Article Text

Abstract
Objective: To study serum levels of citrullinated protein/peptide antibodies (anti-CP) during up to 5 years’ follow up of patients with early rheumatoid arthritis (RA), and to relate serum levels to disease course and to treatments in clinical practice.
Methods: 279 patients with early RA were followed up with clinical investigations, radiographs, and measurement of anti-CP at baseline and after 3 months, 1, 2, 3, and 5 years.
Results: 160/279 (57.3%) patients were anti-CP positive at the first visit (mean 5 months after first symptoms). During follow up only 11/279 (3.9%) of the patients changed their anti-CP status. Anti-CP levels fell significantly during the first year, and this drop correlated with the extent of sulfasalazine treatment but not with other drugs or clinical indices. Anti-CP positive and negative patients had similar disease activities at baseline, but during follow up the anti-CP positive patients had worse clinical disease and greater radiological progression, despite at least equally intensive antirheumatic treatment.
Conclusions: Anti-CP are stable during the first 5 years of RA, suggesting that events before rather than after onset of clinical manifestations of disease determine this phenotype. The presence of anti-CP at diagnosis predicts a less favourable disease course and greater radiological progression despite antirheumatic treatment, but subsequent changes in antibody levels do not reflect changes in disease activity. Taken together, these observations suggest that anti-CP positive RA is a distinct clinical and pathophysiological entity.
- anti-CCP, cyclic citrullinated peptide antibodies
- anti-CP, citrullinated protein/peptide antibodies
- CRP, C reactive protein
- DAS28, 28 joint count Disease Activity Score
- DMARDs, disease modifying antirheumatic drugs
- ESR, erythrocyte sedimentation rate
- HAQ, Health Assessment Questionnaire
- IQR, interquartile range
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- VAS, visual analogue scale
- anti-citrulline peptide antibodies
- disease activity
- longitudinal study
- radiological progression
- rheumatoid arthritis
Statistics from Altmetric.com
- anti-CCP, cyclic citrullinated peptide antibodies
- anti-CP, citrullinated protein/peptide antibodies
- CRP, C reactive protein
- DAS28, 28 joint count Disease Activity Score
- DMARDs, disease modifying antirheumatic drugs
- ESR, erythrocyte sedimentation rate
- HAQ, Health Assessment Questionnaire
- IQR, interquartile range
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- VAS, visual analogue scale
- anti-citrulline peptide antibodies
- disease activity
- longitudinal study
- radiological progression
- rheumatoid arthritis
Rheumatoid arthritis (RA), as defined by classification criteria,1 probably represents various clinical phenotypes and pathophysiological entities, but identification of relevant subsets of RA has been limited to date. Rheumatoid factor (RF) positivity has been shown to predict worse disease outcome.2,3 However, RF phenotyping is marred by two important limitations. Firstly, patients with other diseases can be RF positive, yielding a limited specificity for RA, and secondly, RF is not a stable phenotype, as patients who are initially RF negative may become RF positive with time.
The demonstration that, compared with RF, antibodies against citrullinated proteins or peptides (for example, antibodies against cyclic citrullinated peptide (anti-CCP)) are more specific and similarly sensitive markers for RA4,5 has made the status of citrullinated protein/peptide antibody (anti-CP) an obvious subphenotype in RA. This view is strengthened by the demonstration that anti-CP may occur years before clinical RA, and that the occurrence of anti-CP in subjects who later develop RA is most common close to the onset of disease.6–,9 These findings have thus raised the question of whether anti-CP immunity is causally related to the onset of clinical manifestations of disease, or whether it represents an epiphenomenon.
Most studies to date have focused on the initial qualitative anti-CP status at study inclusion, and compared this status with clinical conditions at one or a few subsequent time points. In this study we used a quantitative and longitudinal approach with parallel investigations of antibody levels and clinical characteristics, including radiological data on multiple occasions. We particularly wanted to investigate whether the anti-CP phenotype was stable or fluctuated with time and whether it predicted clinical and radiological disease course and response to pharmacological treatment.
PATIENTS AND METHODS
Patients
Two hundred and seventy nine patients with RA from a prospective cohort of patients with early RA (<12 months of disease duration) at Karolinska University Hospital were included between January 1995 and October 2000. All patients fulfilled the 1987 American College of Rheumatology classification criteria for RA.1 Clinical evaluation included patients’ global assessment of disease activity and pain scores on visual analogue scales (VAS), functional disability using the Swedish version of the Stanford Health Assessment Questionnaire (HAQ),10 assessment of the number of swollen and tender joints and of disease activity, C reactive protein (CRP) and erythrocyte sedimentation rate (ESR), current drugs including steroids, non-steroidal anti-inflammatory drugs and disease modifying antirheumatic drugs (DMARDs). From the data obtained the 28 joint count Disease Activity Score (DAS28)11 was calculated. Clinical evaluation and serum sampling was performed at baseline, after 3 months, 1, 2, 3, and 5 years. For the calculation of cumulative DAS values and months of treatment with different DMARDs during the first 2 years, additional data were collected at 6, 9, 15, 18, and 21 months of follow up. All participants had given informed consent and the study was approved by the Northern Stockholm ethical committee. Clinical data were available from all patients at inclusion, 271 (97.1%) at 3 months, 244 (87.5%) at 1 year, 241 (86.4%) at 2 years, 232 (83.2%) at 3 years, and 151 (54.1%) at 5 years.
Anti-CP and RF
Anti-CP were analysed using the Immunoscan-RA Mark2 enzyme linked immunosorbent assay (ELISA; Eurodiagnostica, Malmö, Sweden). All samples yielding high values were further diluted to obtain definite values. A level above 25 U/ml was considered as positive, yielding a specificity of 97% when 99 healthy subjects were analysed. Of the initial 279 patients, serum samples were investigated at baseline, after 3 months and 1 year for 202 patients. The serum samples of the remaining 77 patients were also investigated at 2, 3, and 5 years after inclusion.
RF was determined by nephelometry and recorded at the first visit as a qualitative (positive/negative) variable.
Radiographs
A modification of the Larsen score that has proved to be advantageous for long term follow up assessment of RA12 was used. Identical radiographs of the hands and feet were scored without knowledge of the treatment, in pairs (hands and feet), and in chronological sequence applying the Larsen method.13 The scoring procedure was performed by an experienced investigator (MCW) and documented using the “X-RayRheumaCoach” software.14 In each case, 32 joints were scored. The aggregate Larsen score was modified slightly by excluding grade 1, so that the scale became 0–4.12 Thus, the maximum possible score was 160. The change in the Larsen score (ΔLarsen score) was calculated by subtracting the baseline Larsen score from the 2 year scores.
Statistics
Comparisons between groups were performed using Mann-Whitney’s U test for levels, or with the χ2 test for differences between proportions. Wilcoxon’s signed rank test was used to investigate changes in individual patients between different time points. Spearman’s correlation coefficient test was used to analyse the correlation between levels of anti-CP and continuous clinical indices, or between changes in anti-CP levels and changes in the clinical indices detailed in table 1⇓. In the latter analyses, differences and ratios in anti-CP between all time points for antibody analyses and baseline were compared with differences between various time points and baseline for the clinical variables listed in the patients’ section, resulting in 250 comparisons. Analysis of variance was used to dissect the relative prognostic importance of anti-CP status and RF status, where differences in clinical characteristics as compared with baseline were used as dependent variables. The Kruskal-Wallis test was used to investigate the impact of drug treatment on changes in anti-CP during the first year of investigation. No correction for mass significance was performed except when detailed in the text. Values of p<0.05 were considered significant.
Baseline characteristics of the 279 patients with RA included in the study
RESULTS
Qualitative and quantitative anti-CP status at baseline
At inclusion, 160/279 (57.3%) investigated patients had anti-CP antibodies >25 U/ml. The median anti-CP level among positive patients was 576 kU/l (range 27–16 995) and the mean (SD) value 1128 (2186) kU/l.
Qualitative changes in anti-CP status with time were rare. Only 11/279 (3.9%) patients had an altered status (three initially anti-CP negative patients became positive, and eight of the initially anti-CP positive patients lost demonstrable antibodies at any occasion during follow up). Most qualitative changes occurred in marginally positive samples. There was no association between appearance and disappearance of anti-CP and clinical variables, including drug treatment.
Table 1⇑ shows the baseline characteristics of patients. Besides the earlier described association between anti-CP and RF,4 the main difference between patients who were anti-CP positive or negative was age. The median age of anti-CP positive patients was 54.5 years, significantly different from the 60.0 years for anti-CP negative patients. No difference at inclusion was found for the other clinical or laboratory variables. Furthermore, there was no difference in the proportion of patients initially obtaining DMARD treatment. Of the 279 patients, 125 were initially treated with sulfasalazine, 64 with methotrexate, 22 with auranofin, 7 with antimalarial drugs, 3 with sodium aurothiomalate, and 12 with other drugs. Two patients were initially treated with a DMARD combination, and 44 patients did not receive any DMARD treatment.
Calculation of the cumulative use of DMARDs during the first two study years yielded 6696 individual months of treatment. Anti-CP positive patients had the highest percentage of treatment months with sulfasalazine alone (28.9% v 23.7%; p = 0.05) or with a combination of two (10.8% v 6.6%; p = 0.01) or three DMARDs (1.0% v 0%; p = 0.01). Anti-CP negative patients were more often treated with auranofin alone (17.2% v 9.9%; p = 0.01), and had a non-significantly higher percentage of treatment months without any DMARD treatment (14.6% v 11.6%). Methotrexate treatment did not differ between the groups. These results suggest that anti-CP positive patients were recognised as having higher disease activity and required more effective antirheumatic treatment than anti-CP negative patients.
Prognostic value of anti-CP status and quantitative anti-CP levels at baseline
Whereas no difference in disease activity between anti-CP positive and negative patients was present at baseline, the groups started to diverge from each other already after 3 months. Anti-CP positive patients had a higher disease activity measured by DAS28, a higher number of tender and swollen joints, and had a higher disease activity (as assessed using the patient’s and physicians’ global assessment) than anti-CP negative patients. All indices for clinical disease activity (presented in table 1⇑) diminished during the follow up period for the entire patient cohort, but the difference between anti-CP positive and negative patients became more obvious with time (fig 1⇓). A similar picture was also seen when the patients with RA were split according to the occurrence of RF at baseline, with RF positive patients showing the most active disease at all time points (data not shown).

Changes in mean clinical indices detailed in table 1⇑ for anti-CP positive (anti-CP+) and anti-CP negative (anti-CP−) patients treated separately. Statistical comparisons were performed between anti-CP positive and negative patients at the indicated time points. *p<0.05; **p<0.01; ***p<0.001.
No correlations were evident between the levels of anti-CP antibodies at baseline and disease activity indices at baseline. However, the strength of the calculated correlations between baseline anti-CP and clinical indices increased steadily with time from baseline until 5 years, especially for physicians’ assessment of disease activity and the swollen joint count, where the correlations between baseline anti-CP and present clinical indices gradually increased from non-significant at baseline to highly significant after 5 years (rs = 0.33, p<0.0001 for physicians’ assessment of disease activity, rs = 0.31, p = 0.0002 for swollen joint count; data not shown). Comparisons between changes in the actual levels of anti-CP and changes in clinical measures created a number of weakly significant correlations, all of which (except for a drop in CRP between baseline and 1 year and a corresponding drop in anti-CP levels) were no longer apparent after Bonferroni correction (data not included).
Anti-CP positivity predicts greater radiological progression
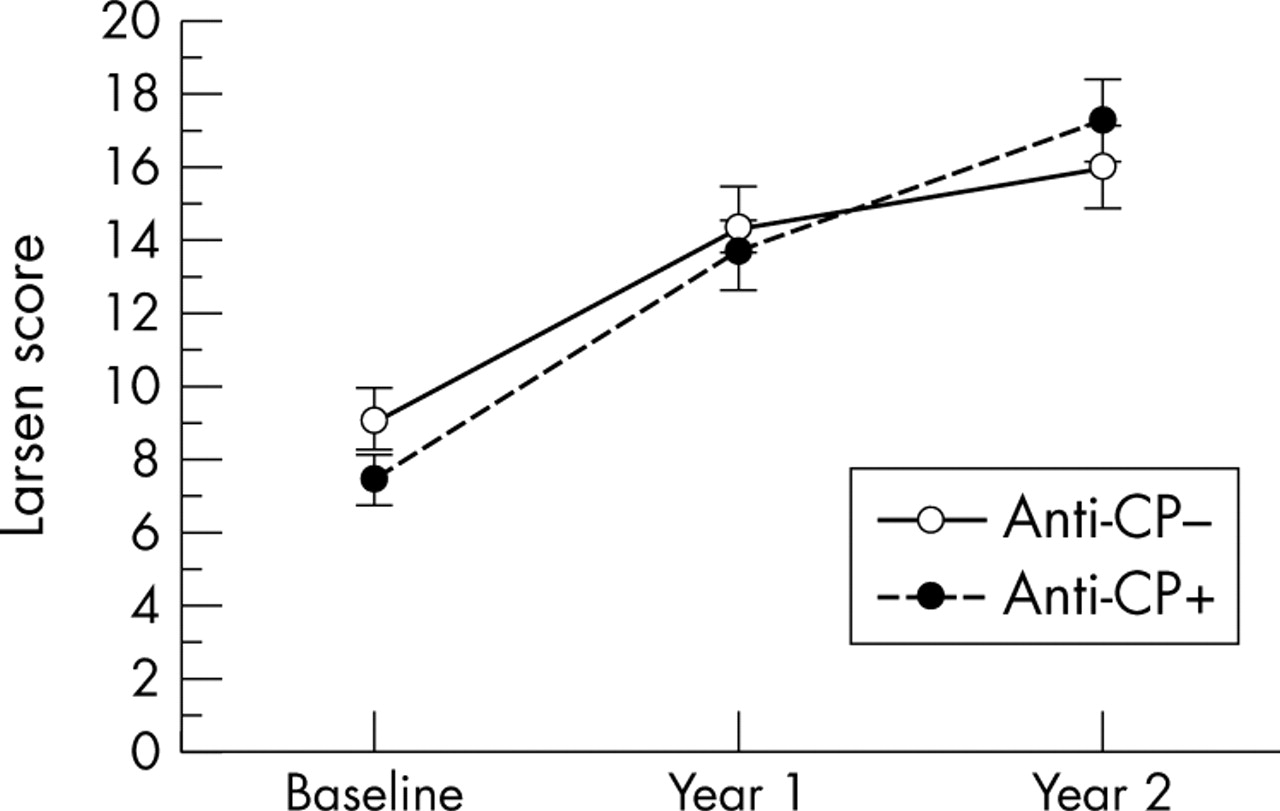
The mean (SD) baseline Larsen score for the 279 investigated patients was 7.9 (9.1) (median 4. 5; interquartile range (IQR) 1.0–12.1) and increased to 13.7 (12.0) (median 10.5; IQR 4.0–20.3) after 1 year, and to 16.6 (13.3) (median 14.0; IQR 6.0–24.0) after 2 years of disease. When the anti-CP positive and negative groups were investigated separately, baseline Larsen scores were 7.5 (8.8) (median 4.0; IQR 1.0–9.9) and 9.1 (9.2) (median 5.0; IQR 1.8–13.8), respectively, and not statistically different. The two groups differed in the degree of radiographic progression during the next 2 years: anti-CP positive patients had a greater ΔLarsen score between baseline and year 2 than anti-CP negative patients (mean (SEM) 9.7 (7.1) v 6.9 (5.7); p = 0.01; fig 2⇓). Similar results were seen when the patients were split according to RF status at baseline, with RF positive patients showing the greater radiological progression (data not shown).

Changes in mean Larsen score (SEM) among anti-CP negative and anti-CP positive patients separately.
Biphasic appearance of anti-CP levels during 5 years of follow up
The levels of anti-CP declined rapidly between inclusion and 1 year. Later, these levels increased, showing a significant rise between 3 months, 1 and 2 years, on the one hand, and 5 years, on the other (fig 3⇓).
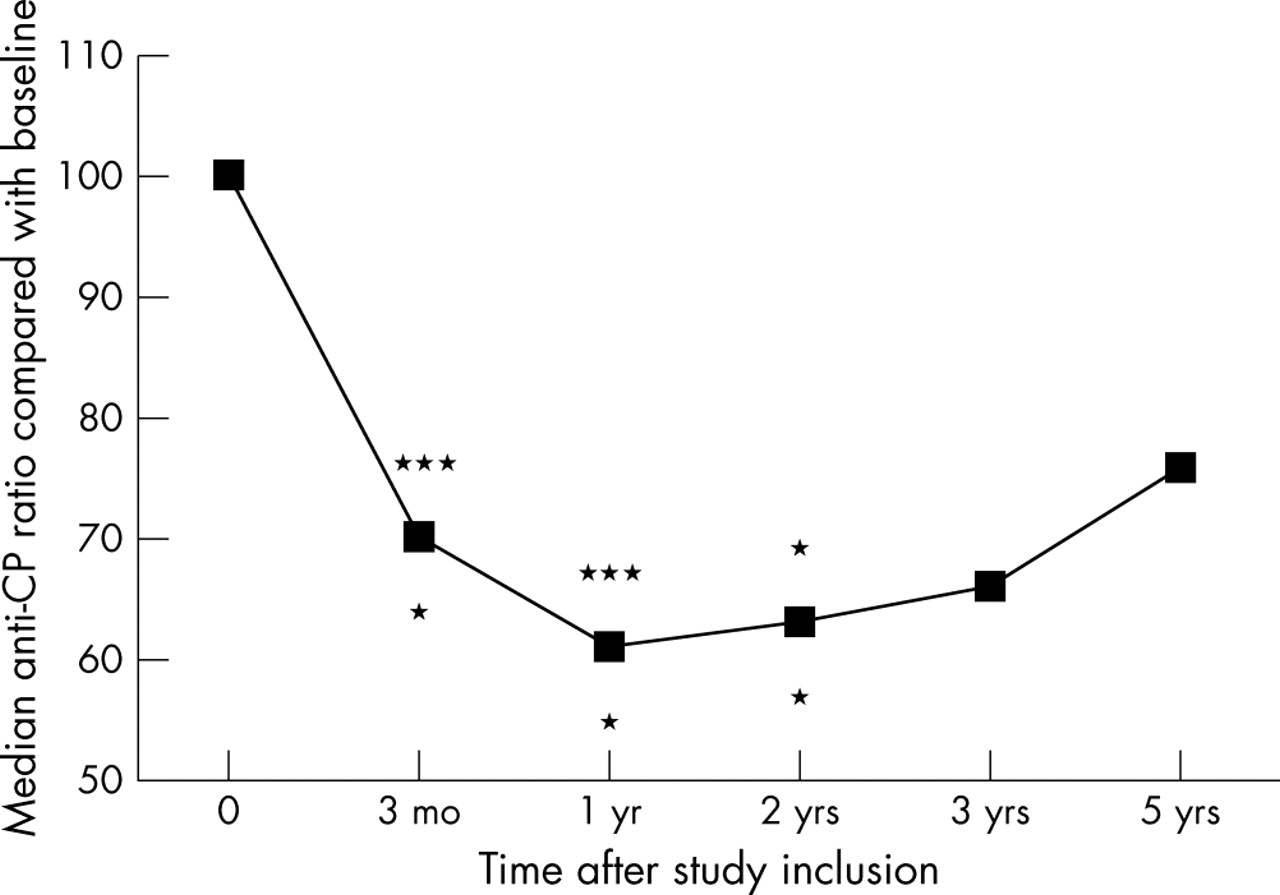
Percentage change in median anti-CP antibody levels among the anti-CP positive patients of the subgroup of 77 patients with RA for whom serum samples were obtained at baseline and after 3 months, 1, 2, 3, and 5 years, respectively. Paired statistical comparisons were performed between baseline and the indicated time points (asterisks above the graph; all differences denoting decreased ratios over time) and between various time points and 5 years (asterisks below the graph, all differences denoting increased ratios over time). *p<0.05; ***p<0.001. The same highly significant drop in anti-CP levels was also found between baseline and 3 months and 1 year, respectively, when the whole group of 279 patients was investigated.
Relationship between DMARD treatment and changes in serum anti-CP levels
The decrease in anti-CP levels during the first year was dose dependently associated with the extent of sulfasalazine treatment during the same period (p = 0.009; fig 4A⇓). No other DMARD showed such a correlation; patients treated with methotrexate instead had a non-significant increase in anti-CP values in comparison with baseline (fig 4B⇓). No correlation between the use of peroral steroids or non-steroidal anti-inflammatory drugs and changes in anti-CP levels was found. The late increase in anti-CP did not correlate with changes in any clinical variables or drug treatment during the same period.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in anti-CP levels during the first year as a function of treatment with (A) sulfasalazine and (B) methotrexate. “Never” indicates that the patient had not had the drug prescribed at any time point during the period, and “partly” that the patient had the drug prescribed for at least 3 months but not for the whole year. “Entire period” indicates that the drug was prescribed at the baseline visit with continuous treatment at 3, 6, and 9 month visits. On the ordinate the ratio between the anti-CP levels at 1 year and baseline is depicted. A few patients who increased more than 100% during the study period have been omitted from the figure but are included in the statistical calculations. Horizontal bars indicate median ratios for the corresponding groups. Only anti-CP positive patients have been included.
Relationship between baseline anti-CP and RF
To distinguish the prognostic effects of baseline anti-CP from those of RF, we performed an analysis of variance with changes (between baseline, on the one hand, and 3 months, 1, 2, 3, and 5 years, on the other) in the clinical indices in table 1⇑ as dependent variables. RF could only be distinguished as an independent variable for the change in DAS between inclusion and 2 years (p = 0.0041), whereas anti-CP was an independent variable for the change in swollen joint count between inclusion and 1 year (p = 0.048) and 3 years (p = 0.035), respectively. The prognostic effect of baseline RF and baseline anti-CP could not be separated in any other comparison.
When instead the 102 RF negative patients (including 12 anti-CP positive patients) were investigated separately, anti-CP antibody status at inclusion showed a predictive value in parallel to, but weaker than, the findings in fig 1⇑ for the total cohort, especially for the swollen joint count (data not included).
DISCUSSION
We have investigated at what time points after diagnosis any clinical differences between anti-CP positive and negative patients would be manifest. By serial quantitative measurements of anti-CP and parallel clinical and radiological investigations we wanted to explore the significance of anti-CP levels and to examine whether changes in antibody levels would predict, parallel, or follow changes in clinical variables, or relate to preceding or synchronous antirheumatic treatment.
We provide data in newly diagnosed RA, showing that very few patients change their anti-CP antibody status over time over a 1–5 year period. The study also confirms previous reports of the prognostic value of these antibodies.15–,19 Finally, new data are presented that demonstrate that changes in levels of anti-CP do not reflect disease activity, but may instead depend on pharmacological treatment.
In our study we observed no difference in clinical variables, except age, between anti-CP positive and negative patients at the time of diagnosis. Thereafter, clinical variables showed a gradually increasing difference between the anti-CP positive and negative patients, although it should be kept in mind that clinical data were only obtained from 151/279 (54.1%) patients after 5 years. In all comparisons for which the subgroups differed, anti-CP positive patients had the least favourable outcome. Likewise, patients who presented with anti-CP at baseline showed a significantly larger increase in radiological damage during the first 2 years of disease. In other words, the effect of antirheumatic treatment on both the clinical course and on radiographic progression was less impressive for the anti-CP positive patients than for the anti-CP negative patients. The anti-CP positive patients were significantly younger than the anti-CP negative patients. Because older age at onset of RA is associated with more severe disease outcome20 we believe that this age difference cannot explain the observed differences in clinical presentation.
The small number of qualitative changes in anti-CP status is of interest from a pathogenic perspective. There is now firm evidence that anti-CP can develop years before the onset of disease and that they occur before the onset of clinical symptoms in a significant proportion of patients with RA.6–,9 The fact that only few patients develop anti-CP after onset of disease is a strong indication that anti-CP immunity is associated with events causing RA, rather than a consequence of already existing disease. The stability of the anti-CP phenotype has also been observed in a recent study.21 Pathogenetic investigations of anti-CP immunity should therefore concentrate on events occurring before disease onset.
We determined no relationship between changes in antibody levels and changes in disease activity. However, correlation with quantitative anti-CP levels at baseline increased steadily over time for physicians’ assessment of disease activity and swollen/tender joint counts, being highest at 5 years. Similar data were produced for radiological progression over the first 2 years. These data imply that the prognostic importance of quantitative anti-CP levels at baseline may increase with time and indicate that follow up studies in longstanding RA are warranted. They also indicate that the immunological events leading to quantitatively different anti-CP levels at the time of development of overt RA are associated with the subsequent development of disease with varying inflammatory responses and disease severity over years to come.
Use of sulfasalazine, but not other DMARDs, was dose dependently associated with decreased anti-CP serum levels during the first year. Sulfasalazine and its metabolite 5-aminosalicylic acid have both been shown to suppress secretion of IgG, IgA, and IgM in vitro.22 Sulfasalazine treatment has also been shown to decrease IgG and IgA production in vivo.23,24 Taken together, it appears that sulfasalazine can down regulate antibody responses in RA. Sulfasalazine, but not other DMARDs, is associated with a decrease in anti-CP levels, indicating that it may have more profound effects on humoral immunity than other DMARDs.
In conclusion, the stability of anti-CP status and the failure of efficient treatment to eliminate these antibodies from serum strengthens the notion that anti-CP positive RA may differ from anti-CP negative RA in several important aspects, and that these two subgroups thus should be evaluated separately in future studies of both aetiology and treatment.
Acknowledgments
We thank Siv Roberg and Eva Jemseby for excellent technical assistance, colleagues at Karolinska University Hospital for collection of clinical data, and Dr R A Harris for linguistic advice.
The work was supported by funds from the Swedish Research Council, the Swedish Rheumatism Association, King Gustaf V’s 80-year Foundation, and the insurance company AFA.
REFERENCES
Footnotes
Published Online First 20 April 2005
Competing interests: none declared.
J Rönnelid and M C Wick contribute equally to this work.