Article Text

Abstract
Objective: To examine the efficacy and safety of infliximab combined with methotrexate compared with methotrexate alone in the treatment of ankylosing spondylitis (AS) using MRI and DXA to monitor its impact on bone.
Methods: In this single centre study 42 subjects with active AS were treated with methotrexate and were randomly assigned, in a ratio of 2:1, to receive five infusions of either 5 mg/kg infliximab or placebo over 30 weeks. The primary outcome was improvement in disease activity as shown by the BASDAI at week 30. MRI was used to assess the effect of treatments on sacroiliac and spinal enthesitis/osteitis and DXA to monitor bone mineral density.
Results: Both therapeutic agents were well tolerated with no dropouts due to adverse events. A significantly greater improvement in mean BASDAI score was seen in the infliximab arm at week 10 (p = 0.017) than in the placebo arm, but this was not maintained by week 30 (p = 0.195), 8 weeks after the last infusion, at which stage disease flares were reported by some subjects. MRI showed that the mean number of lesions resolving for each subject from week 0 to week 30 was significantly greater in the combination group than in the methotrexate monotherapy group (p = 0.016).
Conclusions: Infliximab in combination with methotrexate was a safe and efficacious treatment in AS over 6 months and was associated with significant regression in enthesitis/osteitis as determined by MRI. However, disease flares were reported 8 weeks after the last infusion, indicating that addition of methotrexate failed to extend the infliximab dosing interval.
- ANA, antinuclear antibodies
- ANCOVA, analysis of covariance
- AS, ankylosing spondylitis
- ASAS, ASsessments in Ankylosing Spondylitis
- ASQoL, Ankylosing Spondylitis Quality of Life Index
- BASDAI, Bath Ankylosing Spondylitis Disease Activity Index
- BASFI, Bath Ankylosing Spondylitis Functional Index
- BMD, bone mineral density
- CI, confidence interval
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- DXA, dual energy x ray absorptiometry
- FOV, field of view
- FS, fat suppressed
- MRI, magnetic resonance imaging
- NSAIDs, non-steroidal anti-inflammatory drugs
- RA, rheumatoid arthritis
- SIJ, sacroiliac joint
- TE, time to echo
- TNF, tumour necrosis factor
- TR, repetition time
- VAS, visual analogue scale
- ankylosing spondylitis
- infliximab
- methotrexate
- imaging
Statistics from Altmetric.com
- ANA, antinuclear antibodies
- ANCOVA, analysis of covariance
- AS, ankylosing spondylitis
- ASAS, ASsessments in Ankylosing Spondylitis
- ASQoL, Ankylosing Spondylitis Quality of Life Index
- BASDAI, Bath Ankylosing Spondylitis Disease Activity Index
- BASFI, Bath Ankylosing Spondylitis Functional Index
- BMD, bone mineral density
- CI, confidence interval
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- DXA, dual energy x ray absorptiometry
- FOV, field of view
- FS, fat suppressed
- MRI, magnetic resonance imaging
- NSAIDs, non-steroidal anti-inflammatory drugs
- RA, rheumatoid arthritis
- SIJ, sacroiliac joint
- TE, time to echo
- TNF, tumour necrosis factor
- TR, repetition time
- VAS, visual analogue scale
Ankylosing spondylitis (AS) is a chronic inflammatory disorder that predominantly affects young adults. Conventional therapeutic options for AS, unlike rheumatoid arthritis (RA), fail to prevent disease progression, with a substantial proportion of subjects (40%) eventually developing severe spinal restriction.1 Furthermore, AS carries substantial morbidity and reduced quality of life similar to that seen in RA.2 The short term management of AS has been transformed by the introduction of tumour necrosis factor (TNF) α blockers, with data from double blind and open label studies using the monoclonal antibody infliximab or the Fc-TNFR fusion protein etanercept showing efficacy3–,5 similar to that seen in subjects with RA.
In RA, methotrexate is used as the anchor drug for combination treatment, both with other disease modifying antirheumatic drugs (DMARDs) and with biological treatments.6 However, no data have demonstrated the efficacy of methotrexate as monotherapy in AS, apart from some preliminary results in small open label trials.7,8 Although infliximab generally is well tolerated, hypersensitivity and infusion related reactions have been reported with its use. It has been postulated that these effects may, in part, be related to the development of human antibodies against the chimeric part of the molecule (HACA), and that concurrent use of immunosuppressant drugs such as methotrexate may decrease the development of these antibodies9 and hence reduce some of the side effects associated with the use of infliximab. Furthermore, data suggest that the combination of infliximab and methotrexate may be more effective than either drug alone,10 which may be partly explained by an increase in drug levels but also by a possible synergistic effect on disease pathogenesis. It is unknown whether the same benefits from using methotrexate or other immunosuppressant drugs would accrue in subjects with AS, where disease flares are known to occur 6 weeks after treatment.
Magnetic resonance imaging (MRI) is a sensitive imaging tool that allows excellent visualisation and multiplanar assessment of soft tissues and bone and can identify acute and chronic lesions in AS.11 Recently, the role of MRI in the diagnosis and monitoring of sacroiliac and spinal disease activity in AS has been explored by different groups,12 and although more validation work needs to be done, it is rapidly becoming the preferred imaging method in AS. Likewise, dual energy x ray absorptiometry (DXA) is a sensitive method of quantifying bone mineral density (BMD). Importantly, osteoporosis is an early feature of active AS.13 This study, therefore, aimed at assessing the efficacy, safety, and duration of response to the combination of infliximab with methotrexate in AS and whether the addition of methotrexate could prolong response to infliximab treatment.
METHODS
Study design and randomisation
This study was designed as a 30 week, single centre, randomised, double blind placebo controlled trial and had the approval of the local research ethics committee. All subjects gave written informed consent. A 2:1 randomisation list was generated by a statistician (who was unconnected with the final analysis of results), with two thirds of the subjects being included in the infliximab group and one third in the placebo group. Study participants, clinical observers, and metrologists were unaware of the randomisation code, which was kept in the hospital pharmacy.
Subjects were allowed to continue taking NSAIDs or oral corticosteroids, or both, provided that the dose was unaltered throughout the study. Other DMARDs were stopped at least 4 weeks before the baseline visit. No intra-articular or intramuscular injections of corticosteroids were allowed during the study. If these were required because of an unacceptably high level of disease activity, subjects could be dropped from the study at the investigator’s discretion.
Study drugs
Infusions of infliximab (5 mg/kg in 250 ml 0.9% NaCl) or placebo were prepared by the hospital pharmacy under aseptic conditions. The infusion regimen was weeks 0, 2, 6, 14, and 22. In addition, all subjects were provided at week 0 with a prescription for oral methotrexate at a dose of 7.5 mg with folic acid cover (5 mg twice a week), which would be eventually increased to 10 mg a week.
Subjects
Subjects eligible for the study were recruited from specialist rheumatology clinics in the Yorkshire region and needed to fulfil the modified New York criteria for AS,14 be older than 18 years of age, and have active spinal disease. This was defined as persistent inflammatory back pain (defined as 3 cm or more on a 10 cm visual analogue scale (VAS)) and a raised inflammatory response in serum as shown by a C reactive protein (CRP) value of more than 10 mg/l despite treatment with conventional agents such as an optimal dosage of non-steroidal anti-inflammatory drugs (NSAIDs) or DMARDs. Exclusion criteria included any history of tuberculosis, active infection, demyelinating disease, previous lymphoproliferative or malignant disorder, pregnancy, breast feeding, or uncontrolled concomitant disease in the opinion of the investigator. Subjects who had received an investigational drug within 3 months of the start of the study were excluded.
Assessments of efficacy and outcome
Subjects were seen for clinical evaluation at baseline, weeks 4, 10, and 30. The following variables were evaluated: Bath Ankylosing Spondylitis Disease Activity Index (BASDAI),15 Bath Ankylosing Spondylitis Functional Index (BASFI),16 10 cm VAS to measure spinal pain during the day and night, as well as the physician global assessment of disease activity and duration of early morning stiffness (minutes). Item number 4 of the BASDAI, considered to represent a VAS for enthesopathy, was analysed independently. In addition, a quality of life instrument, the Ankylosing Spondylitis Quality of Life questionnaire (ASQoL),17 was used. Laboratory tests performed included the measurement of inflammatory markers such as the CRP, complete blood count, liver function tests, and levels of antinuclear antibodies (ANA). HLA-B27 type was determined in all cases at baseline.
The primary outcome was evaluation of change in the BASDAI score at weeks 4, 10, and 30. Secondary outcomes included comparison of the proportions of subjects in each arm achieving response criteria proposed by the ASsessments in Ankylosing Spondylitis (ASAS) Group.18 This is presented as ASAS 20, defined as a 20% improvement of at least 10 units (scale 0–100) in at least three of the following four domains: subject’s global assessment, pain, function (as represented by the BASFI), and inflammation (represented by morning stiffness measures as described in the BASDAI), in the absence of deterioration in the remaining domain. In addition, the recently defined ASAS response for biologics criteria19 was analysed. According to this, a subject was deemed to be a responder if they satisfied the following criteria: 50% relative change or absolute change of 2 (scale 0–10) in the BASDAI and expert opinion.
Imaging
Magnetic resonance imaging (MRI)
Scans of the sacroiliac joints (SIJs) and lumbar spine were performed at 0 and 30 weeks using a commercially available 1.5 T Philips Gyroscan ACS NT (Philips Medical Systems, Best, The Netherlands).
The following sequences were used: T1 weighted turbo spin echo, T2 weighted SPIR (fat suppressed (FS)) coronal oblique sequences, and T1 FFE SPIR post-gadolinium (Gd-DTPA) (vol 1.5 mm) of the SIJs as well as T2 SPIR sagittal sequence of the lumbar spine. Magnetic resonance measures were as follows: a spin echo sequence with T1 weighted images (repetition time (TR) 908 ms, time to echo (TE) 14 ms, matrix 192/256, field of view (FOV) 320 mm, slice thickness 4.0 mm, slice gap 0.3 mm, number of signals averaged 3, and acquisition time 2:56 m) was used for the SIJs. T2 TSE/FS acquisition measures were as follows: TR 2125 ms, TE 120 ms echo train length, matrix 252/512, FOV 320 mm, slice thickness 4.0 mm, slice gap 0.4 mm, number of signals averaged 3, and acquisition time 2:54 m for the SIJs; and a TR 1327 ms, TE 120, FOV 320, slice thickness 4.0/0.4, matrix 247/512 with an acquisition time of 2:29 m for the spine. Active disease was defined on T2 FS images as bone oedema (identified by high or intermediate marrow signal) and/or soft tissue oedema (high signal in the extracapsular connective tissues), as previously described.20
For MRI scoring, the MRI scans were anonymised and assigned random numbers by an independent assessor. Two experienced observers who did not know the subjects’ clinical characteristics and time sequence scored paired scans using a scoring system previously described, in which sites of spinal/sacroiliac changes of active enthesitis and osteitis were evaluated.20 When the two observers disagreed, a consensus was reached. As previously reported,20 the SIJ was divided into four quadrants for assessment: right upper, left upper, right lower, and left lower. Each quadrant was subdivided into ilial and sacral aspect. Lesions were scored using a semiquantitative scale (0–3). In the spine, lesions were classified as present or absent within the vertebral bodies, the spinous processes, facetal joints, or in the paraspinal soft tissues. A total count of lesions per spinal area for each subject was performed. The degree of change between baseline and follow up scans was assessed using a semiquantitative scale (resolution, improvement, no change, new lesions). The intrarater and interrater reliability of this system for acute oedematous lesions using ICC statistics was: intrarater = (range) 0.64–1.00 for the sacroiliac joints and 0.6–0.77 for the spine; interrater = (range) 0.67–0.85 and 0.80–0.93 for the sacroiliac joints and the spine, respectively.
Dual energy x ray absorptiometry (DXA)
In addition, to assess the effect of both treatments on bone mass, all subjects underwent a DXA examination to measure BMD at the hip (femoral neck and total hip) and spine (L2–L4) at baseline and 30 weeks. All scans were performed by one technician using the same DXA equipment (Lunar Expert, Madison, Wisconsin). For hip BMD analyses, mean values from the left and right hip were used. Short term in vivo precision was 1.43% at the total hip, 2.89% at the femoral neck, and 2.42% at the spine. The long term spine phantom precision for the whole study period was 0.80%.
Statistical analysis
The study was designed with 90% power to detect a response of up to 30% in the placebo group and 80% in the infliximab group, using Holm corrected analysis of covariance (ANCOVA) at the α = 0.017 level, based on preliminary results from open label studies21,22 available at the time of the study design. A 2:1 randomisation was applied with twice as many subjects in the treatment group, as it was expected that the efficacy of methotrexate would be comparable with that of placebo reported in previous trials. This translated into a target sample of 42 subjects to allow for the withdrawal of up to two subjects from each treatment group. An intention to treat analysis was performed and where a subject withdrew before study completion then a last observation carried forward method was used for missing values.
An ANCOVA was used to compare the degree of change in the BASDAI from baseline in the two treatment groups, taking baseline BASDAI as a covariate. Paired t tests were used to assess whether within each treatment group there was a significant reduction in BASDAI from baseline. Non-parametric statistics were applied to all secondary outcome measures, with the exception of the MRI and DXA results, on which ANCOVA and t tests were performed, respectively. Fisher’s exact tests were used to compare proportions of responders between groups. Mann-Whitney U tests were performed to test for differences between groups at baseline, and to compare change scores between groups at weeks 10 and 30. Wilcoxon signed rank tests were used to test for changes within groups from baseline to week 30. Corrections for multiple comparisons were made separately for primary and secondary outcome measures, within families of statistical tests, following the Holm technique.23
Critical p for testing at the α = 0.05 level was therefore set at p = 0.017 for ANCOVA, p = 0.008 for paired t tests (primary outcome) and Fisher’s exact tests, p = 0.017 for paired t tests (secondary outcome), p = 0.017 for independent t tests, p = 0.005 for Wilcoxon signed rank tests, and p = 0.003 for Mann-Whitney U tests.
RESULTS
Study group
Forty two subjects were randomised, 28 to infliximab and 14 to placebo. Both groups started methotrexate 24 hours after the first infusion. One subject in the infliximab group withdrew consent after randomisation, which left 41 subjects for the initial analysis. Another six subjects withdrew from the study before week 30, including four subjects in the placebo group who dropped out before week 4 owing to lack of efficacy. The other two subjects, one from each group, withdrew after week 10 for personal reasons and non-compliance (fig 1⇓). The remaining 35 subjects, 26 receiving infliximab (93%) and 9 receiving placebo (64%) continued in the study until week 30. Table 1⇓ summarises the demographics and characteristics of the subjects in both groups.
Baseline characteristics of the study patients. Values presented are median (range) unless otherwise stated
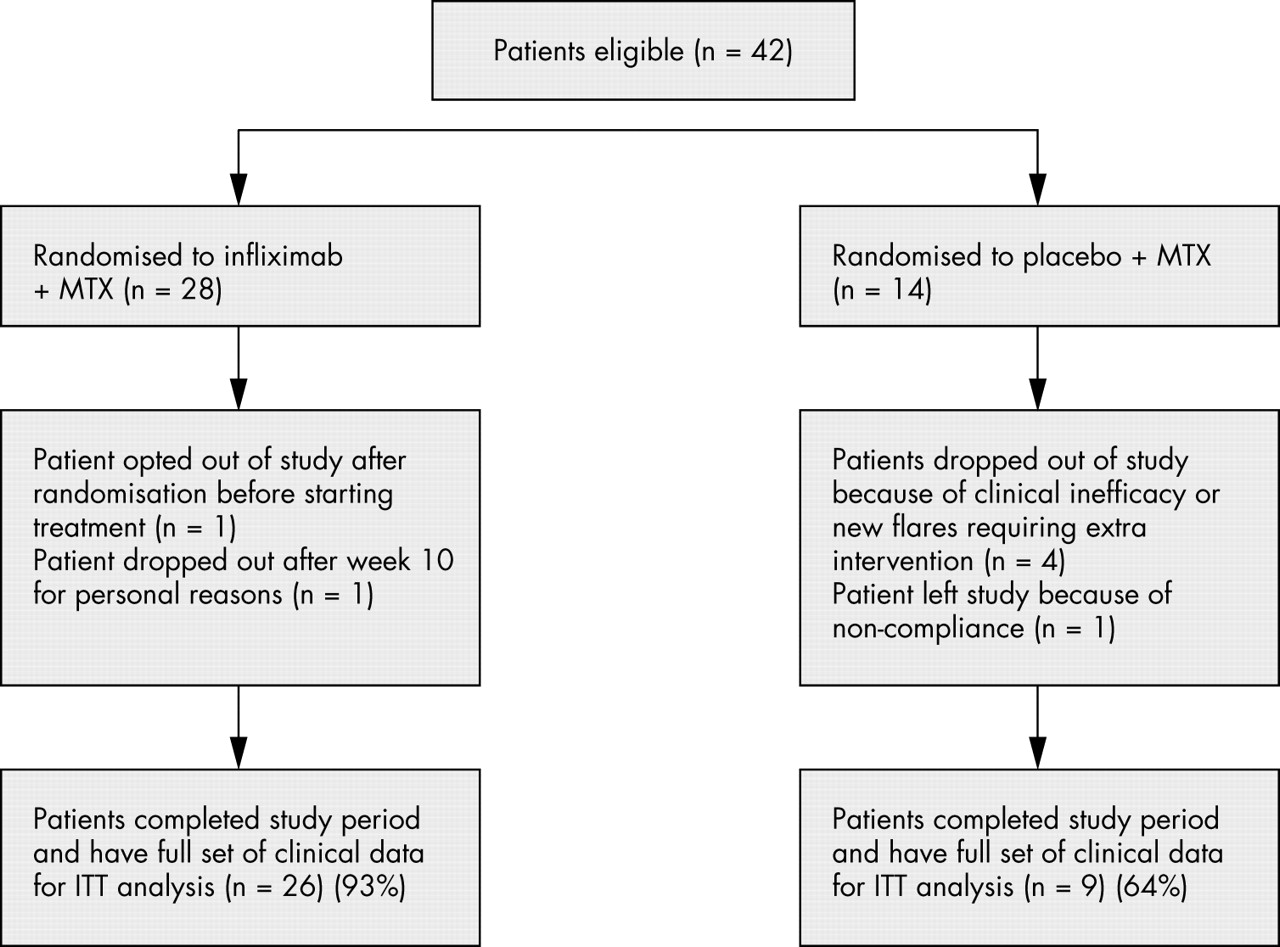
Randomisation, reasons for treatment discontinuation, and numbers of patients who completed the 30 week study period. ITT, intention to treat.
Efficacy results
The intention to treat primary analysis showed that subjects given infliximab in combination with methotrexate showed a greater reduction in BASDAI score at weeks 4, 10, and 30 (mean change −2.0, −3.1, and −1.9, respectively) than the subjects treated with methotrexate alone (mean change −0.6, −1.4, and −0.8). However, this response only achieved significance at week 10 (p = 0.017) and was not maintained at week 30 (p = 0.195), probably reflecting the fact that a number of subjects in the infliximab group reported a flare by week 6 after the last study infusion.
A similar response was also observed in objective measures of disease activity such as the CRP, the improvement in which was significantly greater in the combination group by week 10 (p<0.001) but not significantly different between treatment groups by week 30 (p = 0.017, table 2⇓). Indeed, further subanalysis of the CRP response at the interim visits (weeks 14 and 22) showed a marked deterioration of CRP values by week 22 (mean change 69.3%) for the five subjects who subjectively reported a flare of disease in between study visits (fig 2⇓). When the ASAS 20 response was examined, no significant differences were seen between the groups at any end point (46% v 21% at week 4; p = 0.180; 71% v 28% at week 10, p = 0.019; and 50% v 21% at week 30, p = 0.102) (fig 3A⇓). Analysis of the composite ASAS response criteria for biological agents showed that a significantly greater proportion (50%) of subjects in the infliximab group achieved an ASAS response at week 4 than in the placebo group (7%, p = 0.007), although this response was not maintained at weeks 10 (67% v 35%; p = 0.096) or 30 (53% v 21%; p = 0.057) (fig 3B⇓). A detailed analysis of the groups independently clearly showed that the biggest benefit occurred in the combination group (table 3⇓), where the level of response was equivalent to previously published results.4
Intention to treat analysis of clinical outcomes at all end points. Values are given median (range)
BASDAI response within the groups (*significant difference)

Analysis of CRP results at all study visits examining the subset of patients in the infliximab treated group who reported a flare of disease in the interim visits.

(A) ASAS20 and (B) ASASBIO (composite ASAS response criteria for biological agents) responses.
MRI results
Eight subjects were unable to undergo MRI scanning because of severe postural abnormalities. In addition, a further six subjects either dropped out during the study or did not attend for their follow up scan. In total, pre- and post-treatment MRI scans from 19 subjects in the combination group and nine subjects in the methotrexate monotherapy group were available for analysis.
Overall, 24 (86%) subjects had lesions consistent with active disease (17 in the combination group, 7 in the methotrexate monotherapy group). At baseline, a total of 97 lesions were seen in the combination group (72 lesions in the lumbar spine, 25 lesions in the SIJs) and 107 in the methotrexate monotherapy group (67 in the lumbar spine, 40 in the SIJs). Although an improvement was seen in both groups by week 30, the mean number of lesions for each subject that had resolved completely by week 30 was significantly greater in the combination group (mean 4.7, 95% confidence interval (CI) 3.3 to 6.1) than in the methotrexate monotherapy group (mean 1.4, 95% CI −0.8 to 3.5, p = 0.016). There was a trend towards a greater mean number of lesions for each subject that remained unchanged after treatment in the methotrexate monotherapy group (mean 5.5, 95% CI 3.3 to 7.7) than in the combination treatment group (mean 2.6, 95% CI 1.1 to 4.1); however, after correction for multiple comparisons this difference was not significant (p = 0.038). The mean numbers of new lesions for each subject did not differ significantly between treatment groups (methotrexate, mean 0.9, 95% CI −0.1 to 2.0; combination, mean 0.9, 95% CI −0.2 to 1.6, p = 0.965). A total of 19 new lesions appeared in the combination group (15 in the spine, four in the SIJs), all in subjects who reported flares before week 30. In the methotrexate monotherapy group seven new lesions appeared (six in the spine, one in the SIJs).
When both treatment groups were combined, a significant association was identified between the level of improvement in the BASDAI score and the numbers of lesions that resolved for each subject during treatment (Spearman rank correlation, p = 0.04, see fig 4⇓).
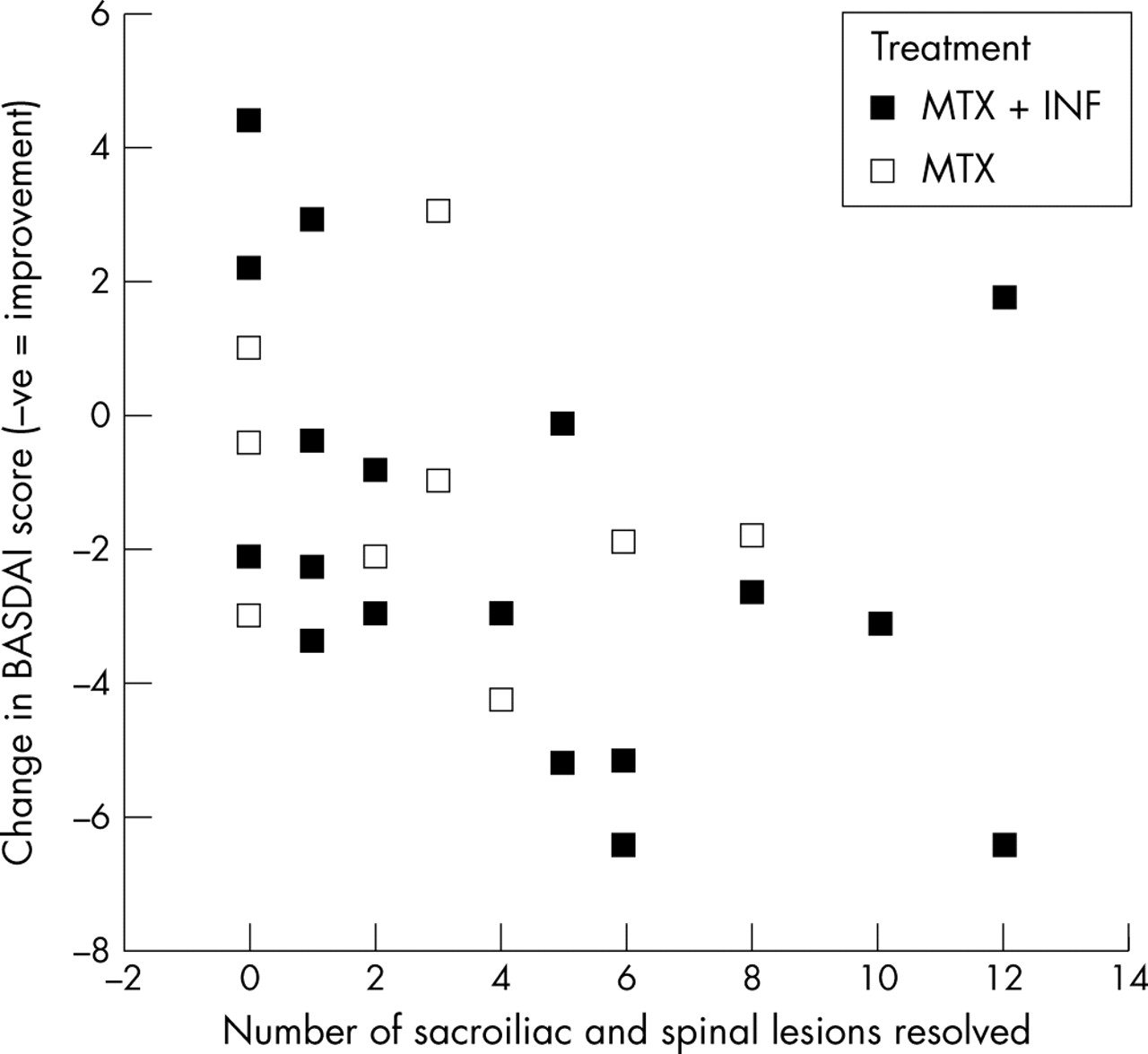
Association between change in BASDAI score and numbers of lesions resolved.
DXA results
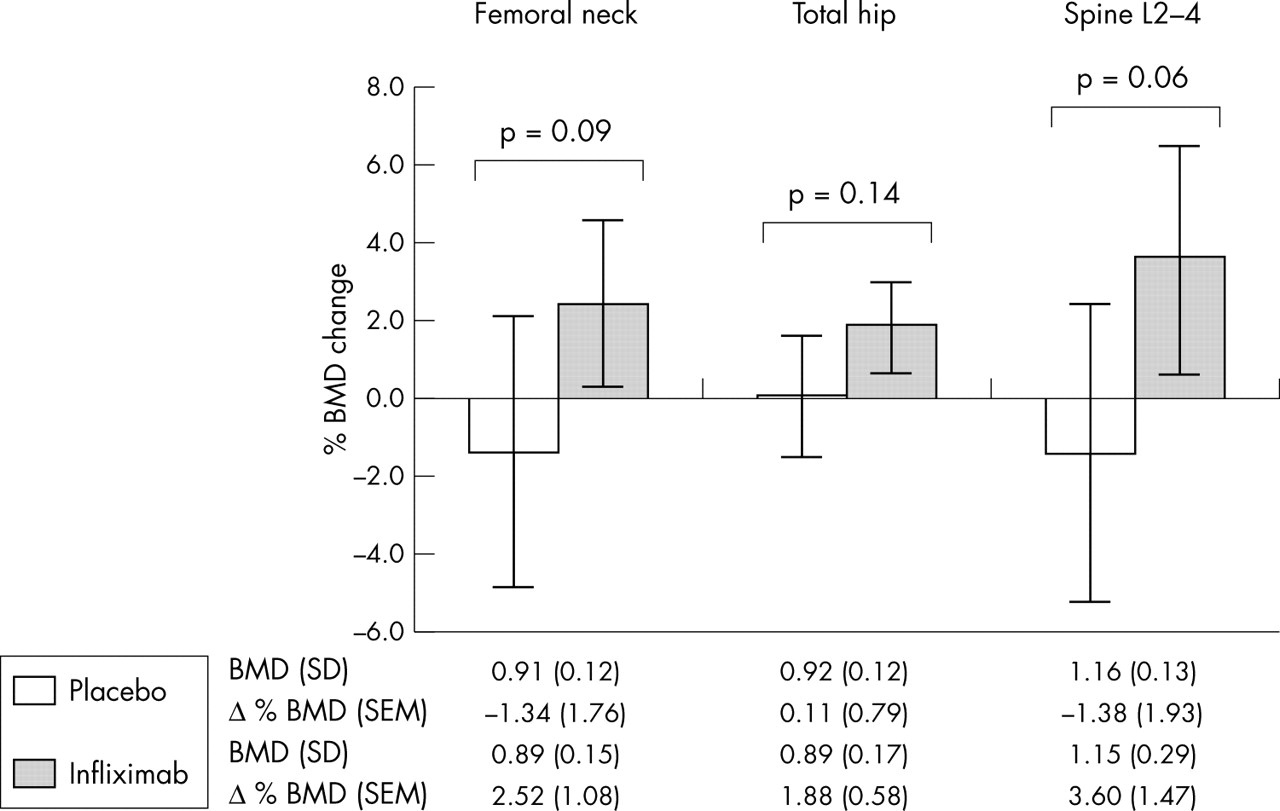
At 30 weeks in the combination group, hip and lumbar spine BMD data were available in 23 and 24, subjects, respectively. In the methotrexate monotherapy group, hip BMD data were available in eight subjects and lumbar spine BMD data were available in 10 subjects. Figure 5⇓ shows that a statistically significant increase in total hip BMD was seen in the infliximab treated group (+1.9%, paired t test p = 0.004), with trends towards increases in femoral neck (+2.5%, p = 0.03) and spine (+3.6%, p = 0.02) BMD, whereas no significant change was seen in the methotrexate monotherapy group at either the femoral neck (−1.3%, p = 0.47), total hip (+0.1, p = 0.90), or spine (−1.4%, p = 0.50). Although there was a trend towards improved BMD in the combination group, comparison between the groups failed to show a significant difference (independent t test p values ranged from 0.06 to 0.14).

DXA results.
Safety data
Both study drugs were well tolerated with the majority of side effects being mild to moderate (table 4⇓). Two subjects in the combination group developed a mild hypersensitivity reaction after the first infusion that settled spontaneously in the first subject and was controlled with regular hydrocortisone cover in the second case. No severe adverse events were seen in either group.
Drug related adverse events
ANA detection
Four subjects in the combination group were ANA positive at baseline in a weak titre (1/40 (n = 3) and 1/80 (n = 1)). No subjects in the methotrexate monotherapy group were ANA positive at baseline. At 30 weeks, a total of 11/28 (39%) subjects were ANA positive in the combination group. Of the four subjects who were initially ANA positive, one subject (ANA 1/40 titre at baseline) was negative at week 30. The remaining three remained positive with a higher titre (1/160 (n = 1), 1/640 (n = 2), all homogeneous pattern). A further eight (29%) subjects in the combination group became ANA positive at week 30 with mildly raised titres. None of the subjects developed clinical symptoms suggestive of a connective tissue disorder. No ANA seroconversion was seen in the methotrexate monotherapy group by week 30.
DISCUSSION
TNFα blockade with infliximab is an important therapeutic advance for subjects with RA and AS. In RA, infliximab used in conjunction with methotrexate results in better safety and efficacy, but this has not been established in AS. As far as we know, this is the first study to look at the efficacy and safety of the combination of infliximab and methotrexate in AS. These results show that the combination regimen was well tolerated with no discontinuations owing to side effects over a 6 month period. This regimen was highly efficacious at 10 weeks, reflecting the immediate improvement known to occur with infliximab, but this effect was not significant at 30 weeks. This reflects the disease flare that was reported by some of the subjects 8 weeks after the last infusion.
Recent reports of monotherapy with infliximab in AS showed a higher incidence of severe adverse events leading to discontinuation of treatment.24 In our study the combination of infliximab and methotrexate was well tolerated with no serious side effects. In addition, although the prevalence of ANA seroconversion was similar to that reported in other studies, this did not appear to be clinically relevant at 30 weeks. Again, these results contrast with those found by other authors25 and although interlaboratory variability on ANA testing should always be considered,26 we believe that this effect may be due to the concomitant use of methotrexate.
The extended infusion regimen interval of 8 weeks was chosen because we postulated that concomitant administration of methotrexate would enhance the duration of response. Accordingly, the primary outcome was set at week 30, 8 weeks after the last infusion was given (week 22). Other studies have reported an impressive clinical response at 12 weeks (comparable with the 10 week efficacy assessments in the present study). However, a number of subjects in our study reported a return of symptoms within 6 weeks of the last infusion, accounting for the apparent lack of efficacy at week 30. In clinical practice this would be overcome by shorter infusion schedules and, indeed, new guidelines suggest an infusion interval of 6 weeks is appropriate.19
The level of response seen in the infliximab treated group when using clinical measures such as the BASDAI is comparable with previous reports. These results also show a small degree of improvement in the monotherapy group treated with methotrexate, which was comparable with the placebo arm of other studies.4 However, there was an improvement in the MRI score in the methotrexate group compared with deterioration in historical studies with placebo controls.27 This may mean that methotrexate has a favourable effect as suggested in small uncontrolled studies7,8 and needs to be confirmed in larger studies in which higher therapeutic doses of methotrexate are achieved.
As shown by imaging methods, the majority of MRI determined lesions in the infliximab treated group improved by week 30 (fig 6⇓) but, interestingly, new regions of enthesitis/osteitis were evident in those subjects who reported a disease flare before the last clinical assessment. In the DXA analysis a clear improvement was seen in the combination treated arm, confirming previous observations from our group that adequate suppression of inflammation leads to improvement of bone mass in subjects with active disease.28 Therefore biological treatment not only suppresses the primary spinal abnormalities but may also reverse secondary abnormalities such as osteoporosis. These imaging findings have important implications for the long term management of these subjects, as osteoporosis is a known complication of active AS and may occur early in the disease process.13,29

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Magnetic resonance images of spine and sacroiliac joints before and after treatment. (A) T2 weighted fat suppressed sagittal sequence of the lumbar spine of a patient showing acute Romanus lesions (thin white arrows) at the anterior inferior aspects of L1 and L3, and anterior superior aspects of L2 and L4 vertebral bodies; (B) complete resolution of the lesions after treatment with infliximab and methotrexate; (C) T2 weighted fat suppressed coronal oblique image of the SIJ of another patient showing active sacroiliitis (thick white arrow) and (D) marked improvement after treatment with infliximab and methotrexate.
A number of limitations in the study need to be taken into account when interpreting these results. Methotrexate was chosen because of previous reports in RA suggesting that an immunogenic effect can be achieved with only a small dose. Because of the lack of data suggesting a therapeutic effect in AS, no higher doses were sought. In addition, the drop out rate from the study was unexpectedly high making interpretation of the results difficult owing to wide differences in standard deviations.
In AS, distinguishing between spinal inflammation and spinal fusion, both of which lead to loss of function, is problematic. In this study, where conventional, clinically based outcomes and imaging determined outcomes were used, the latter were found to be very sensitive for assessing treatment. The response, although suggesting efficacy for both treatment arms, was considerably better for the infliximab arm, confirming that MRI is a valid tool for assessing disease activity in AS. In addition, this study illustrates a scoring method that is reliable and has successfully shown that sensitivity changes over a 6 month period after treatment with different biological agents.17 As is the experience in other units, this scoring method was developed by the combined effort of rheumatologists and radiologists, confirming the need for a close liaison between related specialties in the search for better tools to diagnose and assess disease activity.
In conclusion, this study confirmed that infliximab in combination with methotrexate was safe in AS, but the addition of methotrexate did not sustain response for 8 weeks.
Acknowledgments
We thank sisters Louise Cunnigham, Claire Brown, and Ruth Thorpe for support; Drs Alexander Fraser, Andrew Gough, Michael J Green, Martin Iveson, Michael Martin, Colin Pease, and Richard Reece for referring patients; Paul Astin and Belinda South for statistical advice; Sheena Stewart for help with DXA imaging; Bridget Montague for tissue typing; and Roland Strauss for illustrations.
This study was supported by a grant in aid from Schering-Plough, UK.
Professor McGonagle’s work is sponsored by the Medical Research Council (MRC). Professor Paul Emery and Dr Conaghan are supported by the Arthritis Research Campaign (ARC).
REFERENCES
Footnotes
Published Online First 13 April 2005