Article Text

Abstract
Objective: To determine clinical and immunological correlates of high dose chemotherapy (HDC) + autologous stem cell transplantation (ASCT) in patients with severe rheumatoid arthritis (RA), refractory to conventional treatment.
Methods: Serial samples of peripheral blood and synovial tissue were obtained from seven patients with RA treated with HDC and autologous peripheral blood grafts enriched for CD34+ cells. Disease activity was assessed with the Disease Activity Score (DAS), serum concentrations of C reactive protein (CRP), and human immunoglobulin (HIg) scans, and the extent of immunoablation was determined by immunophenotyping of peripheral blood mononuclear cells, and immunohistochemistry and double immunofluorescence of synovium.
Results: Clinical responders (n = 5) had a larger number of cells at baseline expressing CD3, CD4, CD27, CD45RA, CD45RB, and CD45RO in synovium (p<0.05), higher activity on HIg scans (p = 0.08), and a trend towards higher concentrations of CRP in serum than non-responders (n = 2). Subsequent remissions and relapses in responders paralleled reduction and re-expression, respectively, of T cell markers. A relatively increased expression of CD45RB and CD45RO on synovial CD3+ T cells was seen after HDC + ASCT. No correlations were found between DAS and changes in B cells or macrophage infiltration or synoviocytes.
Conclusions: HDC + ASCT results in profound but incomplete immunoablation of both the memory and naïve T cell compartment, which is associated with longlasting clinical responses in most patients. The findings provide strong circumstantial evidence for a role of T cells in established RA, and demonstrate a role for the synovium in post-transplantation T cell reconstitution.
- AEC, aminoethylcarbazole
- ASCT, autologous stem cell transplantation
- BSA, bovine serum albumin
- CRP, C reactive protein
- DAS, Disease Activity Score
- DMARD, disease modifying antirheumatic drug
- HDC, high dose chemotherapy
- HIg, human immunoglobulin
- HRP, horseradish peroxidase
- IFNγ, interferon γ
- IL, interleukin
- PBS, phosphate buffered saline
- RA, rheumatoid arthritis
- TNF, tumour necrosis factor
- rheumatoid arthritis
- stem cell transplantation
- immunoablation
- synovial T cells
Statistics from Altmetric.com
- AEC, aminoethylcarbazole
- ASCT, autologous stem cell transplantation
- BSA, bovine serum albumin
- CRP, C reactive protein
- DAS, Disease Activity Score
- DMARD, disease modifying antirheumatic drug
- HDC, high dose chemotherapy
- HIg, human immunoglobulin
- HRP, horseradish peroxidase
- IFNγ, interferon γ
- IL, interleukin
- PBS, phosphate buffered saline
- RA, rheumatoid arthritis
- TNF, tumour necrosis factor
High dose chemotherapy (HDC) followed by autologous stem cell transplantation (ASCT) is an experimental treatment for severe autoimmune diseases, including refractory rheumatoid arthritis (RA). A number of clinical studies have demonstrated long term responses in patients with RA previously refractory to disease modifying antirheumatic drugs (DMARDs).1–8 The rationale of this strategy is based on the concept of immunoablation by intense immunosuppression with subsequent regeneration of naive T lymphocytes derived from reinfused haematopoietic progenitor cells.9 The mechanism by which HDC + ASCT exerts its antirheumatic effects has not yet been defined. It has been postulated that intensive immunosuppressive treatment followed by ASCT may be effective for the control of RA because the conditioning regimen deletes the relevant autoreactive lymphocyte population and the reinfused stem cells develop into a lymphocyte population that acquires self tolerance. Experimental studies of autoimmune disease in rodents have lent support to this concept, but no comprehensive studies have been done in humans.
We examined samples taken serially from synovial tissue and blood from seven patients with RA treated with HDC + ASCT in an attempt to unravel pathogenetic mechanisms in RA. We used lineage specific markers to analyse cellular infiltrates in the synovium, as well as activation and inflammatory markers, to assess disease activity at the tissue level.
PATIENTS AND METHODS
Patients
Seven patients with RA (mean age 49 years, range 35–55; disease duration 12 years, range 7–20) were treated at Leiden University Medical Centre (LUMC) with HDC + ASCT as part of a multicentre phase I/II trial.7 The protocol was approved by the LUMC medical ethical committee and the patients gave written informed consent to undergo arthroscopic procedures as described below. All patients had an established diagnosis of RA according to American College of Rheumatology criteria.10 Eligibility criteria were destructive disease; failure to respond to ⩾4 antirheumatic drugs, including maximal tolerable dose of methotrexate and combination therapy; and a clinically inflamed knee. Tumour necrosis factor (TNF) blockade had also failed in four patients. Table 1 summarises measures of disease activity and concurrent DMARDs.
Drugs used at the time of arthroscopy
Detection of the monoclonal antibodies was performed using affinity purified and horseradish peroxidase (HRP) conjugated goat antimouse antibodies (Dako), rabbit antirat-HRP (Dako), and goat antirabbit-HRP (BD Pharmingen), the biotinyl tyramide/streptavidin-HRP amplification system (NEN Life Science Products Inc, Boston, MA, USA), and aminoethylcarbazole (AEC; Sigma, St Louis, MO, USA). The HRP conjugated antibodies were diluted in phosphate buffered saline (PBS)/bovine serum albumin (BSA) (1%) with 10% normal human serum (Bloedbank LUMC, Leiden, The Netherlands) as blocking serum, and incubated for 30 minutes. A biotinyl tyramide/streptavidin-HRP amplification system (NEN Life Science Products Inc, Boston, MA, USA), and AEC (Sigma, St. Louis, MO, USA) was used to enhance staining. A biotinyl tyramide solution was added and slides were incubated for 30 minutes, followed by subsequent incubation with streptavidin-HRP in PBS/BSA (1%) for 30 minutes. HRP activity was detected using hydrogen peroxide as substrate, and AEC as dye. After washing with distilled water, the sections were counterstained with Mayer’s Hämalaunlösung (Merck), and mounted with Kaiser’s glycerol gelatin (Merck).
All patients had a high Disease Activity Score (DAS) at baseline as defined by EULAR criteria.11 Autologous haematopoietic stem cells were mobilised using a single infusion of cyclophosphamide 4 g/m2 followed by filgrastim (granulocyte-colony stimulating factor) 10 μg/kg/day subcutaneously until leukapheresis. Immunomagnetic selection of CD34+ cells from the leukapheresis product was performed using the Clinimacs Device (Miltenyi Biotec, Munich, Germany). DMARDs were discontinued before mobilisation and not reinstituted until at least 3 months after transplantation if deemed necessary owing to recurrence or persistence of disease activity. Corticosteroids were tapered when possible. Non-steroidal anti-inflammatory drugs were continued in the lowest dosage needed to control pain and morning stiffness. The conditioning regimen consisted of intravenous cyclophosphamide 200 mg/kg followed by reinfusion of the CD34+ enriched graft.
Clinical assessment
Clinical assessment was performed on the day synovial biopsies were obtained using the DAS.12 DAS = (0.54×√ Ritchie articular index (tender joint count)) + (0.065×number of swollen joints) + (0.33×ln ESR) + (0.0072× patient disease activity visual analogue scale). We refer to the DAS website for detailed information on this score: http://www.das-score.nl/www.das-score.nl/index.html (accessed 27 July 2005).
Human immunoglobulin (HIg) scan
HIg scans were performed at baseline and at 3 months after transplantation according to standard operating procedures.13 Disease activity was assessed by scoring total uptake in joints by two independent observers (RV and MW) on a four point scale (0 = no; 1 = light; 2 = moderate; 3 = strong uptake).
Synovial tissue
Synovial tissue specimens were obtained from patients by serial arthroscopy. The baseline arthroscopy was performed before mobilisation (n = 7). The first arthroscopy after transplantation was performed at a mean interval of 86 days (range 60–127) after transplantation (n = 7). The second arthroscopy was performed with a mean interval of 1.4 years (range 405–577 days) after transplantation (n = 5). The arthroscopy procedure was performed in the inflamed knee. Five millimetre biopsy specimens of synovial tissue were taken. A minimum of 10 biopsy samples was obtained and analysed for each patient at each time point.
Immunohistochemistry
Sections of biopsy specimens taken at baseline and 3 months after transplantation were stained with monoclonal antibodies (table 2). The following markers were investigated on the 1 year post-transplantation samples: CD3, CD4, CD8, CD27, CD45RA, CD45RB, CD45RO, CD55, CD68. Immunohistochemical staining procedures were performed as follows. Slides were warmed up to room temperature, fixed in acetone (Merck) at room temperature for 10 minutes, and air dried. After each step, the sections were washed with PBS (Apotheek LUMC, Leiden, The Netherlands). All incubations were carried out at room temperature. Endogenous peroxidase activity was inhibited using 0.1% sodium azide (Merck) and 1% hydrogen peroxide (Merck) in PBS. The monoclonal antibodies were diluted in PBS with 1% BSA (ICN Biomedicals Inc, Aurora, OH), and incubated for 60 minutes. Interleukin (IL) 1β, IL4, IL10, IL12, and interferon γ (IFNγ) were incubated for 18 hours. For control sections, the IgG1 isotype control (anti-KLH, Pharmingen) or PBS was applied.
Primary and secondary antibodies used for immunohistochemistry studies
Immunofluorescence double staining
To characterise subsets of CD3+ cells in the five responders, double staining procedures were performed with CD45RA, CD45RB, CD45RO, and CD27 (table 3). The following combinations of markers were used in order to identify different cell types: naïve T cells (CD45RA and CD27), memory T cells (CD45RO), and early versus more mature T cells (CD45RB) in combinations described in table 3.
Primary and secondary antibodies used for immunofluorescence double staining
Microscopic analysis of immunohistochemically stained slides
Sections were coded and randomly analysed. All areas of each biopsy section were examined and histological features were scored semiquantitatively by two observers (RV and RF or RV and LvD), who were unaware of the clinical data. The expression of CD3, CD4, CD8, CD27, CD45RA, CD45RB, CD45RO, CD55, CD56, CD68, CD25, CD62E, CD62L, CD69, HLA-DR, CD19, CD38, IL1β, IL4, IL12, IFNγ, TNFα, and IL10 was scored on a five point scale (0–4). A score of 0 was given to those sections with minimal infiltration and/or low expression, whereas a score of 4 represented large infiltration by numerous lymphocytes, macrophages, or a strong expression of a certain cell surface marker. For the evaluation of CD4+ cells, only cells with lymphocyte morphology were included, because CD4 can be expressed on monocytes. The scoring is calibrated for each marker, and has been developed previously by examining ⩾5 biopsy specimens of rheumatoid synovial tissues.14 Interobserver readings were identical or differed by only one point, and all differences that did occur were resolved by agreement.
Microscopic analysis of haematoxylin and eosin stained slides
Haematoxylin and eosin stained sections were scored for the degree of infiltration with lymphocytes, plasma cells, and polymorphonuclear cells on a five point scale (0–4) by two observers (RV and PM Kluin), who were unaware of the clinical data. These quantitative scores corresponded with the numbers of cells per high power field (787.5x), as described earlier.15 A score of 0 was given to those sections with minimal infiltration, whereas a score of 4 represented infiltration by numerous cells. A composite inflammation score was calculated by summing the scores for the four components: synovial lining hyperplasia, and infiltration with lymphocytes, plasma cells, and polymorphonuclear cells (range 0–14).
Microscopic analysis of immunofluorescence stained slides
Immunofluorescence double staining in the five responders was scored by counting at least 100 of single or double positive cells.
Peripheral blood T cell reconstitution analysis
Immunophenotyping studies were carried out on peripheral blood mononuclear cells obtained at baseline, and at 1, 3, 6, 9, and 12 months after transplantation. The following combinations of markers were used to identify different cell types: naïve CD4 and CD8 T cells, memory CD4 and CD8 T cells, and early versus more mature CD4 and CD8 T cells (see table 4 for antibodies used).
Antibodies used for flow cytometric analysis of peripheral blood T lymphocytes
Statistical analysis
Non-parametric techniques (Wilcoxon signed rank tests) were used to test whether measures of disease activity and immunological parameters after transplantation differed significantly from baseline. Differences between responders and non-responders were assessed using the Mann-Whitney U test. A Pearson correlation coefficient was calculated to assess the relationship between serum concentrations of C reactive protein (CRP) and scores on HIg scans.
RESULTS
Clinical efficacy
The seven patients displayed a dichotomous clinical response to HDC + ASCT, with 5/7 patients attaining a good response based on the EULAR response criteria for disease activity (mean DAS from 5.33 to 1.89; p = 0.04), at 3 months after transplantation. Of the two remaining patients (referred to as “non-responders”) one had an initially moderate response (DAS from 6.61 at baseline to 3.85 at 3 months), but then progressed, while the other failed to respond at all (DAS from 4.71 at baseline to 5.16 at 3 months). TNF blockade also failed in four patients. Two of these four patients responded favourably to HDC + ASCT. At the time of the second arthroscopy none of the seven patients were receiving DMARDs; however, these were reinstituted during the first year after transplantation in the two non-responders and in 3/5 responders because of flares. One year after transplantation the five responders underwent a third arthroscopy. The mean DAS in these patients at the time of the third biopsy was 2.78 (range 2.47–3.26, p = 0.04 versus baseline) (table 1).
HIg scan
Baseline HIg scores and CRP concentrations were highly correlated (r = 0.91, p<0.01), as were the changes after HDC + ASCT (r = 0.91, p = 0.01). The five clinical responders differed from the two non-responders in baseline HIg scan score (mean 2.4 v 0.5, p = 0.08) and serum concentrations of CRP (mean 54.2 g/l v 34 g/l, p = 0.44).
Haematoxylin and eosin stained slides
The mean inflammation score in the whole group decreased from 6.17 at baseline to 2.33 at 3 months after transplantation (p = 0.06), and from 5.75 to 1.75 in the responders (p = 0.14). A reduction of >50% in the inflammation score was seen in 4/7 patients after transplantation (fig 1).

Synovial tissue taken from patient No 2 (table 1) before and 3 months after HDC + ASCT. Infiltration with numerous lymphocytes and plasma cells before stem cell transplantation, which were almost absent after the transplantation.
Immunohistochemistry
Clinical responders had a high expression at baseline of CD3, CD4, CD27, CD45RA, CD45RB, CD45RO in synovium while the non-responders lacked a significant synovial T cell infiltrate (table 5, fig 2). The expression of these markers decreased at 3 months after transplantation in the responders, and was significant for CD45RA and CD27 (p = 0.04). When the changes between responders and non-responders were compared, significant differences were found for CD45RA and CD27 (p = 0.05; Mann-Whitney U test) (figs 2 and 3). Changes in other surface markers and cytokines were found, but these were not significant except for IL10, which was significantly higher in the whole group at 3 months (p = 0.04), and IL1, which was significantly higher in non-responders at 3 months after transplantation (4.0 v 0.60; p = 0.02) (table 5). Expression of IL4 and transforming growth factor β was considered too low to allow meaningful analyses. At 1 year after transplantation, expression of CD3, CD4, CD27, CD45RA, CD45RO, but not CD45RB, had returned to baseline levels in the responders (fig 3).
Immunohistochemical scores at baseline and three months after HDC + ASCT for responders and non-responders

Immunohistochemically stained synovial tissue in a responder with CD3, CD27, CD45RA, and CD45RO, before and 3 months after HDC + ASCT.
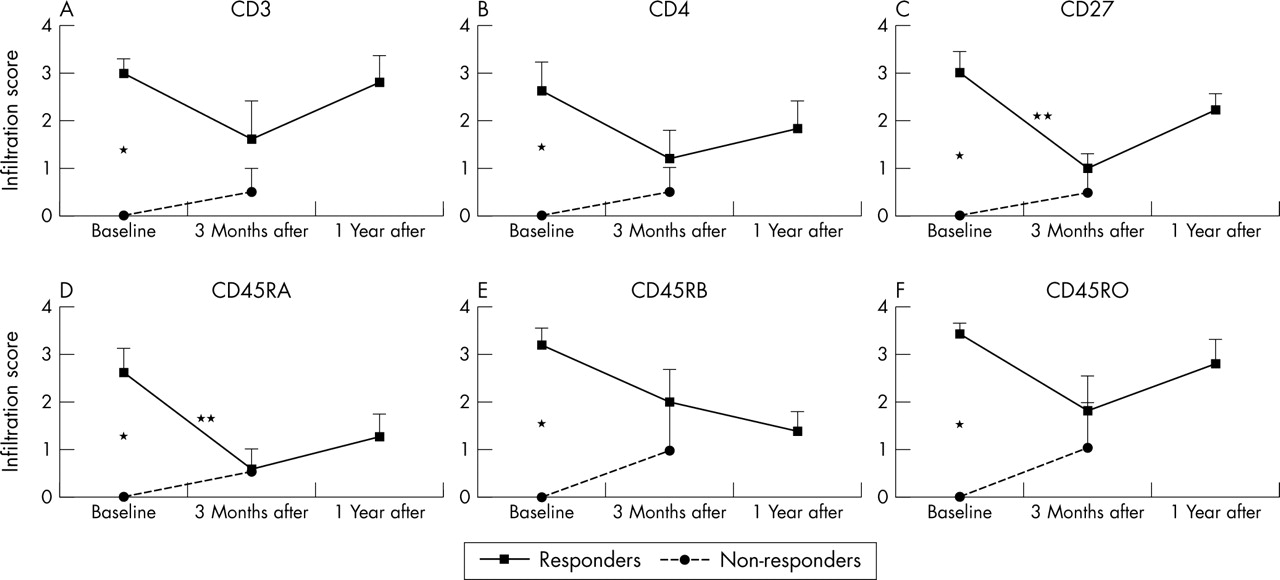
Semiquantitative infiltration scores before, 3 months after, and 1 year after HDC + ASCT of responders and non-responders for CD3, CD4, CD27, CD45RA, CD45RB, and CD45RO. *p<0.05, significant baseline difference between responders and non-responders; **p<0.05, significant decrease at 3 months after transplantation in responders CD45RA and CD27.
Immunofluorescence double staining
Immunofluorescence double staining was performed in the five responders to investigate co-expression of CD27 and CD45R isoforms on synovial CD3 T cells. At baseline 72% (range 56–86%) of CD27+ cells were CD3+ and 88% (range 57–99%) of CD45RO+ cells were CD3+ (fig 4). Vice versa, of CD3+ cells 68% (range 55–93%) were CD45RO+, 22% (range 5.5–32.7%) CD45RA+, and 34% (range 16.5–86%) CD45RB+. Three months after transplantation, CD45RA+ was expressed only on 9% of CD3+ cells but CD45RO+ on 90% (fig 4). A high proportion of CD3+ T cells co-expressed CD45RB (66%, range 48.9–72.4%, p = 0.04) at 3 months after transplantation. One year after transplantation the distribution of CD45R isoforms on CD3+ T cells had returned to baseline levels (see fig 6).

Co-expression of CD3 and CD45RO in RA synovial tissue before transplantation in a responder. CD3 (FITC = green) and CD45RO (TRITC = red) were detected using immunofluorescence techniques. (A) Rheumatoid synovial tissue showing CD3+ cell infiltrate. (B) Rheumatoid synovial tissue showing CD45RO+ cell infiltrate. (C) Double positive cells as depicted by yellow and orange, showing numerous double positive and only a few CD45RO single positive cells (red).
Cell surface antigens in peripheral blood
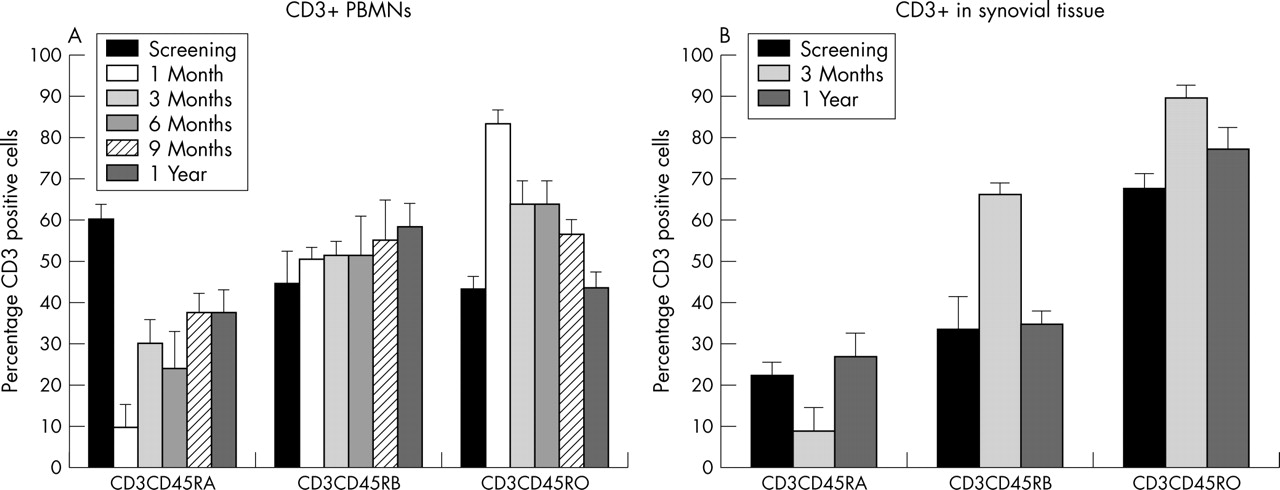
To compare the reconstitution results of T cell subsets in the synovial tissue in the five responders, flow cytometric analyses of peripheral blood mononuclear cells in the five responders were performed focusing on CD45RA, CD45RB, and CD45RO expression on CD4+ and CD8+ cells. Absolute cell counts in peripheral blood after HDC + ASCT were characterised by prolonged lymphopenia of CD4+ T cells and transient expansion of CD8+ T cells (fig 5). Numbers of B cells, monocytes, and natural killer (NK) cells decreased transiently but had returned to baseline numbers by 3–6 months (not shown). We then focused on the relative reconstitution of T cells in blood versus synovium. Figure 6 shows that a greater proportion of CD45RA+ T cells and a lower proportion of CD45RO+ T cells were present in peripheral blood than in synovial tissue at baseline. In the first months after transplantation the percentage of CD45RA in peripheral blood decreased and remained lower than baseline for the duration of the follow up. A relative increase in CD45RO+ T cells was observed, which was significant up to 6 months after transplantation (p = 0.03). This was mostly due to the transient peripheral expansion of CD8+ memory T cells (not shown). The percentage of CD45RB+ cells remained relatively constant over time in peripheral blood, contrasting with the findings in synovial tissue described above.

Absolute cell count in peripheral blood mononuclear cells in the five responders for CD3, CD4, and CD8. Absolute cell numbers were calculated by multiplying absolute lymphocyte count (106/l (SEM)) by the percentage of each subset determined by flow cytometry after isolation of peripheral blood mononuclear cells by density gradient centrifugation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The mean number of CD45RA, CD45RB, and CD45RO expressed as a percentage of CD3+cells. (A) Immunofluorescence double staining of peripheral blood mononuclear cells with CD3 plus CD45RA, CD45RB, or CD45RO in the five responders at screening and at 1, 3, 6, 9, and 12 months after HDC + ASCT. Results expressed as the percentage of CD3 cells expressing the CD45R isoform. (B) Immunofluorescence double staining of synovial cells with CD3 plus CD45RA, CD45RB, or CD45RO in the five responders at screening and 3 and 12 months after HDC + ASCT. Results expressed as the percentage of CD3 cells expressing the CD45R isoform.
DISCUSSION
This study was undertaken to advance our understanding of the immunological effects of HDC + ASCT in RA. This experimental treatment modality has been employed in recent years as a means to profoundly perturb the immune system of patients with severe autoimmune disease, including RA. Substantial improvements of disease activity have been reported in a number of studies, although treatment failures and relapses have also been seen (reviewed by Verburg et al9). Data on immunological correlates of the clinical responses in RA are scarce, but the persistence of serum autoantibodies in many patients who have undergone transplantation suggested that eradication of autoreactive B cells was not achieved, possibly contributing to the failure to induce long term remission in these patients. An overall decrease in the titre of IgM rheumatoid factor and anti-cyclic citrullinated peptides was seen at 3 and 6 months after transplantation. However, concentrations returned to pretransplantation levels 1 year after transplantation.
Of all the measures investigated in this study those involving the T cell compartment were most pronounced, particularly in the patients with high inflammatory activity as measured by serum levels of CRP and uptake on HIg scans. Failure of TNF blocking treatment or any other clinical or laboratory variable was not predictive of clinical response. The induction of (partial) remission was, however, associated with strong baseline expression and subsequent reduction of CD3, CD4, and the differentiation markers CD27 and the CD45 isoforms (RA, RB, RO) in synovium, but expression of these markers had returned to baseline levels at the 1 year biopsy at a time when the disease had relapsed to varying extents in most patients. Although changes in other cell subsets occurred, no association was found between disease activity and the number of macrophages (CD68+ cells), B cells (CD19+ cells), plasma cells (CD38+ cells), or fibroblast-like synoviocytes (CD55+ cells). Marked expression of proinflammatory cytokines—notably of IL1, remained detectable after transplant, in the two non-responders.
Of interest was the high proportion of CD45RB+ CD3+ T cells at 3 months after transplantation, and the gradual increase of this subset among peripheral blood T cells. This subset has recently been reported to be increased in the peripheral blood of patients with RA in comparison with healthy controls, reflecting accelerated differentiation of naive CD45RA T cells under the influence of inflammation.16 Co-expression of high levels of CD45RB and CD45RO and loss of CD45RA on T cells has been shown to reflect a phenotype typical of recently activated T cells.17 The overrepresentation of T cells with a similar phenotype in the synovium at 3 months suggests either the selective migration of newly developed T cells expressing high levels of CD45RB from blood, and/or local differentiation and/or expansion in the synovium, probably under the influence of homoeostatic pressures or a local inflammatory drive as suggested by the results on cytokine expression. Any of these possibilities might contribute to the prolonged depletion of T cells from peripheral blood, which is a feature of patients with RA after lymphocytotoxic treatment.18,19,20,21,22 Why some patients have more abundant T cell infiltration at baseline and respond favourably is not known. It may be attributed either to differences in the pathogenesis or in fluctuations of disease state.
In non-responders an influx of inflammatory cells and cytokines after transplantation was observed possibly related to stopping DMARDs at the time of the first biopsy, whereas these DMARDs were not used at the second arthroscopy. The non-responders showed an increase in inflammatory cytokines—notably, IL1 and TNFα. Both cytokines are believed to have a central role in the pathogenesis of RA. The procedure in this subset of patients with HDC seems to worsen the disease rather than ameliorate it. In responders there was a general trend towards a decrease in all cytokine markers, except for IL10 and IFNγ. The increase in IFNγ may be explained by a relative increase of CD45RB+ cells, which were shown to produce IFNγ.
Our data, though for obvious reasons just a snapshot, provide strong circumstantial evidence for an active role of T cells in the perpetuation of disease activity.23 Whether attracted to, or expanding in, the synovium specifically or non-specifically, interaction of T cells with residual lymphoid or myeloid cells or resident cells such as synoviocytes could turn a subclinical synovitis into a clinically manifest synovitis.24,25 The findings from our study on the central role of CD4+ T cell infiltration add to the accumulating evidence from earlier case reports of patients with RA and juvenile idiopathic arthritis treated with HDC + ASCT, and patients with psoriatic arthritis treated with T cell depleting monoclonal antibodies.26,27,28
Our study raises the important question as to whether more intense immunosuppression to the extent of myeloablation or post-transplantation immunosuppression is necessary to attain lasting remission. Preclinical studies and a recent registry analysis of transplants in human autoimmune disease have lent support to this concept.29 In none of our patients was complete ablation of the synovial T cell compartment achieved, at least not at the time points evaluated. Also, autoantibodies (rheumatoid factor and anti-cyclic citrullinated peptides) remained detectable in serum taken at monthly intervals for 2 years (not shown). Given the complex immune dysregulation in RA—notably, in the late stages, it is conceivable that a more comprehensive treatment may indeed be needed. The key goal from a T cell centred perspective would be to induce sufficient immunoablation to allow regeneration of regulatory elements. HDC + ASCT may provide a brief opportunity to establish tolerance against selected autoantigens. Our data suggest such a strategy would not be effective in patients with a low synovial T cell load. Whether different pathogenetic mechanisms are involved in such patients remains to be determined, but a recent study does point in this direction.30 A baseline synovial biopsy seems useful to discriminate between the two categories.
To our knowledge, this is the first comprehensive study to examine clinical and immunological correlates of HDC + ASCT in RA. Although the number of patients investigated was small, and technical issues precluded the use of in situ multiparameter staining of the synovial T cell population, the data disclose interesting aspects of pathogenetic mechanisms operative in RA. The association of clinical responses with T cell debulking in the joint, recurrence of disease activity with re-emergence of T cell infiltration of synovium, and the lack of a relation between disease activity and other cell types in blood or synovium lend support to the concept that T cells have a role in established disease. The changes in relative expression of the different CD45 isoforms in synovial tissue in comparison with blood suggest that T cell repopulation in the joint is dictated by local homoeostatic forces, selective homing, or antigenic stimulation. More complete eradication of the synovial T cell compartment or post-transplantation immunosuppression may be needed to induce more robust remissions, but whether the risks of these steps outweigh the risks of more intense immunosuppression remains to be determined.
Acknowledgments
We thank Professor Dr PM Kluin for his expert advice on analysis of synovial tissue specimens.
Financial support for this study was obtained from the Dutch Arthritis Association (NR 99-1-301).
REFERENCES
Footnotes
-
Published Online First 13 April 2005
-
There are no competing interests