Article Text

Abstract
Objective: To evaluate a modified American College of Rheumatology 20 (mACR20) scoring system for patients with rheumatoid arthritis.
Methods: The data were evaluated from one study on patients with methotrexate (MTX)-naive early rheumatoid arthritis (ERA) and another study on patients with DMARD-refractory late rheumatoid arthritis (LRA). For mACR20 scoring, acute-phase reactant measurements were excluded, and 20% improvement from baseline was determined by 2 or 3 of the 4 remaining ACR components.
Results: For full joint counts with data from patients with ERA, marked differences favoured 25 mg etanercept (ETN) over 10 mg ETN by using the unmodified ACR20 (69% v 55%), the mACR203 of 4 (63% v 49%) and the mACR202 of 4 (72% v 58%). An assessment of 28 joints showed similar findings. In the trial on patients with LRA, considerably more patients in both ETN groups achieved a clinical response compared with placebo by using the ACR20, the mACR203 of 4 and the mACR202 of 4, whether using full or 28 joint counts. The mACR203 of 4 and full joint counts with data on patients with ERA showed a marked difference between the MTX and 10 mg ETN groups (63% v 49%), which was not observed with the ACR20.
Conclusion: Patterns of improvement indicated by mACR20 scores were consistent with standard ACR20 scores.
- ACR, American College of Rheumatology
- CRP, C reactive protein
- DAS, Disease Activity Score
- DMARD, disease-modifying antirheumatic drug
- ERA, early rheumatoid arthritis
- ESR, erythrocyte sedimentation rate
- ETN, etanercept
- LRA, late rheumatoid arthritis
- mACR20, modified American College of Rheumatology 20
- MTX, methotrexate
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- CRP, C reactive protein
- DAS, Disease Activity Score
- DMARD, disease-modifying antirheumatic drug
- ERA, early rheumatoid arthritis
- ESR, erythrocyte sedimentation rate
- ETN, etanercept
- LRA, late rheumatoid arthritis
- mACR20, modified American College of Rheumatology 20
- MTX, methotrexate
In efforts to increase uniformity in the assessment and reporting of outcomes in clinical trials on rheumatoid arthritis, researchers have proposed definitions of improvement based on sets of prespecified measures. Paulus et al1 proposed a composite index for measuring improvement in individual patients during trials on rheumatoid arthritis, and Felson et al2 proposed a core set of improvement measures. The American College of Rheumatology (ACR) composite score, which evaluates clinical improvement relative to an initial assessment, is a commonly accepted efficacy end point for clinical trials in patients with rheumatoid arthritis. The ACR20 denotes at least 20% improvement in tender and swollen joint counts and in three of the following end points: global assessment by patients, global assessment by doctors, erythrocyte sedimentation rate (ESR) or C reactive protein (CRP), patient’s pain Visual Analogue Scale and Health Assessment Questionnaire Score.3 The number of swollen joints, ESR and CRP correlate with radiographic progression of joint damage, whereas tender joint counts, as well as global assessments by doctors and patients, and patients’ reports of pain, are sensitive to change in clinical outcomes. Physical function, as assessed by the Health Assessment Questionnaire Score, is a potent predictor of the risk of disability in rheumatoid arthritis.4
In this report, we compare results derived using the standard ACR20 scoring method with two modified ACR20 (mACR20) scoring methods that exclude the acute-phase reactant criteria. This type of modified scoring method can be useful in measuring efficacy responses when acute phase reactant results are not readily available.
METHODS
The mACR20 scoring methods were evaluated using data from clinical trials on patients with methotrexate (MTX)-naive early rheumatoid arthritis (ERA) and disease-modifying antirheumatic drug (DMARD)-refractory late rheumatoid arthritis (LRA), who received 12 months and 6 months of treatment with etanercept (ETN), respectively. The institutional review boards and ethics committees of participating medical centres approved the protocols, and all subjects gave written, informed consent before any study-related procedures were carried out.
Patients with ERA were randomly assigned to receive MTX, 10 mg twice weekly ETN, or 25 mg twice weekly ETN.5 Entry was limited to MTX-naive adults with early aggressive rheumatoid arthritis for <3 years. DMARDs were discontinued at least 4 weeks before the study began. Patients were required to have a positive rheumatoid factor or at least three bone erosions on radiographs of the hands, wrists or feet; at least 10 swollen and 12 tender joints; and an increased ESR or CRP or morning stiffness that lasted at least 45 min.
In the trial on patients with LRA,6 adults with rheumatoid arthritis who previously had an inadequate response to at least one DMARD were randomly assigned to receive placebo, 10 mg twice weekly ETN, or 25 mg twice weekly ETN. If patients were receiving DMARDs, they were required to complete a DMARD washout period for at least 1 month before receiving the investigational product. At least 10 swollen and 12 tender joints were required, as well as an increased ESR or CRP or morning stiffness that lasted at least 45 min.
To evaluate the validity of the mACR methods, standard ACR20 scores, using 20% improvement in tender and swollen joints and 20% improvement in three of the five other scores (including ESR or CRP), were calculated with data from the trials on patients with ERA and LRA. These scores were compared with results obtained according to mACR20 methods; acute phase reactant measurements were excluded, and scores were calculated using 20% improvement in tender and swollen joints and 20% improvement from baseline based on either two or three of the four remaining criteria. Furthermore, ACR20 and mACR20 scores were calculated in two ways: using full joint counts (assessment of 71 joints; hip and cervical spine were evaluated only for tenderness; cervical spine and carpometacarpal joints were assessed in addition to the standard 66/68 joint count) and using assessment of 28 joints.
Consistent with the original study designs, ACR20 and mACR20 responses were calculated using last-observation-carried-forward for missing values for ERA and non-responder imputation for LRA. Statistical comparisons between treatment groups were made using the likelihood ratio χ2 test.
RESULTS
ACR20 and mACR20 scores for 632 patients with ERA (MTX, n = 217; 10 mg ETN, n = 208; 25 mg ETN, n = 207) and 234 patients with LRA (placebo, n = 80; 10 mg ETN, n = 76; 25 mg ETN, n = 78) were evaluated. Table 1 summarises the demographics of patients included in this assessment, which were well balanced between groups. In all groups, most patients were women and most were Caucasian; the mean age was about 50 years. In addition, the mean duration of rheumatoid arthritis across all groups was about 1 year. Most patients in all groups were receiving non-steroidal anti-inflammatory drugs at baseline. In the ERA group, 41%, 42% and 39% of patients used corticosteroids. In the LRA group, 58%, 66% and 81% of patients used corticosteroids (table 1).
Demographics of patients with ERA and LRA
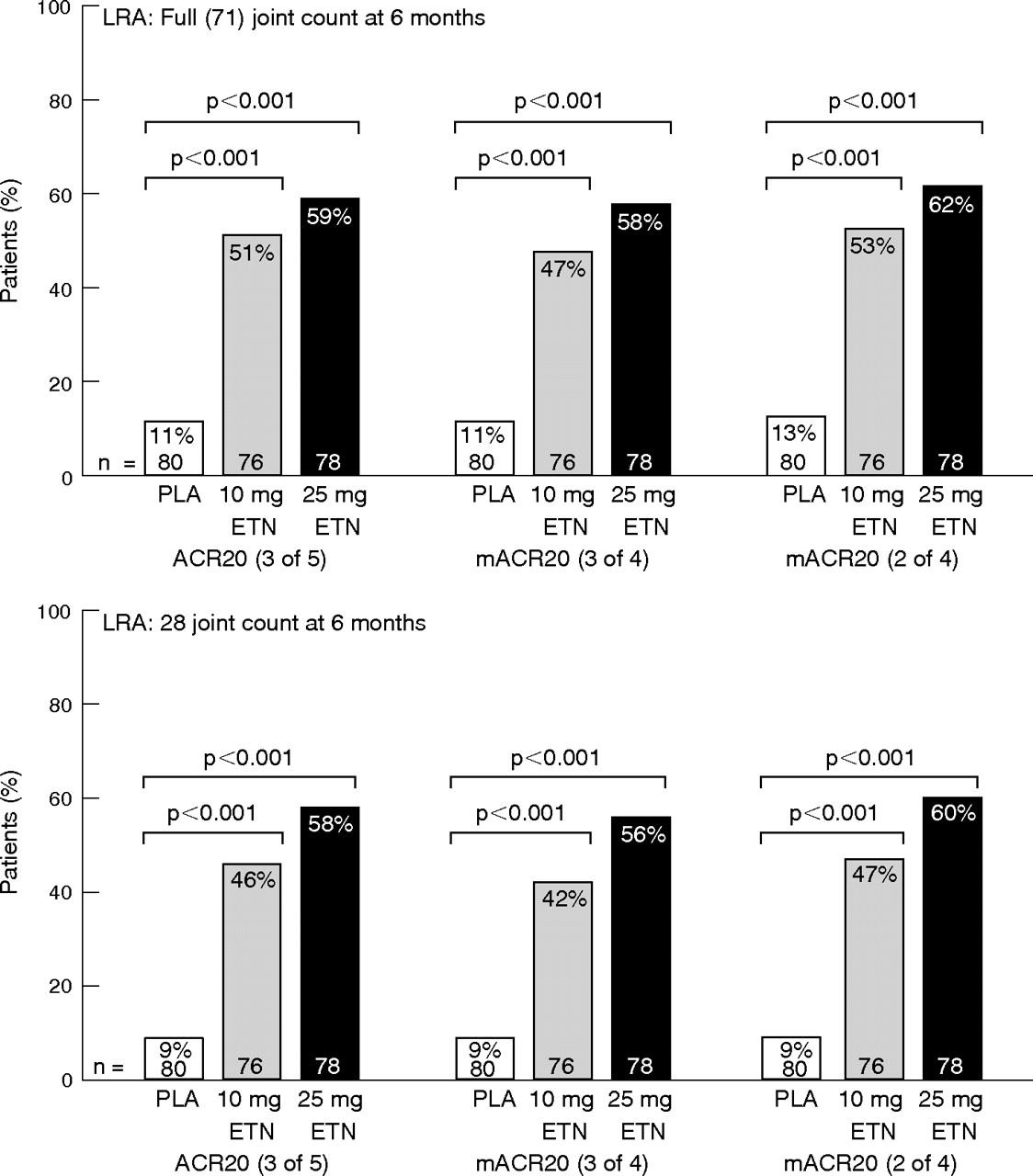
Statistically significant differences between the treatment groups were observed with the mACR20, similar to findings using the original ACR20 method. When using the full joint count and unmodified ACR20 in the ERA trial, considerably more patients in the 25 mg ETN group (69%) than in the 10 mg ETN group (55%) were ACR20 responders (fig 1). Similar differences between the two groups were seen with the mACR203 of 4 (49% v 63%) and the mACR202 of 4 (58% v 72%). In the LRA trial, considerably more patients in both ETN groups achieved a clinical response than those in the placebo group by using the ACR20, the mACR203 of 4 or the mACR202 of 4 (fig 2).
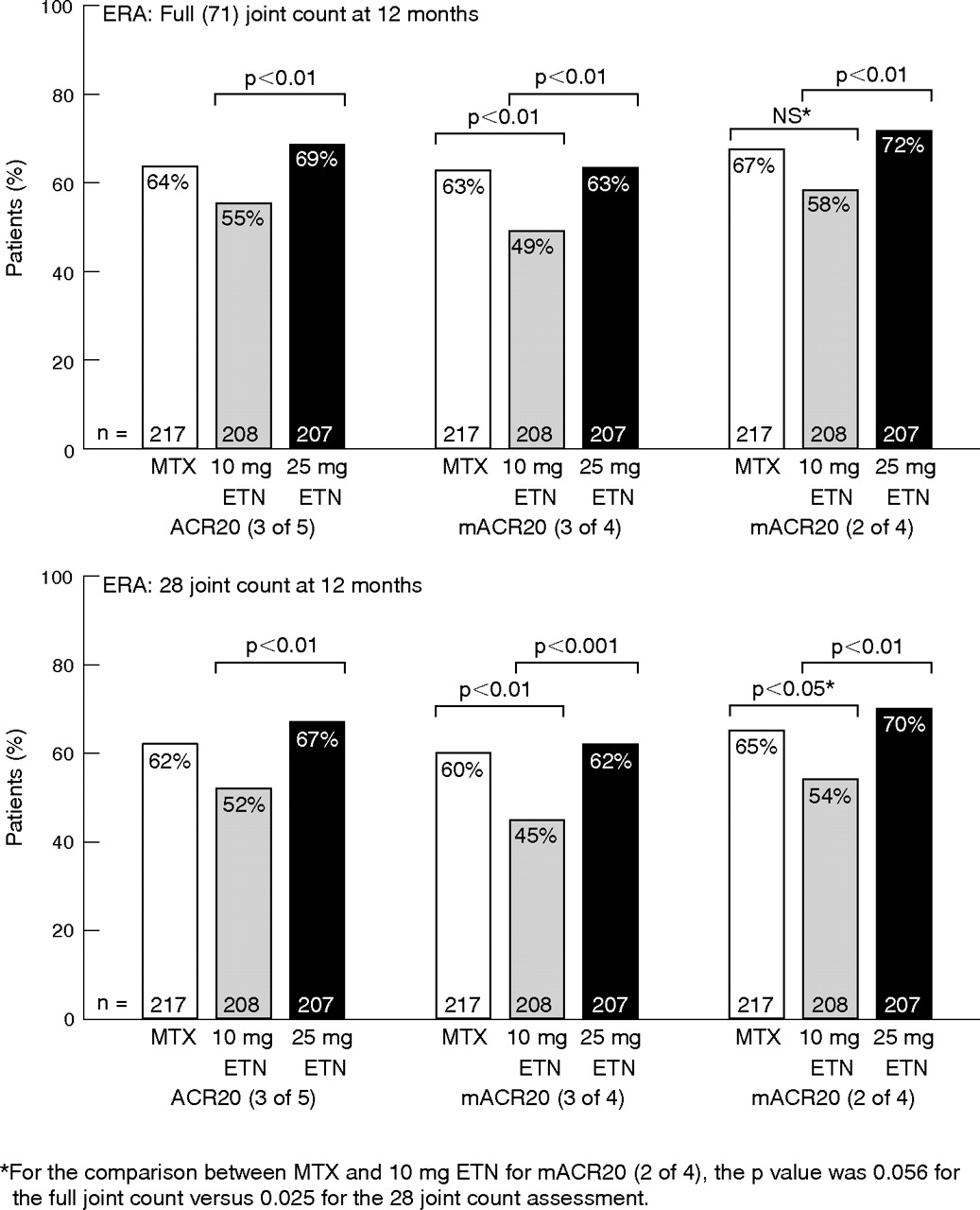
American College of Rheumatology (ACR) and modified American College of Rheumatology (mACR) Scores for patients with early rheumatoid arthritis (ERA). ETN, etanercept; MTX, methotrexate; NS, not significant.
{kind=link}
{kind=link}
American College of Rheumatology (ACR) Scores and modified American College of Rheumatology (mACR) Scores for late rheumatoid arthritis (LRA). ACR20, American College of Rheumatology 20; ETN, etanercept; PLA, placebo.
The only difference between the scoring systems was found in the trial on patients with ERA; a marked difference in ACR score was observed between the 10 mg ETN group and the MTX group (49% v 63%) by using the mACR203 of 4, which was not notable using the unmodified ACR20 (55% v 64%).
Results for the 28 joint count were similar to the full joint count for the trials on patients with ERA and LRA, and for the unmodified and modified ACR20 scoring systems. When using the 28 joint count and the unmodified ACR20 for assessment, marked differences were observed in the trial on patients with ERA between the proportion of ACR20 responders in the 10 mg ETN group (52%) and the 25 mg ETN group (67%). Similar differences between the two groups were seen using the mACR203 of 4 (45% v 62%) and the mACR202 of 4 (54% v 70%). In agreement with the full joint count results, in the trial on patients with LRA, considerably more patients in the ETN groups than those in the placebo group achieved a clinical response using the ACR20, the mACR203 of 4 or the mACR202 of 4.
DISCUSSION
Patterns of improvement indicated by mACR20 Scores were consistent with standard ACR20 Scores when comparing ERA and LRA patient groups. The mACR20 Scores can therefore provide reasonable assessments of clinical improvement in patients with rheumatoid arthritis. The mACR203 of 4 may be preferable as it is more conservative than the mACR202 of 4.
The mACR scoring system can be used to assess group efficacy responses when acute phase reactant values are not available, such as when evaluating patient populations from large databases (eg, observational registries); reviewers of these databases may not have access to laboratory reports. A modified Disease Activity Score would be of interest, but although Disease Activity Score (DAS) has been validated for interchanging ESR and CRP values, no validation has been carried out for omission of the ESR or CRP value.7 Notably, recent research does indicate that the Clinical Disease Activity Index, a composite score of clinical variables that does not include acute phase reactant measures, is a valid instrument for measuring disease activity in patients with rheumatoid arthritis.8
We recognise the usefulness and objectivity of ESR and CRP in assessing patients with rheumatoid arthritis, but this mACR scoring method can benefit clinicians and clinical trial investigators. Firstly, in daily practice, rheumatologists may have limited access to laboratory values on a timely basis. Depending on ambient temperature and delays in processing, ESR may be spuriously low if sent to an external reference laboratory for processing; it is optimal to run fresh specimens in as timely a manner as possible. Use of the mACR20 method will help doctors (who do not conduct ESR tests in their offices) quantify clinical improvement in their patients. Secondly, blinded clinical trials that include ACR20 assessment in the trial design may require an independent study site staff member to carry out ESRs. The additional resource and staffing expenses of having an independent staff member for this purpose may be avoided with the use of an mACR method.
As van Riel and van Gestel9 discuss, rheumatologists are continually striving to develop new measures or revise existing outcome measures to monitor changes in disease activity. Instruments such as the DAS scoring system7 are valuable in trial settings, but we recognise that real-world utility is also important. In an effort to increase the amount of decision-making data available to clinicians, we are studying whether our observations of clinical trial data can extend to the bedside. In contrast with the delayed reporting of ESR or CRP values, the mACR may supply a rapid result, available immediately at the patient’s bedside or during the visit to the clinic.
The mACR20 is shown to be consistent with the standard ACR20 scoring system, based on data from the ERA and LRA clinical trials. The mACR20 was able to discriminate between etanercept treatment as against either placebo or MTX. Although the removal of ESR or CRP does remove an objective criterion, this may be considered a more conservative approach because of the more stringent criteria needed to achieve an mACR20 response. Furthermore, a recently published manuscript validating the Clinical Disease Activity Index confirms that acute phase reactant data are not essential for the clinical assessment of rheumatoid arthritis disease activity.8
The results of this report indicate that mACR data can be useful for group comparisons of changes in disease status. It shares the advantages and disadvantages of the ACR20 method, which is useful for measuring relative change over time, as in the evaluation of treatment effects, but does not indicate the current status of rheumatoid arthritis inflammation (which is quantified by the DAS). Although the generalisability of these results remains to be determined, the mACR20 has effective utility for measuring changes in disease activity in patients with rheumatoid arthritis when acute phase reactant measures are not readily available.
Acknowledgments
We thank Julie Wang, DPM, for help in the preparation of this manuscript.
REFERENCES
Footnotes
-
Competing interests: These studies were funded by Amgen Inc, Thousand Oaks, California, USA. JAG is a member of Amgen’s Speakers Bureau and HP has received research grants and consulting fees from Amgen. JAG and HP are members of the RADIUS steering committee. BW and AX are employees of Amgen.