Article Text

Abstract
Objectives To determine the causes and predictors of mortality in systemic sclerosis (SSc).
Methods Patients with SSc (n=5860) fulfilling the American College of Rheumatology criteria and prospectively followed in the EULAR Scleroderma Trials and Research (EUSTAR) cohort were analysed. EUSTAR centres completed a structured questionnaire on cause of death and comorbidities. Kaplan–Meier and Cox proportional hazards models were used to analyse survival in SSc subgroups and to identify predictors of mortality.
Results Questionnaires were obtained on 234 of 284 fatalities. 55% of deaths were attributed directly to SSc and 41% to non-SSc causes; in 4% the cause of death was not assigned. Of the SSc-related deaths, 35% were attributed to pulmonary fibrosis, 26% to pulmonary arterial hypertension (PAH) and 26% to cardiac causes (mainly heart failure and arrhythmias). Among the non-SSc-related causes, infections (33%) and malignancies (31%) were followed by cardiovascular causes (29%). Of the non-SSc-related fatalities, 25% died of causes in which SSc-related complications may have participated (pneumonia, sepsis and gastrointestinal haemorrhage). Independent risk factors for mortality and their HR were: proteinuria (HR 3.34), the presence of PAH based on echocardiography (HR 2.02), pulmonary restriction (forced vital capacity below 80% of normal, HR 1.64), dyspnoea above New York Heart Association class II (HR 1.61), diffusing capacity of the lung (HR 1.20 per 10% decrease), patient age at onset of Raynaud's phenomenon (HR 1.30 per 10 years) and the modified Rodnan skin score (HR 1.20 per 10 score points).
Conclusion Disease-related causes, in particular pulmonary fibrosis, PAH and cardiac causes, accounted for the majority of deaths in SSc.
Statistics from Altmetric.com
Systemic sclerosis (SSc) is a multisystem disease with vascular, inflammatory and fibrotic components. The mortality of SSc is high.1,–,3 Several studies have suggested that the cause of death has changed over time, possibly because the natural history of SSc complications such as renal crisis and pulmonary arterial hypertension (PAH) are altered by pharmacological prevention and treatment.4 5 In addition to the temporal changes in the causes of SSc mortality, regional and centre-specific prevalences of organ involvement and survival have been noted.2 6
We therefore aimed to (1) obtain information on the cause of death, (2) the prevalence of comorbidities in those that died and (3) to identify independent predictors of death in SSc in the current era. In order to diminish regional bias, we assessed survival in the multinational EULAR Scleroderma Trial and Research (EUSTAR) cohort.7 The data gained are important for the appropriate planning of clinical trials because high-risk interventions may only be justified in patients with a high likelihood of an adverse outcome in the absence of treatment.
Methods
Data collection
The EUSTAR database was inaugurated in June 2004 and represents a multinational, prospective and open SSc cohort in which consecutive patients with scleroderma are included if they provide informed written consent. The structure of the minimal essential dataset (MEDS), which is collected in the EUSTAR database has been described previously.7 Follow-up visits are documented annually. SSc cases registered as dead up to April 2008 were analysed. The EUSTAR database contains a domain in which participating centres provide the date of death and assess whether the death was due to SSc itself, the treatment of SSc, or due to non-SSc-related causes.
For the purpose of this study, centres registering an SSc fatality were invited to fill out a standardised questionnaire. In the first section of this form, centres had to choose the single primary cause of death from a set of predefined categories including cardiovascular, respiratory, renal, infectious, neoplastic, gastrointestinal, suicidal and other causes. The centre was required to distinguish between the most important (primary) clinical problem and inevitable secondary terminal events. As an example, the centre was instructed to document pneumonia or PAH, rather than cardiac arrest.
In the second part of the questionnaire, the centres had to document any clinically significant comorbidity. In this part of the form, clinicians had an unlimited choice from a similar set of predefined comorbidities. Space for explanatory comments was also provided.
Three experienced rheumatologists evaluated the forms for completeness and plausibility. Disagreement was solved by consensus after queries with the centre.
Data analysis
Causes of death were analysed using standard descriptive statistics. Categorical variables were compared using χ2 statistics. MEDS data were used to determine risk factors for mortality. For this purpose, the survival data of SSc patients who had at least one annual visit after their inclusion in EUSTAR were analysed. Survival distribution functions in Kaplan–Meier plots were generated from MEDS parameters. MEDS parameters found to affect survival significantly in a first univariate analysis were then entered in a multivariate Cox proportional hazards model with a stepwise selection procedure in order to calculate independent predictors of mortality. The statistical analysis was performed with SAS version 9.2.
Results
A total of 5860 patients diagnosed with SSc according to the American College of Rheumatology criteria had been enrolled in the EUSTAR cohort.8 One hundred and forty-five centres in 28 European and six non-European countries had participated. Two hundred and eighty-four patients (5.2%) from 64 centres in 29 countries died after enrolment. Two hundred and twenty-nine deceased patients (80.6%) were women. The mean age at recruitment was 57 years. The total number of person-years of follow-up was 5268 years. The mean duration of follow-up was 0.9 years per person. Dead patients had been followed in the cohort for a mean period of 1.3 years (SD 1.1) after inclusion. The mean age at death was 61.7 years (SD 13.3 years). The annual mortality was 68 per 1000 person-years of follow-up.
Of the 284 deceased patients, we received 234 (82%) completed questionnaires from 45 centres in 19 European and four non-European countries. Fifty questionnaires were not returned; although these cases were excluded from the ‘causes of death analysis’, they were included in the calculation of predictors of death based on the MEDS data. When we compared the cases with documented cause of death with those without returned cause of death questionnaires, we did not find a significant difference of age at death, disease duration, gender, antibody status, proteinuria, modified Rodnan skin score (mRSS), diffusing capacity of the lung for carbon monoxide (DLCO), dyspnoea, the presence of PAH and pulmonary restriction (p>0.05 for all parameters). This finding supports the notion that the course of SSc was not more or less severe between the 234 patients in whom a questionnaire was available, compared with the 50 patients for whom we had no cause of death data.
Among the total of 284 dead patients, 54.6% had diffuse cutaneous (dc) SSc and 40.5% had limited cutaneous (lc) SSc, compared with 34.7% with dcSSc and 60.1% with lcSSc among the patients who were alive at the last follow-up (p<0.001). Among the 284 patients who died, the median SSc disease duration as estimated from the onset of Raynaud's phenomenon until death was 7.1 years for patients with dcSSc and 15.0 years for lcSSc; 47.9% of the patients who had died had serum autoantibodies against topoisomerase I (Scl70), and 20.8% had anticentromere antibodies (ACA). For comparison, these autoantibody frequencies among the survivors were 35.3% and 32.9%, respectively (p<0.001 for both). The median mRSS of the patients who died was 13, compared with the mRSS of nine among the survivors (p<0.001).
Primary causes of death
The majority of deaths (55%) were attributed to SSc directly (table 1).
Primary causes of death in 234 patients with SSc
Nineteen per cent of all SSc fatalities had died of pulmonary fibrosis and 14% of PAH. SSc-related myocardial causes (14%) were to a large part attributed to arrhythmia (6% of total deaths). Renal causes accounted for the death of 10 patients (4%), all due to renal crisis. Renal crisis was fatal in 16% of all patients experiencing renal crisis. Seven patients (3%) died of gastrointestinal-related causes.
In those having died from arrhythmia, no cardiomyopathy was noted. However, 47% of arrhythmia cases did have a history of PAH (71% of which was secondary to pulmonary fibrosis). Twenty-seven per cent had pulmonary fibrosis without PAH.
One of the five patients dying with right heart failure had borderline PAH. Two patients with right heart failure had pulmonary fibrosis without PAH and one patient had diastolic dysfunction. In these cases, death due to right heart failure was not considered as secondary to other factors. Unfortunately, neither biopsy nor autopsy data were available to confirm suspected cardiomyopathy.
Non-SSc-related causes accounted for 41% of all deaths. Infectious (13% of all deaths), neoplastic (13%) and cardiovascular causes (12%) scored almost equally. Pneumonia predominated among the infections (17 pneumonia cases among 31 fatalities from infections). Among the malignancies, non-small cell lung cancer was clearly most prevalent (11 cases among 30 malignancies).
Comorbidities
The non-SSc-related deaths documented in the second part of the questionnaire were then analysed for SSc-related comorbidities. At least 24 of the 96 patients (25%) who died of a non-SSc-related cause had SSc-related comorbidities that were judged to have significantly contributed to the non-SSc-related mortality (table 2).
SSc-related co-morbidities among patients deemed to have died from causes unrelated to SSc (sepsis, pneumonia and gastrointestinal haemorrhage)
Thirteen of the 17 patients who died from pneumonia also had considerable SSc-related risk factors, as judged by the presence of oesophageal reflux with or without documented aspiration, or significant immobility. Septicaemia in the context of chronic ulcers, immobility and contractures was also frequent (six of 14 fatalities due to septicaemia).
Nine of the 14 lung cancer deaths had concomitant pulmonary fibrosis. Pulmonary fibrosis was not, however, significantly more frequent in the lung cancer cases (64%) than in the total EUSTAR cohort (2363 patients with lung fibrosis, 40.3%, p=0.12).
Predictors of death
A total of 2940 patients had a baseline visit plus at least one additional follow-up; these were used to compare survival univariately in Kaplan–Meyer curves and to determine HR of mortality by multivariate Cox regression modelling. When comparing the clinical features between patients with no follow-up and those with a follow-up, we found no meaningful difference with respect to most key parameters.
The univariate analysis of all MEDS parameters with regard to their association with mortality showed that decreased survival was associated with more extensive skin involvement at baseline, as evidenced by the mRSS, in which the HR was 1.55 for mRSS 10 to less than 20, HR 2.14 for mRSS 20 to less than 30, and HR 4.31 for mRSS 30–40 (p<0.001), dcSSc subtype (vs lcSSc, HR 1.63, p<0.001) and the presence of digital ulcers (HR 1.61, p<0.001). Furthermore, increased mortality was associated with a higher age at the onset of Raynaud's phenomenon (1.22 for age 30 to <50 years, 2.48 for age 50 to <70 years, 3.80 for age >70 years, p<0.001), male gender (HR 1.61, p<0.002), the presence of Scl70 autoantibodies (compared with ACA, HR 1.59, p<0.002) and the duration of SSc (as measured by the onset of Raynaud's phenomenon at study inclusion (HR 1.47, p=0.004). At the cardiopulmonary level, the presence of PAH diagnosed by echocardiography (HR 2.42, p<0.001), the presence of pulmonary fibrosis on chest x-ray (HR 1.71, p<0.001), the finding of a forced vital capacity (FVC) below 80% of normal (HR 2.24, p<0.001), a reduced DLCO (HR 6.01 for DLCO <40% of normal, 4.16 for DLCO 40 to <60% of normal, HR 1.71 for DLCO 60 to <80% of normal p<0.001), a reduced left ventricular ejection fraction (HR 2.86, p<0.001), a New York Heart Association functional class III or IV for dyspnoea (HR 2.32, p<0.001), palpitations (HR 1.30, p<0.048) and arterial hypertension (HR 1.38, p=0.007) were all univariately associated with increased mortality. Finally, a history of renal crisis (HR 2.89, p<0.001), the presence of proteinuria (HR 3.09, p<0.001), elevated acute phase reactants (HR 1.79, p<0.001), elevated creatine kinase (HR 1.73, p<0.001) and muscle weakness (HR 1.55, p<0.001) were associated with decreased survival. Gastrointestinal manifestations in contrast (oesophageal, gastric or intestinal involvement) had no significant impact on the risk of dying in univariate analysis (p=0.93).
In the multivariate Cox proportional hazards model, independent risk factors for increased mortality were the presence of proteinuria on urine dipstick analysis, the presence of PAH, an impaired pulmonary compliance (FVC <80% of normal), the presence of dyspnoea on exertion, a reduced DLCO, an elevated age of SSc onset as estimated by the first manifestation of Raynaud's phenomenon and the mRSS. The magnitude of the HR of these independent predictors is shown in table 3.
Independent risk factors for reduced survival in SSc patients by Cox regression modelling
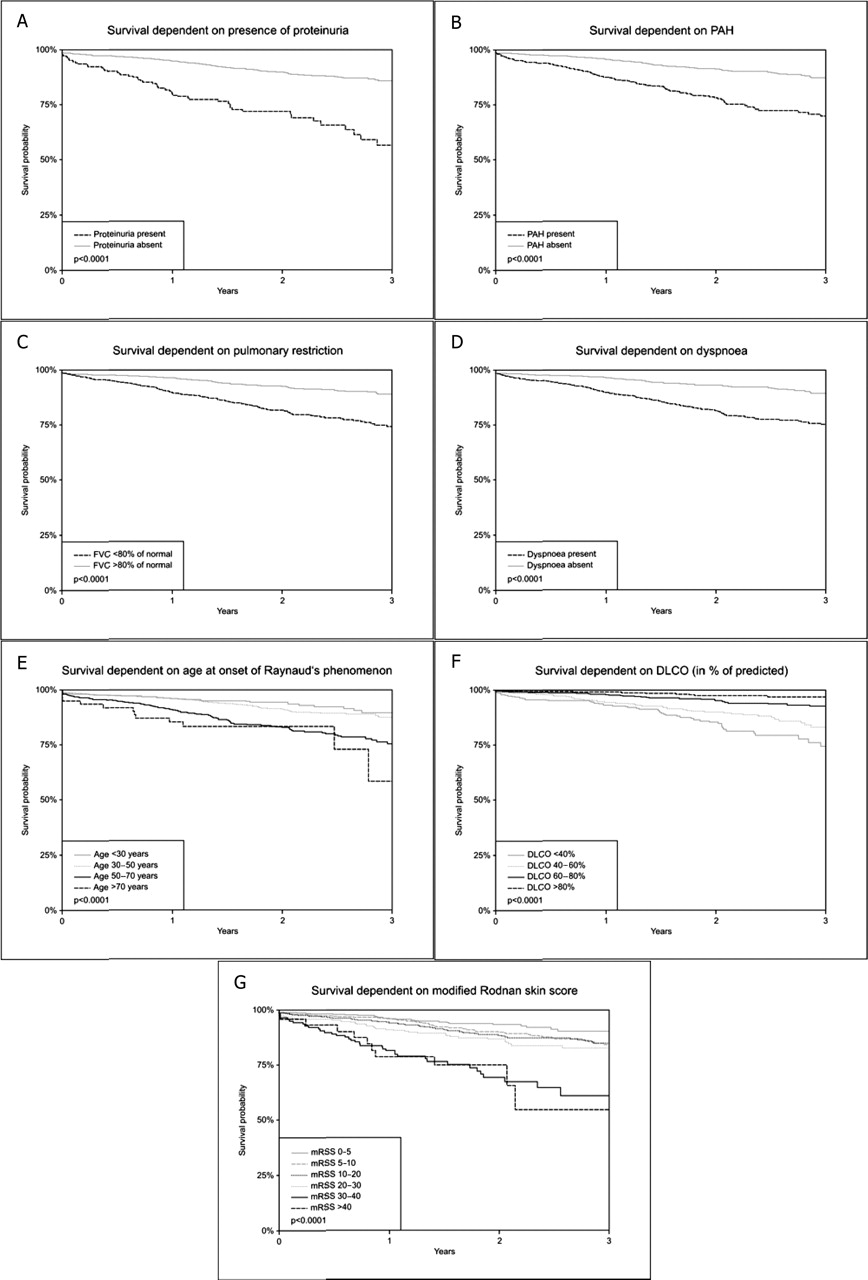
The Kaplan–Meier survival curves are shown in figure 1. Of note, SSc subtype, autoantibody status and gender did not remain independent ‘predictors’ of subsequent death, nor did elevated acute phase reactants, serum creatine kinase measurements and muscle weakness.
{kind=link}
Kaplan–Meier graphs for systemic sclerosis (SSc) survival on the basis of the follow-up data of 2940 patients of whom 384 had died. SSc mortality is plotted according to the presence or absence of proteinuria on dipstick analysis (A), pulmonary arterial hypertension (PAH) diagnosed by echocardiography (B), pulmonary restriction as indicated by a forced vital capacity (FVC) below 80% of normal (C), dyspnoea above the functional class II of the New York Heart Association (D), the patient's age at the onset of Raynaud's phenomenon (E), the diffusing capacity of the lung for carbon monoxide (DLCO) in percentage of normal (F) and the modified Rodnan skin score (mRSS). p Values refer to univariate comparisons (A–D) or tests for trend (E–G).
Of note, age was not automatically selected into the Cox proportional hazards model. When forcing age as a parameter into the model, the other determinants of mortality (PAH, proteinuria, mRSS, DLCO) practically remained unchanged, whereas the age at onset of Raynaud's phenomenon was eliminated. This suggests that age at onset of Raynaud's phenomenon and age itself are predictors that are highly correlated but that age at disease onset is the more important predictor.
Discussion
This study analysed the mortality of SSc patients in the prospective multinational EUSTAR cohort. The dataset comprised the MEDS data and a structured questionnaire.7 The results demonstrate a high prevalence of disease-related causes of death. The prevalence of SSc-related causes of mortality is similar, or in between the figures of other cohorts.3 5 Our findings underscore the high prevalence of pulmonary (interstitial lung disease and PAH), as well as myocardial causes.9 10
Since the introduction of ACE inhibitors, renal crisis appears to have become an increasingly less frequent terminal event.5 In our cohort, renal crisis accounted for 4% of the deaths, similar to the recent data from Pittsburgh.5 Except one individual, all patients dying from renal crisis were on an ACE inhibitor at the time of death (data not shown). Prednisone equivalents above 15 mg daily has been implicated in exacerbating scleroderma renal crisis, but in our study only one patient was on such treatment in the 3 months before the onset of renal crisis (data not shown).11
Among the non-SSc-related causes, infections, malignancies and cardiovascular incidents ranked highest. It should be noted, however, that a quarter of the patients with a non-SSc-related cause of death also had significant SSc-related comorbidity. If these deaths were adjudicated as ‘probably disease related’, the disease-related death toll would be as high as 65%.
Interestingly, an association between interstitial lung disease and lung cancer, especially non-small cell lung cancer has been noted.12,–,14 Nine of the 14 lung cancer cases in our cohort had pulmonary fibrosis, but the proportion of pulmonary fibrosis among the non-cancer EUSTAR patients did not differ statistically from that in our cancer cases. Although our analysis is limited by the absence of the smoking history, most lung tumours previously noted in patients with SSc were bronchioalveolar carcinomas or adenocarcinomas, malignancies that are not necessarily associated with cigarette smoking.13 Another population-based study has not confirmed an increased risk of lung cancer among SSc patients compared with the general population.15
Cardiovascular disease, especially premature atherosclerosis, had been implicated as the cause of early death in other inflammatory autoimmune diseases such as rheumatoid arthritis and systemic lupus erythematosus.16 17 In SSc, however, an increased prevalence of macroscopic coronary artery or cerebrovascular involvement has not been demonstrated.18 19 In SSc, it rather appears that cardiac microvessel involvement results in patchy replacement fibrosis, congestive cardiac failure and tachyarrhythmia rather than clinically overt myocardial infarction.20
Determining the exact cause of death poses problems. Patients may die at home away from diagnostic facilities, a circumstance that may cause disparities between death certificates and adjudicated expert judgement.21 Access to detailed clinical records has an influence on death certificates, as autopsies are only performed in the minority of cases.22 23 Comorbidities may be underestimated in their causal association and impact on mortality.3 24 Study results may also be biased by the coding of death certificates, rather than true disease patterns.25 Our study is also subject to these limitations. Although centres are asked to include SSc patients in EUSTAR consecutively and regardless of disease severity, we can not fully exclude the possibility that milder cases not under a rheumatologist's care may have been excluded. It is also unlikely that a high proportion of severe patients in the centres' care had died before entry into the EUSTAR registry, but it should be noted that in such cohorts, ‘dropouts’ at annual 12-month census could be due to death or ‘lost to follow-up’, leading to over-representation of survivors. Although such left-censorship bias is difficult to rule out, we found that the mean follow-up of fatalities was longer than the follow-up of the survivors. Nevertheless, annual mortality must be interpreted with caution, whereas the predictors of mortality are relatively robust. Finally, there may a centre-related patient selection bias, but the inclusion of a large number of centres contributing to MEDS is likely to reduce this potential confounder considerably.6
We evaluated independent predictors of mortality in terms of HR. Proteinuria was the strongest predictor of death. Similar to the finding of others1 proteinuria may be a marker of endothelial dysfunction. An independent influence of skin involvement on survival was previously determined using Cox regression analysis. dcSSc conferred a higher adverse risk compared with lcSSc but in our study skin involvement appeared to be better adjusted for by the more continuous mRSS model.3 24 26
Previous studies have delineated the importance of internal organ involvement.1 2 4 27 Our study also underlines the significant adverse effects of pulmonary restriction, reduced DLCO and PAH on mortality. The finding of PAH and pulmonary restriction as independent risk factors for mortality is also consistent with findings indicating a reduced survival in patients with interstitial lung-associated PAH compared with those with PAH alone.1 2 27,–,29
The presence of anti-topoisomerase I serum antibodies was previously found to be an independent risk factor for mortality.2 26 Topoisomerase I antibodies were also found to be an independent determinant of lung fibrosis in the EUSTAR cohort.7 The fact that we did not find autoantibodies to be an independent risk of death in the same cohort indicates that pulmonary risk was better predicted by the combination of DLCO, dyspnoea, FVC and PAH than by autoantibody status. In line with the previous analysis of SSc organ manifestations in EUSTAR, gender was not independently associated with mortality in the multivariate analysis.7 This also suggests that any effect of gender is better accounted for by the other variables.
In summary, our data indicate that SSc-related mortality is still high in the current era. Renal involvement, pulmonary complications, skin induration and age at SSc onset predict the excess mortality. The EUSTAR figures presented here are useful in estimating the number of patients that need to be included in clinical trials that investigate survival as the endpoint.
Acknowledgments
The authors would like to thank Dr Klaus Freivogel, Analytica Co, Lörrach, Germany for the statistical analysis in this paper.
References
Footnotes
-
Competing interests None.
-
Funding EUSTAR is supported by research grant from EULAR and is under the auspices of the Standing Committee for Clinical Affairs (ESCCA).
-
Patient consent Obtained.
-
Ethics approval All participating EUSTAR MEDS database centres have ethics committee approval.
-
Provenance and peer review Not commissioned; externally peer reviewed.