Article Text

Abstract
Objective: To measure synovial tissue interleukin-18 (IL-18) expression in patients with inflammatory arthritis, and to identify associations with serum levels, disease activity, and response to treatment.
Methods: Synovial tissue biopsies and serum samples were obtained from patients with early, active, rheumatoid arthritis (RA) (n = 12), undifferentiated seronegative arthritis (SnA) (n = 9), psoriatic arthritis (PsA) (n = 5), and reactive arthritis (ReA) (n = 2) before and one year after introduction of disease modifying antirheumatic drug (DMARD) treatment. Osteoarthritis (OA) tissues were compared. Tissue IL-18 expression was determined after immunohistochemical staining using a semiquantitative scale. Serum IL-18 was measured by enzyme linked immunosorbent assay.
Results: Before treatment was started, tissue IL-18 expression was increased in each diagnostic group compared with OA (p<0.05). Tissue IL-18 expression was correlated with serum C reactive protein levels (r = 0.53, p = 0.003) but not with serum IL-18. After DMARD treatment, 12 patients (five RA, four SnA, three PsA) were re-evaluated. Decreases in tissue IL-18 expression were observed in eight, although the trend did not reach significance (p = 0.068). Changes in tissue IL-18 expression were correlated with changes in serum IL-18 (r = 0.62, p = 0.041) and C reactive protein (r = 0.72, p = 0.009).
Conclusions: Synovial tissue IL-18 expression was correlated with disease activity in inflammatory arthritis. After treatment, tissue levels changed in parallel with changes in serum IL-18 and with changes in the acute phase response. These observations support a role for IL-18 in the pathophysiology of inflammatory arthritis.
- DMARD, disease modifying anti-rheumatic drug
- IL, interleukin
- OA, osteoarthritis
- PBMC, peripheral blood mononuclear cells
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- ReA, reactive arthritis
- SnA, undifferentiated seronegative arthritis
- DMARD
- arthritis
- interleukin-18
- synovial tissue
Statistics from Altmetric.com
- DMARD, disease modifying anti-rheumatic drug
- IL, interleukin
- OA, osteoarthritis
- PBMC, peripheral blood mononuclear cells
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- ReA, reactive arthritis
- SnA, undifferentiated seronegative arthritis
Rheumatoid arthritis, along with other categories of inflammatory arthritis, is characterised by prominent synovial tissue inflammation. Abundant new blood vessel formation facilitates infiltration by many activated cell populations that participate in complex pathophysiological pathways. Activated T lymphocytes accumulate in the perivascular areas. B lymphocytes, plasma cells, neutrophils, and dendritic cells may also appear prominently. Large numbers of macrophages and fibroblast-like synoviocytes accumulate in the synovial lining layer. Interleukin-1 (IL-1) and tumour necrosis factor α (TNFα), produced mainly by activated macrophages, are pro-inflammatory cytokines that play a critical role in the pathophysiology of synovial inflammation.1
Interleukin-18 (IL-18), a member of the IL-1 superfamily, was first identified as an interferon-γ (IFN-γ) inducing factor,2 and is widely expressed in human tissues.3 Its precursor, pro-IL-18, is cleaved by interleukin-1β converting enzyme to yield mature, active IL-18.4 Two IL-18 receptors—IL-18Rα and IL-18Rβ—have been identified and cloned, and both are important for IL-18 signalling.5,6 IL-18 binding protein (IL-18BP) is a decoy receptor with multiple isoforms which further modulates the bioactivity of circulating and tissue IL-18.7 IL-18 has a highly diverse range of biological functions, including the stimulation of Th1 differentiation, synergy with other cytokines, and the induction of cytokine production and release from peripheral blood mononuclear cells (PBMC), T cells, and tissue macrophages.8,9 In addition, IL-18 induces the expression of CXC chemokines by synovial fibroblasts, stimulates angiogenesis, enhances mononuclear cell recruitment, and promotes articular degradation.10–13 Raised serum concentrations of IL-18 have been identified in various chronic inflammatory diseases, including rheumatoid arthritis, adult onset Still’s disease, and chronic liver disease.14,15 The demonstration of IL-18 mRNA and protein in the synovial tissues of patients with rheumatoid arthritis suggested a role in pathogenesis.9 IL-18 expression in synovial tissue is associated with IL-1β and TNFα expression, with local tissue inflammation, and with the acute phase response.16 Treatments that inhibited IL-18 resulted in the improvement of animal models of arthritis.17,18
Our aim in this study was to quantify expression of IL-18 in synovial tissue and serum from patients with different categories of inflammatory arthritis, and to measure changes in those undergoing treatment with disease modifying antirheumatic drugs (DMARD).
METHODS
Patients
The patients included in this study had been referred to the early arthritis clinic at St Vincent’s University Hospital, Dublin. Patients with active inflammatory arthritis, including a clinically inflamed knee joint, consented to arthroscopic or blind needle synovial biopsy from the affected knee before starting appropriate DMARD treatment. Patients were diagnosed with rheumatoid arthritis (RA), psoriatic arthritis (PsA), or reactive arthritis (ReA) if they satisfied the American College of Rheumatology criteria for the diagnosis of rheumatoid arthritis, the criteria of Veale et al for psoriatic arthritis, or the criteria of Amor et al for reactive arthritis.19–21 Nine patients were categorised as having undifferentiated seronegative arthritis (SnA).
After completing DMARD treatment for one year, all patients were invited to undergo a second synovial tissue biopsy. Twelve consented. Serum samples were collected at each time point. Synovial tissue from the knee joints of patients with osteoarthritis was also evaluated. This banked osteoarthritis tissue had been previously obtained at either arthroscopic examination or joint replacement surgery. Serum samples from these patients were unavailable for this study.
Preparation of synovial tissue
Multiple synovial tissue biopsies were taken from each patient under local anaesthesia using either a Parker-Pearson needle or a 2.7 mm arthroscope and 2.8 mm universal biopsy forceps (Karl Storz GmbH & Co, Tuttlingen, Germany). Ethical approval for synovial biopsy was obtained from St Vincent’s University Hospital ethics committee. The synovial tissue was prepared as previously described.22 In brief, tissue samples were snap frozen together en bloc in Tissue-Tek OCT (Miles Inc Diagnostic Division, Elkhart, Indiana, USA) by immersion in methylbutane (−70°C). Frozen blocks were stored in liquid nitrogen until sectioned for staining. Sections (7 μm) were cut in a cryostat and mounted on glass slides. The slides were fixed in acetone at room temperature for 10 minutes and stored at −70°C until immunohistochemical analysis was done. After thawing for 20 minutes at room temperature, sections were stained using an anti-human IL-18 mouse monoclonal antibody (2D3B6, MD Biosciences, Zurich, Switzerland). The antibody used recognises mature active IL-18, but not its precursor.9 A standard three stage immunoperoxidase method was used, and was followed by counterstaining with haematoxylin. Sections in which the anti-IL-18 monoclonal antibody was replaced with an isotype matched irrelevant primary antibody served as negative controls.
Microscopic analysis of synovial tissue
Immunohistochemically stained synovial tissue sections were examined using a light microscope. IL-18 expression throughout the entire area of each section was evaluated and scored semiquantitatively on a scale of 0 to 4, where 0 represents little infiltration and 4 represents extensive infiltration. The validity and reproducibility of this scoring system have been reported previously.23 Sections from patients who contributed tissue after treatment were also examined using high power (400×) magnification. Three hundred randomly selected lining layer cells per section were evaluated, and the percentage of lining layer cells staining positively was calculated. Two to four early arthritis tissue sections and single osteoarthritis (OA) sections were available to derive mean scores for each patient time point. All synovial tissue sections were coded and analysed in random sequence by two blinded observers. After unblinding, minor differences between observers were resolved by agreement. In order to calculate intraobserver variation, all analyses were carried out in duplicate by a single observer (TR).
Measurement of serum IL-18 expression
Circulating serum IL-18 levels at each patient time point were measured using a commercially available enzyme linked immunoassay (Medical and Biological Laboratories, Nagoya, Japan) at the Division of Immunology and Allergy, University Hospital, Geneva (PRL). The assay used detected total serum IL-18, including IL-18 bound to IL-18BP. The methodology and validation of this assay have been described in detail previously.24
Statistical analysis
All statistical calculations were done using SPSS software (version 10.0). Simultaneous comparisons between multiple patient groups were carried out using one way analysis of variance or Kruskal–Wallis tests. Differences between pairs of patient groups were evaluated using Student’s unpaired t test or the Mann–Whitney U test. Student’s paired t test or the Wilcoxon signed ranks test was employed to examine differences in variables between baseline and one year. Correlations were expressed using Pearson’s or Spearman’s coefficients. Only two tailed significance tests were used, and probability (p) values of less than 0.05 were taken as significant.
RESULTS
Patient characteristics
Thirteen male and 15 female patients with early inflammatory arthritis were evaluated (table 1). The four different disease subgroups did not differ significantly with respect to age (p = 0.355) or pretreatment C reactive protein concentrations (p = 0.508).
Patient characteristics at pretreatment evaluation
IL-18 expression before treatment
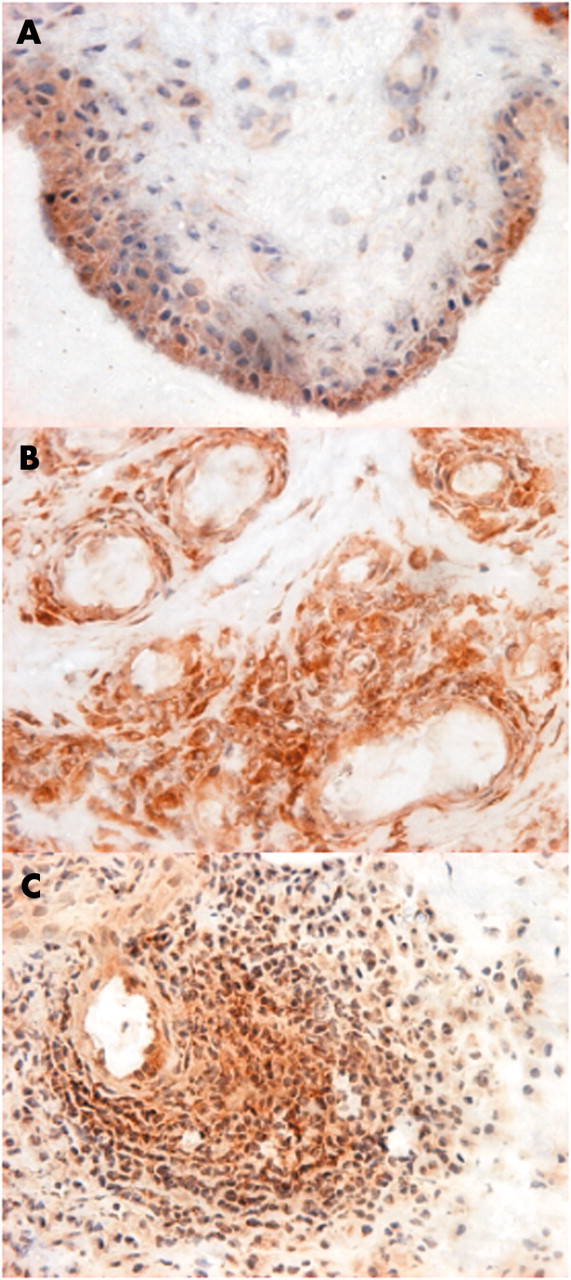
After immunohistochemical staining, microscopic analysis of biopsy sections obtained from the early arthritis group showed a wide range of synovial tissue IL-18 infiltration. Cells in the lining layer, endothelial cells, and sublining cellular aggregates in which the principal component cells showed phenotypic characteristics of tissue macrophages had the most prominent IL-18 expression (fig 1). In many patients, abundant synovial tissue IL-18 expression (scores 3–4) was evident, while few patients (2/28) had low levels of expression (scores 0–1) (fig 2A). The mean (median; range) semiquantitative score for synovial tissue IL-18 expression in the total early arthritis group was 2.49 (2.50; 0.33 to 4.00): RA, 2.40 (2.17; 1.50 to 3.67); SnA, 2.44 (2.50; 1.00 to 3.67); PsA, 2.70 (3.00; 0.33 to 4.00); ReA, 2.75 (2.75; 2.50 to 3.00). Synovial tissue IL-18 expression did not differ significantly between these diagnostic subgroups (p = 0.798), and when analysed separately, each of the RA, SnA, PsA, and ReA groups showed significantly higher tissue levels than OA (p<0.05 for each); the mean (median; range) score for OA was 1.44 (1.00; 1.00 to 2.00). A range of serum IL-18 concentrations was also observed in the early arthritis group (fig 2B). Many values (16/28) exceeded the normal reference range for healthy individuals (37–215 pg/ml). The mean (median; range) level of circulating serum IL-18 was 256.2 pg/ml (240.0; 95.0 to 501.0): RA, 268.0 pg/ml (301.0; 96.0 to 435.0); SnA, 277.2 pg/ml (266.0; 95.0 to 596.0); PsA, 201.0 pg/ml (188.0; 147.0 to 281.0); ReA, 207.5 pg/ml (207.5; 199.0 to 216.0). Serum IL-18 concentrations did not differ significantly between diagnostic groups (p = 0.557).

Photomicrographs of synovial tissue sections obtained from patients with active inflammatory arthritis, showing interleukin-18 (IL-18) expression in the lining layer (A), endothelial cells (B), and aggregating inflammatory cells in the sublining layer (C). IL-18 positive cells are shown actively infiltrating perivascular tissue in panels B and C. (Original magnification ×200.)

Interleukin-18 (IL-18) expression in synovial tissue (A) and serum (B) in patients with active inflammatory arthritis. After immunohistochemical staining, tissue IL-18 expression was evaluated using a semiquantitative scale of 0 to 4, where 0 represents little expression and 4 intense expression. Serum IL-18 was measured by enzyme linked immunosorbent assay. The upper limit of the normal reference range for serum IL-18 in healthy subjects is indicated. OA, osteoarthritis; PsA, psoriatic arthritis; RA, rheumatoid arthritis; ReA, reactive arthritis; SnA, seronegative arthritis.
Synovial tissue IL-18 expression in the early arthritis group correlated significantly with serum C reactive protein (r = 0.53, p = 0.003) (fig 3). Correlations between synovial tissue IL-18 expression and serum C reactive protein in the smaller diagnostic subgroups were significant for RA (r = 0.68, p = 0.016) and SnA (r = 0.74, p = 0.024). A similar trend was observed for PsA, but was not statistically significant (r = 0.78, p = 0.118). No significant correlations were observed between serum IL-18 levels and either synovial tissue IL-18 expression (r = −0.11, p = 0.590) or serum C reactive protein (r = 0.14, p = 0.512) in the early arthritis cohort.

Synovial tissue interleukin-18 (IL-18) expression and serum C reactive protein in patients with active inflammatory arthritis. The correlation coefficient was calculated using Spearman’s rank correlation test.
Effects of treatment on IL-18 expression
Twelve patients consented to a second synovial tissue biopsy after one year of treatment with either methotrexate (n = 7) or sulphasalazine (n = 5) (table 2).
Synovial tissue and serum IL-18 values before and after treatment with a disease modifying antirheumatic drug
Age, disease duration, C reactive protein, and tissue and serum IL-18 concentrations before treatment did not differ significantly between this group and the patients who did not submit to a second biopsy procedure. Synovial tissue IL-18 expression decreased in eight of the 12 patients. This trend did not reach statistical significance in the group overall (p = 0.068). A further trend towards a decrease in the percentage of lining layer cells expressing IL-18 after treatment was observed, with the mean (median; range) decreasing from 95% (99; 77 to 99) to 82% (95; 48 to 100) (p = 0.067, data not shown). In those patients whose tissue IL-18 expression either increased (Nos 4, 9, 10) or remained unchanged (No 11), serum IL-18 levels also increased or did not change. The changes in synovial tissue IL-18 expression after treatment correlated significantly with changes in serum IL-18 (r = 0.62, p = 0.041). Serum C reactive protein fell significantly after treatment (p = 0.013). Patients with the greatest improvements in C reactive protein (Nos 2, 7, 8, 12) showed the highest levels of baseline tissue IL-18 expression, and in three of the four patients (Nos 2, 7, 12), the most striking decreases in tissue IL-18 expression. C reactive protein concentrations were notably low both before (0–14 mg/l) and after treatment (0–12 mg/l) in the four patients whose synovial tissue IL-18 expression did not decrease. A significant correlation between the changes in tissue IL-18 expression and changes in serum C reactive protein levels was also observed (r = 0.72, p = 0.009) (fig 4). A correlation between changes in serum IL-18 and changes in C reactive protein levels was found, but was not statistically significant (r = 0.52, p = 0.10). Interobserver and intraobserver variations were both less than 5%.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in synovial tissue interleukin-18 (IL-18) expression versus changes in serum C reactive protein levels after one year of methotrexate (n = 7) or sulphasalazine (n = 5) treatment in patients with inflammatory arthritis. The correlation coefficient was calculated using Spearman’s rank correlation test.
DISCUSSION
In this study, abundant IL-18 expression was confirmed in synovial tissue samples from most patients with early rheumatoid arthritis, as well as from patients with seronegative arthritis, psoriatic arthritis, and reactive arthritis. Various previous studies have highlighted synovial tissue IL-18 expression in established rheumatoid arthritis.9,12,16,25 This is the first to demonstrate prominent tissue IL-18 expression in other categories of early inflammatory arthritis. In cross sectional analysis, tissue IL-18 expression, but not serum levels, correlated significantly with the acute phase response. An association between synovial tissue IL-18 expression and the acute phase response has been observed by others in established rheumatoid arthritis16 but not in other categories of arthritis.
Another novel feature of this study was the evaluation of synovial tissue expression and serum levels of IL-18 at the same time points. A range of serum IL-18 concentrations was observed across the disease categories, including some individual values that were within the normal reference range. No significant associations were observed between serum IL-18 values and either synovial tissue IL-18 expression or C reactive protein. Thus, both the patients with ReA had serum IL-18 values that were within the normal range and yet had abundant synovial tissue IL-18 expression. In previous studies, raised serum IL-18 concentrations have been described in adult onset Still’s disease and rheumatoid arthritis. Inconsistent associations between serum IL-18 levels and the acute phase response were found in these studies,25–28 suggesting the need for caution when including serum measures of IL-18 as a marker of disease activity.
A third novel aspect of this study concerned the effects of treatment on IL-18 expression. Following conventional DMARD therapy for one year, the levels of tissue IL-18 expression were reduced in eight of 12 patients who underwent a repeat synovial biopsy of the same joint. This trend failed to reach statistical significance in the small patient sample evaluated. Of interest, there was a significant association between the changes in synovial tissue IL-18 expression after treatment and changes in serum levels of both IL-18 and C reactive protein. Thus, in five of seven patients showing a decrease in the level of tissue IL-18 expression there were also decreases in the serum levels of IL-18, even in patients whose baseline serum levels were within the normal range. In the four patients with either an increase or no change in tissue IL-18 expression, there were parallel changes in the serum levels. Synchronous changes in serum and synovial tissue cytokine expression after treatment have been observed by others.29 The absolute change in serum levels of IL-18 after treatment in this study was not significant, and the association between changes in serum IL-18 levels and C reactive protein failed to reach significance. The effects of treatment on serum IL-18 concentrations in inflammatory arthritis have been examined previously. In one study involving patients with early rheumatoid arthritis, serum IL-18 levels did not change significantly after one year of methotrexate treatment.28 In contrast, when infliximab was given to patients with active established rheumatoid arthritis, significant and consistent decreases in serum IL-18 were observed after 14 weeks.30
The bioactivity of IL-18 is modulated at many levels. IL-18 mRNA production, protein synthesis, cleavage, and release, and differential expression of IL-18 receptor and IL-18BP isoforms interact in a variety of biological environments, under the influence of many pro- and anti-inflammatory cytokines. These pathways are further influenced by internal and external positive and negative feedback loops.3,6,7,9,25,27,31,32 Given the exquisite complexity of this biological network, it is not surprising that levels of individual cytokines in serum do not consistently parallel the acute phase response in inflammatory disease.25–28,33,34 This was illustrated in one study of interferon-α treatment in patients with chronic liver disease, in which changes in the relative proportions of free and protein bound plasma IL-18 occurred earlier than changes in total plasma IL-18.35 Many immunoassays would therefore have failed to detect this biologically important phenomenon. Raised levels of bioactive IL-18 in serum related inconsistently to measures of disease activity in previous studies, and changed in parallel with tissue IL-18 in the present study. A meaningful role in disease is therefore strongly suggested. However, there is some evidence that in diseases characterised predominantly by synovitis, the pathophysiological role of IL-18 in the circulation may be of lesser importance than its activity within the joint. In rheumatoid arthritis, IL-18 concentrations in synovial fluid exceed those found in serum,9 and in one study IL-18 was consistently unable to produce the same potent induction of TNFα and IL-1β in rheumatoid PBMC that it had induced in previous studies in rheumatoid synovial tissue macrophages and in PBMC from healthy subjects.8,9,31
In synovial tissue, IL-18 is predominantly produced by CD68+ macrophages and is potently induced by TNFα and IL-1β.9 Studies in vivo as well as in vitro have consistently highlighted its pivotal role in synovial tissue inflammation.9,14,16,17 It is therefore not surprising that DMARD treatment—which improves clinical and microscopic synovitis and suppresses synovial TNFα and IL-1β expression1,36–39—should produce meaningful changes in tissue IL-18. It is unclear whether the changes in tissue IL-18 expression following treatment in this study were a direct or an indirect DMARD effect. It is probable that non-specific treatment effects on several inflammatory mechanisms, including cellular infiltration and TNFα and IL-1β production, contributed to these changes. Nevertheless, a reduction in both the absolute number and the proportion of lining layer cells that expressed IL-18 after treatment suggests a DMARD mediated effect.
Prospective studies evaluating the effects of treatment on IL-18/IL18BP expression in tissue and serum in larger numbers of patients would clarify the importance of our observations. They are consistent with the suggestion that IL-18 plays a critical proinflammatory role in the pathophysiology of inflammatory arthritis,3,9,14 and support the hypothesis that treatment which inhibits the production of, or neutralises, endogenous IL-18 may effectively control synovial tissue inflammation.
Acknowledgments
We would like to acknowledge Martina Gogarty and Laura Greenan for maintenance of the synovial tissue bank, and Douglas Veale for provision of osteoarthritis synovial tissue.