contraindications to the use of these medications. Recent studies in gouty arthritis have shown IL-1 inhibition to have a beneficial effect. So et al studied the response to IL-1Ra. Anakinra at a dose of 100 mg per day was administered subcutaneously for 3 days to 10 patients with acute gout. They reported a 78% response in their pilot study of 10 patients, thus significantly relieved the pain following acute gout53 Another IL-1 inhibitor, an IL-1 trap, rilonacept (arcalyst) given at a dose of 160 mg subcutaneously once a week decreased disease activity and pain in patients with chronic active gouty arthritis.54 Yet another IL-1 inhibitor currently in clinical trials is canakinumab (Ilaris), a fully human monoclonal anti-human IL-1β antibody which binds to human IL-1β and thus blocks the interaction of this cytokine with its receptors. It does not bind to either IL-1α or IL-1Ra. A phase II study to determine the target dose of canakinumab in the treatment of acute gouty attacks in patients refractory to or with a contraindication to NSAIDs and/or colchicines has been completed.55 A statistically significant response was observed at 72 h for canakinumab 150 mg given subcutaneously. The median time to 50% reduction in pain was 1 day with canakinumab 150 mg compared with 2 days for patients treated with triamcinolone acetonide (p=0.0006).55
Imaging
Conventional radiography
The assessment of bone damage in gouty arthritis traditionally relied on conventional radiography (CR) in which bone erosions serve as a marker of joint damage. Typical well-defined ‘punched out’ periarticular erosions with overhanging edges may not be seen with CR until 6–12 years after the initial acute attack.56 57 The overhanging edges are caused by a gradually expanding tophus eroding at the bone cortex with concomitant new periosteal bone formation trying to contain the tophus.58 CR may underestimate the size and extent of soft tissue and osseous involvement by tophi.59
Computed tomography
CT is a more sensitive method for detecting tophi and erosions than CR.60 Dalbeth et al,61 in a systematic CT analysis of individual joints in patients with chronic gouty arthritis, demonstrated a strong relationship between bone erosions and intraosseous tophi; 82% had visible tophi where CT identified bone erosions whereas large erosions (>7.5 mm diameter) were always associated with tophi.61 Dalbeth et al62 have shown that CT is able to assess subcutaneous tophus volume in a reliable and reproducible manner.
Dual-energy CT
Dual-energy CT (DECT) is a new technique that allows differentiation of materials and tissues based on CT density values. Compounds with different anatomic weights absorb x-ray beams differently. The DECT uses two x-ray tubes rather than one. The material-specific differences in attenuation between the high and low tube voltage acquisitions (80 and 140 kV) allow accurate and specific characterisation and separation of MSU crystals from calcium. Using a specially designed software program, MSU crystal deposits and calcium can be differently colour coded. Thus, DECT offers a non-invasive way of identifying MSU crystal deposits63 as well as measurement of total body urate burden.64 DECT could be useful in detecting subclinical tophus deposits and the extent of the tophaceous burden, which we have probably been underestimating in patients with gout.
Magnetic resonance imaging
MRI helps establish bone damage and erosions early in the disease.65 The signal intensity characteristics of tophi have been reported to be homogeneous and generally isointense to muscle on T1-weighted images. The reported imaging findings of tophi on T2-weighted images have varied, but the intermediate to low heterogeneous signal intensity in a tophus on T2-weighted images has been reported to be seen most frequently.66 Variable degrees of MRI enhancement of tophi following intravenous gadolinium have been reported. The patterns of enhancement have varied from homogeneous to heterogeneous and peripheral enhancement.67 The presence of the peripheral enhancement pattern supported the diagnosis of gouty arthritis.66 Peripheral enhancement is not typical of chronic RA, pigmented villonodular synovitis or chronic infectious arthritis and is supportive of our findings described in the section below.
High-resolution ultrasound
High-resolution ultrasound (HRUS), using transducer frequencies between 12 and 18 MHz, can demonstrate very good anatomical detail and pathology. The physics of ultrasound (US) make it an ideal tool to detect crystalline material in soft tissues. For many years it has been used to detect calcified gallstones and urolithiasis. Crystalline material strongly reflects sound waves. This enables distinction of MSU crystals from less echogenic surrounding soft tissues.
Power Doppler or colour Doppler US is based on the Doppler effect, which consists of the shift of frequency of a sound beam reflected back to the source when it encounters a moving object. Doppler US detects movement of red blood cells in vessels. Power Doppler or colour Doppler US is a valuable tool for assessing hyperaemia of synovial tissue. Doppler US findings correlate closely with histopathological findings of vascularity68 and also with arthroscopic vessel scores.69 No such studies have been published in gouty arthritis to date.
Erosions are defined ultrasonographically as breaks in the hyperechoic outline of the bony cortex, seen in two perpendicular planes, following the Outcome Measures in Rheumatology.70 Examples of early gouty erosions detected by US but not seen on CR were included in our earlier reports.60 This is in agreement with studies by Rettenbacher et al71 and Wright et al72 who detected erosions three times more frequently by HRUS than by CR. We found a frequent association between the presence of the gouty tophus and bone erosions on HRUS. Erosions adjacent to tophaceous material were seen in 15 of 23 (65%) MTP joints and 1 of 4 (25%) MCP joints.72 73 As discussed above, gouty tophi are surrounded by an inflammatory reaction, a rim of macrophages, lymphocytes and large foreign body giant cells.19 These cells are part of the corona zone and form a well-defined compact zone which is demarcated from both the central crystalline deposit and the surrounding fibrovascular zone. This corona zone may explain the ultrasonographic in vivo finding of an anechoic rim surrounding tophi.74 In contrast to RA, synovial proliferation is only moderate in gouty arthritis and bony erosions can occur outside synovial joints. Sonographically,74 tophi and not invading synovial tissue, such as that seen in RA, are closely associated with bony erosions.
Ultrasongraphic studies have shown that persistent low-level inflammation is present in asymptomatic chronic tophaceous gout. Doppler signals were present in and around tophaceous deposits in more than half of patients with asymptomatic chronic gouty arthritis (figures 2 and 3A-D).3 Doppler signals were more often seen over the anechoic corona surrounding the tophi or invading tophi than over tissue that emanates from the synovial lining of the joints. This suggests that erosions were associated with tophaceous material and not with synovial tissue such as that seen in RA. In an MRI study of first MTP joints, evidence of chronic inflammation was seen in 63% of first MTP joints in the absence of acute attacks, which is supportive of our findings.73 This chronic inflammation surrounding tophi most probably contributes to erosion formation in gouty joints.

Orientation of ultrasound images.
{kind=link}
{kind=link}
{kind=link}
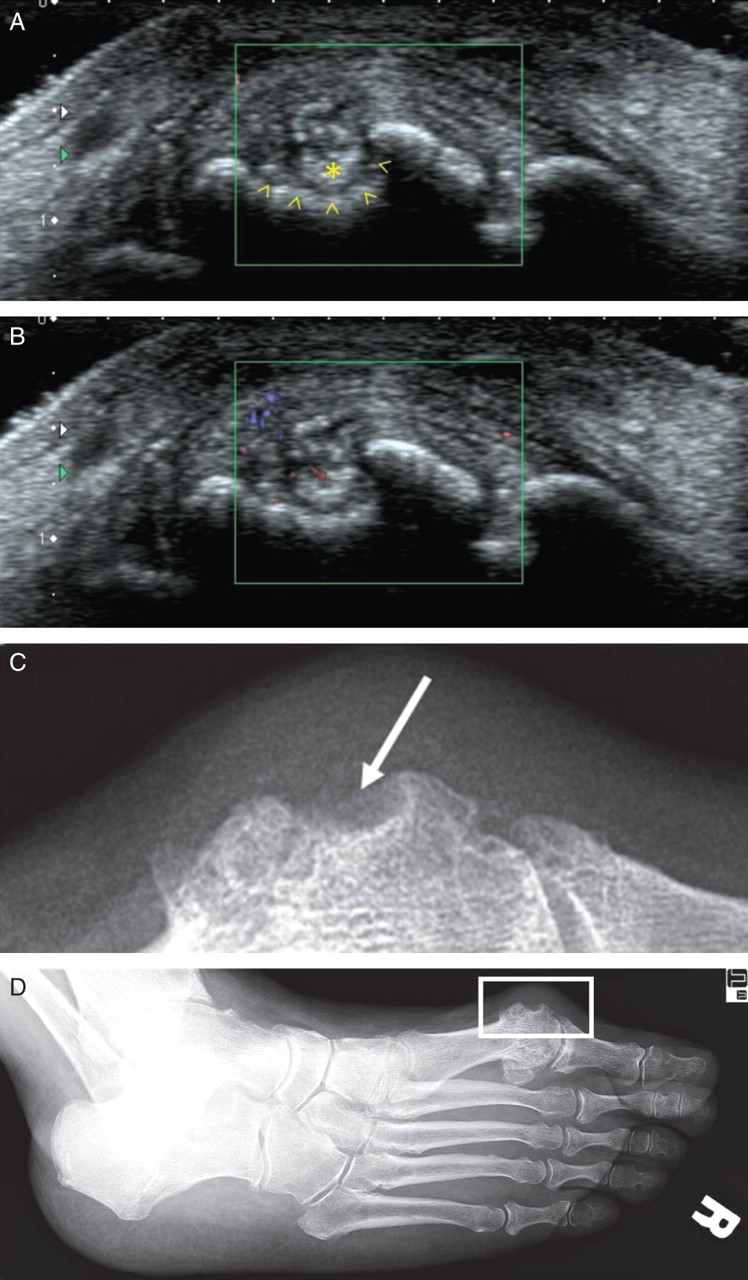
Comparison of conventional radiography and ultrasonographic images in a 65-year-old woman with recurrent episodes of monosodium urate crystal-proven gouty arthritis. She was asymptomatic at the time of study. Previously raised serum urate levels had normalised to 4.7 mg/dl. Acute phase reactants had normalised. High-resolution ultrasound with a transducer frequency of 18 MHz was used in images A and B. (A) Medial long axis view of first metatarsal head showing large erosion (open arrowheads) with invading hyperechoic tophus (asterisk). An anechoic zone is seen between hyperechoic tophus and hyperechoic bone. This frame is captured in diastole. (B) Frame captured in systole. Flow is seen adjacent to the tophus. (C) Section of conventional x-ray obtained on same day as ultrasound images (same orientation as images above). Suspicion of small erosion was raised (arrow). Tophi not well seen on conventional x-ray. (D) Original x-ray of same patient (same orientation as US images). Section of interest is framed.
Conclusions
In recent years there has been more insight into the processes underlying the development of bone erosions in gouty arthritis. The tophus eroding the underlying bone is pivotal in the development of bone erosions in gouty arthritis. MSU crystal deposition is associated with the presence of underlying OA. Osteoclasts and the RANK–RANKL pathway are important in mediating bone erosion formation in gouty arthritis.
Adequate urate lowering therapy is important in the reduction and resolution of tophi,75,–,77 thus possibly facilitating the regression and resolution of erosions in patients with gout.78
IL-1 has previously been implicated in bone destruction and erosions in inflammatory arthritis. It has recently become apparent that the inflammatory process in gouty arthritis is primarily driven by IL-1β. IL-1 blockers may allow us to probe the specific cellular and molecular pathophysiological mechanisms responsible for bone erosions in our patients. Persistent low-grade inflammation is frequently present in asymptomatic chronic tophaceous gouty arthritis. Thus, chronic anti-inflammatory therapy may need to be added to chronic urate-lowering therapy in patients with chronic tophaceous gouty arthritis.
References
Footnotes
-
Competing interests NS has received grant/research support from Novartis, is a consultant to Novartis and has been on the Advisory Boards of Novartis, Takeda, Savient, URL Pharma and EnzymeRx. RGT is a consultant to Novartis. Patent application: ‘Diagnosis of gout by ultrasound’ filed by the University of Medicine and Dentistry of New Jersey, 9/22/2005, US Patent and Trademark Application serial number 11/523,727.
-
Provenance and peer review Not commissioned; externally peer reviewed.