Article Text

Abstract
Background: The synovial tissue is a primary target of many inflammatory arthropathies, including psoriatic arthritis (PsA). Identification of proinflammatory molecules in the synovium may help to identify potentially therapeutic targets.
Objective: To investigate extensively the features of cell infiltration and expression of mediators of inflammation and joint destruction in the synovium of patients with PsA compared with patients with rheumatoid arthritis matched for disease duration and use of drugs.
Methods: Multiple synovial tissue biopsy specimens were obtained by arthroscopy from an inflamed joint in 19 patients with PsA (eight oligoarthritis, 11 polyarthritis) and 24 patients with rheumatoid arthritis. Biopsy specimens were analysed by immunohistochemistry to detect T cells, plasma cells, fibroblast-like synoviocytes, macrophages, proinflammatory cytokines, matrix metalloproteinases and tissue inhibitor metalloproteinase-1, adhesion molecules and vascular markers. Stained sections were evaluated by digital image analysis.
Results: The synovial infiltrate of patients with PsA and rheumatoid arthritis was comparable with regard to numbers of fibroblast-like synoviocytes and macrophages. T cell numbers were considerably lower in the synovium of patients with PsA. The number of plasma cells also tended to be lower in PsA. The expression of tumour necrosis factor alpha (TNFα), interleukin (IL) 1β, IL6 and IL18 was as high in PsA as in rheumatoid arthritis. The expression of matrix metalloproteinases, adhesion molecules and vascular markers was comparable for PsA and rheumatoid arthritis.
Conclusion: These data show increased proinflammatory cytokine expression in PsA synovium, comparable to results obtained for rheumatoid arthritis, and support the notion that, in addition to TNFα blockade, there may be a rationale for treatments directed at IL1β, IL6 and IL18.
- DMARD, disease-modifying antirheumatic drug
- HPF, high-power field
- HRP, horseradish peroxidase
- MMP, matrix metalloproteinase
- MTX, methotrexate
- PsA, psoriatic arthritis
- VEGF, vascular endothelial growth factor
- vWf, von Willebrand’s factor
Statistics from Altmetric.com
- DMARD, disease-modifying antirheumatic drug
- HPF, high-power field
- HRP, horseradish peroxidase
- MMP, matrix metalloproteinase
- MTX, methotrexate
- PsA, psoriatic arthritis
- VEGF, vascular endothelial growth factor
- vWf, von Willebrand’s factor
The synovial tissue is a primary target of inflammation in many inflammatory arthropathies, including psoriatic arthritis (PsA). PsA is a chronic, progressive disease in most patients1; a polyarticular onset of PsA is associated with a more destructive course.2 PsA has some typical entities such as the presence of dactylitis, enthesitis and involvement of distal interphalangeal joints. The diagnosis of PsA is in most cases easily made on the basis of the typical clinical signs and symptoms in combination with the presence of psoriatic lesions of skin or nails and often the absence of rheumatoid factor.
The clinical spectrum of PsA is heterogeneous, and the classification into five subgroups by Moll and Wright3 according to the phenotype appears to be partially unreliable in early arthritis cohorts, with almost half of the patients classified as polyarticular in the early stages being reclassified as oligoarticular after 2 years.4 Therefore, new classifying criteria are being developed.5 In addition, there is a need for better understanding of the pathogenetic mechanisms involved in PsA.
Identification of specific features of the PsA synovial cell infiltrate and mediators of inflammation and destruction may provide insight into the pathogenesis and identify potential therapeutic targets. In the past, a few studies have analysed the characteristics of the synovium with PsA compared with that with rheumatoid arthritis,6,7,8,9,10,11,12,13 with variable results. Several confounding factors may have influenced the results of some of the previous work, the most important probably being differences in the use of antirheumatic drugs and corticosteroids between both groups, which can have a major influence on the features of synovial inflammation in rheumatoid arthritis14–18 and PsA.19–23 Another confounding factor may be the selection of patients. Finally, computer-assisted image analysis of stained sections is more sensitive for detecting differences between groups than the semiquantitative evaluation that has been used in most previous studies. This is especially relevant for the evaluation of the expression of cytokines, adhesion molecules and matrix metalloproteinases (MMPs) per cell, which cannot be quantified reliably by conventional microscopic evaluation.24
Therefore, we designed a comparative cohort study to investigate the features of cell infiltration, expression of proinflammatory cytokines, adhesion molecules, MMPs and markers of angiogenesis in the synovium of patients with PsA compared with those with rheumatoid arthritis. Both groups were matched for disease duration and use of drug, and stained sections were analysed using sophisticated computer-assisted image analysis.25
MATERIALS AND METHODS
Patients
Nineteen patients with PsA were included in the study. Characteristic psoriatic skin disease was present in all patients, and the diagnosis of psoriasis was confirmed by a dermatologist. The patients had either an oligoarticular (n = 8) or a polyarticular (n = 11) pattern of joint involvement, with or without spinal involvement. One patient with polyarticular joint involvement was classified as mutilans type. The diagnosis of PsA was confirmed by two experienced rheumatologists (AWRvK and PPT). Twenty four patients with rheumatoid arthritis served as a control group. These patients fulfilled the 1987 ACR criteria for rheumatoid arthritis.26 The patients with rheumatoid arthritis were matched for disease duration and use of disease-modifying antirheumatic drugs (DMARDs). Patients were using either methotrexate, the most commonly used DMARD in daily practice for the treatment of both rheumatoid arthritis and PsA, or no DMARD at the time of inclusion.
Clinical data on disease activity were collected at the time of the biopsy, and consisted of a tender joint count, swollen joint count, patient’s visual analogue scale for disease activity and measurement of severe phase reactants in the blood. All patients gave their informed consent before inclusion.
Arthroscopy and biopsy handling
The arthroscopy was performed in the most accessible clinically inflamed large joint (knee, wrist or ankle joint) under local anaesthesia.27 To reduce sampling error, an average of 15 synovial biopsies was obtained at each arthroscopy. All samples were embedded en bloc in Tissue Tec OCT (Miles, Elkhart, Indiana, USA) and subsequently snap frozen. The frozen blocks were stored in liquid nitrogen until processed. Shortly before staining, 5-μm sections were cut and mounted on glass slides (Star Frost; Knittelgläser, Braunschweig, Germany). The glass slides were sealed and stored at −80°C until immunohistochemical analysis was performed in a single session.
Immunohistochemical staining
Serial sections were stained with the following mouse monoclonal antibodies (mAb): anti-CD3 (SK7, Becton-Dickinson, Mountain View, California, USA), anti-CD4 (SK3, Becton-Dickinson), anti-CD8 (DK25, Dako, Glostrup, Denmark), anti-CD38 (Leu-17, Becton-Dickinson), anti-CD55 (mAb67, Serotec, Oxford, UK), anti-CD68 (EBM11, Dako), anti-CD163 (M0794, Dako), anti-granzyme B (GrB-7, Monosan, Uden, The Netherlands), anti-intercellular adhesion molecule 1 (ICAM-1; CD54, BBIG-L1, R&D Systems Inc, Minneapolis, MN, USA), anti-vascular cell adhesion molecule 1 (VCAM-1; CD106, 51-10C9, Becton-Dickinson), anti-E-selectin (BB1G-E4, R&D Systems Europe, Abingdon, UK), anti-MMP1 (36665.111 R&D), anti-MMP3 (10D6, R&D), anti-MMP13 (181-15A12, Oncogene Research Products, Cambridge, Massachusets, USA), anti-tissue inhibitor metalloproteinase 1 (TIMP-1; 7-6C1, Oncogene Research Products), anti-von Willebrand’s factor (vWf; F8/86, Dako), and anti-αvβ3 (23C6, Santa Cruz Biotechnology, Santa Cruz, California, USA), anti-vascular endothelial growth factor (VEGF; C-1, Santa Cruz), anti-basic fibroblast growth factor (bFGF; clone 6, BD Transduction Laboratories, Lexington, Kentuky, USA). Staining was also performed with the following rabbit polyclonal antibodies: anti-tumour necrosis factor alpha (TNFα; IP-300, Genzyme, Cambridge, Massachusets, USA), anti-IL1β (LP-712, Genzyme), anti-IL6 (LP-716, Genzyme), and anti-IL18 (2D3B6, MD Biosciences, Zürich, Switzerland).
Endogenous peroxidase activity was inhibited using 0.1% sodium azide and 0.3% hydrogen peroxide in phosphate-buffered saline. Staining for cell markers and cytokines was performed as described previously.28 For control sections, the primary antibodies were omitted or irrelevant isotype-matched antibodies were applied. After a primary step of incubation with mAb, the bound antibody was detected according to a three-step immunoperoxidase method. Alkaline phosphatase-conjugated swine anti-rabbit antibodies (Dako), naphthol-AS-MX-phosphate, Fast Red Violet LB and levamizole (Sigma, St Louis, Missouri, USA) were used for detection of the rabbit polyclonal antibodies. Staining of MMPs and TIMP-1 was performed using biotinylated tyramide for amplification, as described previously.29 The primary antibodies were incubated for 60 min. Affinity-purified horseradish peroxidase (HRP)-conjugated goat anti-mouse (Dako) was added for 30 min, followed by subsequent incubation with biotinylated tyramide for 30 min and HRP-conjugated streptavidin for 30 min. HRP activity was detected using hydrogen peroxide as substrate and amino ethylcarbazole (AEC; Sigma) as dye. Slides were counterstained with Mayer’s haematoxylin (Merck, Darmstadt, Germany) and, after washing with distilled water, mounted in Kayser’s glycerol gelatin (Merck).
Microscopic analysis
The coded sections stained for CD3 (T lymphocytes), CD4 and CD8 lymphocytes, CD38 (plasma cells), CD55 (fibroblast-like synoviocytes), CD68 (macrophages), CD163 (subset of macrophages), granzyme B (cytotoxic cells), ICAM-1, VCAM-1, E-selectin, MMP1, MMP3, MMP13, TIMP1, vWf, αvβ3, VEGF, bFGF, TNFα, IL1β, IL6 and IL18 were analysed in a random order by computer-assisted image analysis, as described previously in detail.25 Briefly, three separate representative regions were chosen for evaluation of each section. Six consecutive high-power fields (HPFs) from each region were captured and digitised, resulting in a total of 18 HPFs per section. We have previously shown that this results in a representative measurement. The HPF images were analysed using the Qwin analysis system (Leica, Cambridge, UK). Additionally, vascularity was also separately scored using a semiquantitative vessel score to evaluate the vWf-stained sections as described previously in detail.30
Statistics
SPSS 11.5.1 for Windows was used for statistical analysis. The Mann–Whitney U test was used for comparison of the various markers in the synovial tissue of rheumatoid arthritis versus PsA. Results are expressed as mean (standard error of the mean (SEM)).
RESULTS
Clinical features
Table 1 shows the clinical and demographic data of the patients. The two groups were on average comparable with regard to disease duration and DMARD use. The patients with PsA had a mean disease duration of 10 years (range 2 months–25 years) and those with rheumatoid arthritis 9 years (range 3 months–25 years). In all, four (21%) patients with PsA and six (25%) patients with rheumatoid arthritis had a disease duration of <1 year. Also, 11 (58%) patients with PsA and 13 (54%) patients with rheumatoid arthritis were being treated with methotrexate (MTX) and two of these patients (one in each group) also used prednisone 10 mg/day. The other patients (eight with PsA (42%) and 11 with rheumatoid arthritis (46%)) were not being treated with a DMARD or corticosteroids. Thus, all patients were using either MTX or no DMARD at the time of synovial biopsy (other DMARDs were not permitted to prevent bias).
Clinical and demographic data of the patients
As expected, the rheumatoid arthritis group comprised more women (17 rheumatoid arthritis, 71%, and seven PsA, 37%) and more rheumatoid factor-positive patients (18 rheumatoid arthritis, 75%, and one PsA, 5%). Patients with rheumatoid arthritis had on average a higher swollen joint count (28 swollen joint count in rheumatoid arthritis: mean (SEM)14.5 (1.6); PsA 7.6 (1.8), p = 0.005) and CRP (rheumatoid arthritis 41.2 (7.9); PsA 20.5 (3.4) mg/l, p = 0.019). The fact that on average more joints were affected in the rheumatoid arthritis cohort may be reflected in the levels of acute-phase reactants.
Immunohistochemical features
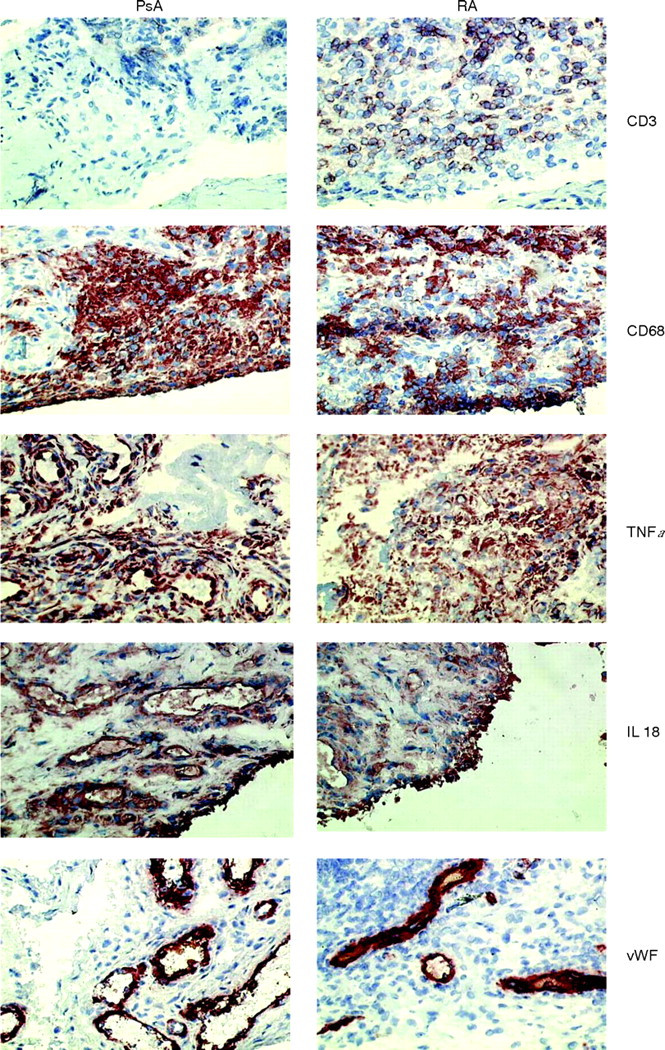
Table 2 and fig 1 show the results of the immunohistochemical analysis. All biopsy samples were taken from an actively inflamed joint, shown by pain and swelling, as stated before. The synovial infiltrate of patients with PsA and rheumatoid arthritis was comparable with regard to the number of fibroblast-like synoviocytes, intimal macrophages and sublining macrophages. T cell numbers were considerably lower in the synovium of patients with PsA. Consistent with this observation, both CD4 and CD8 T cells tended to be lower in PsA, but the differences did not reach statistical significance. It should be noted that CD4 is not only expressed by CD4+ T cells but may also be expressed by macrophages. The number of plasma cells also tended to be lower in PsA, although this difference did not reach statistical significance, possibly owing to the relatively small number of patients in this type of study. Interestingly, the expression of the proinflammatory cytokines TNFα, interleukin (IL)1β, IL6 and IL18 was as high in the synovium in PsA as in rheumatoid arthritis.
The cell infiltrate and expression of mediators of inflammation and joint degradation in synovial tissue of patients with PsA and rheumatoid arthritis

{kind=link}
Synovial immunohistology in patients with psoriatic arthritis (PsA) and rheumatoid arthritis (RA). Representative sections of staining with monoclonal antibodies for CD3, CD68, tumour necrosis factor (TNF) α, interleukin (IL) 18 and von Willebrand’s factor (vWf) are shown original (magnification ×400).
No differences between the groups were detected for MMP-1, MMP-3, MMP-13 and TIMP, or for the adhesion molecules ICAM-1, VCAM-1 and E-selectin. Furthermore, results between the two groups were comparable for the vascular markers VEGF, vWF, αvβ3 and bFGF. This was confirmed by semiquantitative vessel analysis on the vWf-stained sections; the scores were also comparable for rheumatoid arthritis and PsA.
When analysis was performed between patients with oligoarthritis and polyarthritis, no other significant differences or trends were detected (data not shown). Within the PsA group, additional analyses were performed: there were no differences between patients with oligoarthritis and polyarticular arthritis, except for IL1β, which was higher in the polyarticular group (p = 0.047); no major differences between MTX users and non-users were found, except for a higher MMP1 expression in the MTX users (p = 0.028).
DISCUSSION
This paper is the first to study the features of the synovial infiltrate of PsA in comparison with rheumatoid arthritis, taking into account disease duration and use of drug, using sophisticated digital image analysis. Interestingly, the only marked difference detected between the two groups in this study was a lower T cell count in the synovium with PsA. This is consistent with observations in two previous studies,11,13 and is perhaps remarkable because psoriasis and PsA are considered to be T cell-driven diseases. The lower number of T cells in the synovium with PsA does not mean, however, that these cells are not important in pathogenesis: a subset of specific T cells might be sufficient to promote the inflammatory process, and regulatory T cells may have anti-inflammatory effects. A trend towards a higher number of plasma cells in the synovium with rheumatoid arthritis was observed, but this difference was not significant. Only one earlier study10 showed a considerably higher number of plasma cells in the synovium in rheumatoid arthritis compared with that in spondyloarthropathy, but this could not be confirmed in a larger study by the same group.12 The most striking feature in both rheumatoid arthritis and PsA is the abundant overexpression of proinflammatory cytokines, especially TNFα, which was equally high in both groups. No other major differences between PsA and rheumatoid arthritis were found in synovial cell infiltrate, or in the expression of MMPs, adhesion molecules or vascularity.
A few previous studies have examined the features of the synovium in PsA with variable results.
Some studies suggested that the synovium in PsA is characterised by less pronounced lining layer in the hyperplasia and fewer monocytes/macrophages in the synovium,6,11 but neither finding could be confirmed in another study that analysed different forms of spondyloarthropathies together.10 One group found fewer T and B cells in the case of spondyloarthropathy synovium,10 but this was not found in the other studies.6,11 The fact that the synovial tissue was collected in different ways and the use of antirheumatic treatment may account for some of the observed differences.6,10,11
Interestingly, recent studies suggested that the presence of major histocompatibility complex–human cartilage gp39 peptide complexes in the synovium could be specific for rheumatoid arthritis12 and that the presence of a p53 mutation was higher in the case of rheumatoid arthritis than in the case of PsA synovium.13 These data suggest that the aetiology may be distinct between rheumatoid arthritis and PsA, although different processes may lead to the activation of common final pathways and similarities in the synovial infiltrate in established disease.
Increased vascularity has been reported in both psoriatic skin lesions and synovial tissue. The dermis of psoriatic skin has an abundance of dilated and tortuous blood vessels.31 This increased dermal vascularity is believed to be mediated by angiogenetic factors.32 Several authors have reported that the synovium in PsA is characterised by an increase in macroscopically tortuous blood vessels, and this is more pronounced—but not exclusive—in PsA than in rheumatoid arthritis.6–8,33 Consistent with the vascular abnormalities, overexpression of VEGF, which is involved in angiogenesis, has been reported in both psoriatic skin34 and synovial tissue in PsA.8,9 However, the increased vascularity in PsA compared with rheumatoid arthritis was not confirmed in all studies.11 In the present study, hypervascularity could be detected in both PsA and rheumatoid arthritis. There were trends toward increased numbers of blood vessels and expression of VEGF in PsA, but the difference from rheumatoid arthritis did not reach statistical significance, possibly because of the relatively small number of patients.
Blood vessels in psoriatic skin and PsA synovium express a variety of adhesion molecules such as ICAM-1, VCAM-1 and E-selectin.6,35 These adhesion molecules are involved in leucocyte adhesion and penetration through the endothelium. TNFα has been shown to promote the expression of adhesion molecules and angiogenesis,36 whereas blockade of TNFα resulted in a decrease in the expression of angiogenetic factors and adhesion molecules in psoriatic skin22 and the synovium in PsA.22,23,37 In this study, abundant expression of adhesion molecules was found equally in rheumatoid arthritis and PsA.
The degradation of cartilage and bone, resulting in structural (radiological) damage in inflammatory arthropathies, is believed to be mediated in part by MMPs. MMPs have been shown to be abundantly present in both rheumatoid arthritis29,38 and PsA.39 It has been suggested that high MMP expression is associated with more destructive disease.39,40 In the present study, there was high expression especially of MMP3, which was comparable for rheumatoid arthritis and PsA. This is in line with recent clinical studies, which showed that joint destruction in PsA is progressive in almost 50% of patients from an early arthritis clinic, showing radiological damage 2 years after first presentation,1 and that the degree of radiological damage in PsA is comparable to that in rheumatoid arthritis.41
Proinflammatory cytokines are important mediators of systemic and local inflammation, and abundant expression of IL1 and TNFα has been shown in psoriatic skin lesions,42 as well as in the synovial tissue of both patients with rheumatoid arthritis and PsA.11,39,43 The success of several TNFα blocking treatments in psoriasis and PsA44–49 and in rheumatoid arthritis50–53 has confirmed the importance of TNFα in these inflammatory diseases. In this study, there was equally high expression of TNFα in rheumatoid arthritis and PsA synovium. High expression of IL6, IL1β and, to a lesser extent, IL18 in rheumatoid arthritis and PsA has also been found in the present study. These data support the view that blockade of not only TNFα but also IL1β, IL6 and IL18 might be effective in PsA.
Consistent with previous reports, there were large differences in synovial infiltrate between individual patients within both groups. This may be caused by heterogeneity of what we diagnose clinically as being rheumatoid arthritis or PsA, and may point to the presence of certain disease subsets or pathophysiological differences, as has recently been suggested for rheumatoid arthritis.54
There were no clear-cut differences between patients who used MTX and those who did not, which is in line with a previous cross-sectional study.12 These data show that the lack of clinical response to MTX is reflected by persistent synovial inflammation.
In conclusion, although rheumatoid arthritis and PsA are clinically separate diseases, with a different aetiology, the present study showed mainly similarities in the synovial infiltrate of two well-matched cohorts of patients with rheumatoid arthritis and PsA. This may be explained by the fact that different pathophysiological processes may lead to the activation of final common pathways. This study shows increased proinflammatory cytokine production in PsA compared with results obtained in rheumatoid arthritis. These data support the view that, in addition to TNFα blockade, targeted treatments against other proinflammatory cytokines might be effective in PsA as well.
Acknowledgments
We thank Dr Maarten C Kraan, who performed several of the arthroscopies.
REFERENCES
Footnotes
-
Published Online First 25 May 2006
-
Competing interests: None.