Article Text

Abstract
OBJECTIVE To assess organ involvement according to a modified Medsger severity scale and its relation to outcome and prognosis in patients with systemic sclerosis.
METHODS One hundred consecutive patients observed in Lund with systemic sclerosis were followed up for a period of 14 years. The mean follow up time was 7.7 years. Initial assessment and an annual evaluation was performed for each patient, with a mean visit frequency of 5.6 per patient.
RESULTS Age at referral, high total skin score, truncal skin involvement, low vital capacity, low static lung compliance, low Cr-EDTA clearance, and ECG abnormalities at the initial assessment predict poor outcome. A severity scoring system for five organ systems indicates a slow progression of organ dysfunction after recruitment into the study. The female: male ratio was 2:1, the mean age at onset of symptoms was 42.3 (range 3–82), and the mean age at recruitment was 47.2 years (range 17–82). Thirty patients died during the follow up period at the mean age of 61.3 years (range 33–85). The causes of death were directly related to systemic sclerosis in at least 10 patients, infections in six, cancers in nine, and other causes in four patients. The standardised mortality ratio was 3.5 and 3.7 for men and women, respectively.
CONCLUSION A high severity score for function of vital organs was shown to predict shortened survival. In this study a severity score based on simple clinical assessment variables was able to predict poor outcome from extensive skin changes, ECG changes, and compromised lung and renal function. Organ dysfunction mainly became manifest during the first five years of the disease, whereafter organ function remained largely stable.
- scleroderma
- severity score
- prognosis
Statistics from Altmetric.com
Systemic sclerosis (SSc) is a rare disease that causes excessive collagen deposition and fibrosis in skin and internal organs. Endothelial cell alteration with vasomotor instability, permeability changes and thickening of the intimal layer of arterioles, and perivascular mononuclear cell infiltration are present before fibrosis is apparent in target organs. Inflammation and fibrosis in internal organs can cause organ failure and premature death.1Predicting outcome for an individual patient with scleroderma is not easy because the disease can be heterogeneous in its presentation. The spectrum of the disease ranges from rapidly progressive generalised fibrosis of the skin and vital internal organs like heart, lungs, gastrointestinal tract, and kidneys to a more indolent form developing over a long period of time.2 The prognosis is affected by cutaneous, and internal organ involvement and other factors, and although no cure is available for SSc, certain disease manifestations like vasomotor instability, hypertension, cardiopulmonary dysfunction, and oesophageal problems can be treated.3-7 Treatment targeting affected organs may alter the long term outcome of the disease. This is supported by improved survival in some recent reports8 ,9 compared with earlier studies.10 ,11 Early active treatment is in need of better clinical or laboratory based measures of severity and prognosis. In cooperation with other European and North American units, we worked on a severity index as a first step to this end.12 However, only longitudinal observation over extended time periods can provide a test of how useful such an instrument may be. In this structured cohort study 100 consecutively admitted patients with scleroderma were followed up for a period of 14 years, and prognosis and outcome evaluated by organ involvement and laboratory variables, using a scoring system similar to the European, North American one.12
Patients and methods
One hundred consecutively admitted patients with SSc, fulfilling the American Rheumatism Association criteria,13 were followed up in Lund from January 198214 to December 1995. The mean follow up time was 7.7 years (range 0.3–12.8); 64 patients were followed up for more than five years. The mean visit frequency was 5.6 per patient. The patients were divided according to skin involvement. Thus 66 patients had limited and 34 had diffuse SSc. Table1 shows the demographic data. Disease onset was defined as the beginning of skin involvement.
Demographic data on 100 patients with systemic sclerosis (SSc). Results given as mean (range)
SKIN ASSESSMENT
Skin involvement was determined by palpation over 24 anatomical sites, and grading the findings on a 0–3 scale, with 0 being normal and 3 hidebound dermal sclerosis. The scores for all sites were added, giving the total skin score. The mean skin thickness of the proximal and middle phalanx of both second fingers was examined with dynamic 10 MHz ultrasound.15
LUNG FUNCTION
Vital capacity (VC) was measured with a water-filled spirometer and total lung capacity was measured with body plethysmography. Static lung compliance (Cst) was measured over the pressure interval 5–15 mm H2O; these variables were expressed in relation to predicted values in age and sex matched healthy subjects.16
RENAL FUNCTION
Glomerular filtration rate was determined by 51Cr-EDTA clearance expressed as ml/min.
GASTROINTESTINAL TRACT FUNCTION
Oesophageal function was assessed by cinematography, repeated boluses of barium were swallowed. Motility was recorded with the patient in a prone position, and graded on a 0–3 scale, where 0 was normal oesophageal function and 3 signified complete absence of propulsive motility. A fat meal containing [14C]triolein was given to the patient after an overnight fast. Breath14CO2 was collected at two, four, five, and six hours. Peak expiratory 14CO2 (percentage of a given dose/h) was used as a measure of fat absorption.17
CARDIAC FUNCTION
Cardiac function was assessed by ECG; the most common changes were ST or T wave changes, followed by bundle branch block, hemiblock, and septal infarction pattern. Acrolysis and calcinosis were assessed byx ray examination. Erythrocyte sedimentation rate expressed in mm/1st h, haemoglobin (g/l), creatinine (μmol/l), and antinuclear antibody (rat liver substrate) expressed as inverse titre, titrated to the highest dilution, were performed as routine in the laboratory of the hospital.
DISEASE SEVERITY SCORING SYSTEM
We constructed a disease severity scoring system adapted from a recently developed severity scale by Medsger et al based on assessing the function of five organ systems.12 We use different organ function assessment techniques in some instances from those reported in Medsger's paper. Thus the function severity score of some organs had to be omitted because of lack of recorded data. This applied to peripheral vascular organs, joint/tendon, muscle, and heart. In other instances we used a different measuring system. For general health we used haemoglobin instead of packed cell volume and weight loss. Skin score was determined by palpation over 24 anatomical sites, identical with those defined by Rodnan, but using 0–3 instead of a 0–4 scale. This results in a theoretical range from 0–72.13 Cinematography and the triolein breath test were used to assess involvement of the gastrointestinal tract. Lung function was graded by VC and Cst instead of carbon monoxide transfer factor and forced vital capacity and renal function by Cr-EDTA clearance instead of serum creatinine and urine analysis in the Medsger severity scale.12 In all instances an effort was made to make our scoring of organ function comparable with the severity scale of Medsger et al.Organ function was graded in five grades: 0 (no documented involvement), 1 (mild involvement), 2 (moderate involvement), 3 (severe involvement), and 4 (end stage organ failure). Table 2 shows the grades by which the criteria were defined. Scoring was performed at inclusion in the study and thereafter at each visit. A Kaplan-Meier survival analysis was used to test the effect of the severity score on survival.
Severity index scoring system of organ function in patients with systemic sclerosis (SSc). The definition of the categories used is given below. For each organ system grades of 0 (no involvement)—4 (end stage failure). Scoring system used to assess survival function
CAUSES OF DEATH
The causes of death and its relation to SSc were subdivided according to the following four categories: (a) unequivocally SSc related, death caused by organ failure; (b) probably SSc related, death caused by a complication caused or aggravated by SSc related to organ injury or treatment; (c) possibly SSc related, death caused by a manifestation reported to have a greater prevalence in SSc—for example, malignancy or suicide; (d) death apparently unrelated to SSc, treatment or organ involvement.9
STATISTICS
Logistic regression univariate model and the χ2 test were used to assess the effect of different variables on prognosis.
Results
Demographic data are shown in (table 1). During the 14 year follow up 30 of the 100 patients had died, at a mean age of 61.3 years (range 33–85). There was no difference in survival according to sex, but patients with lSSc had longer survival than those with dSSc. When assessment at first visit was used as a reference, the following variables were predictors of non-survival. Older age at inclusion, higher skin score, reduced VC, reduced total lung capacity, and reduced Cst, were significant predictors of fatal outcome. This also applied to low Cr-EDTA clearance and abnormal electrocardiogram (ECG). No other laboratory variables nor the presence of acrolysis, digital ulcers or telangiectasia were found to have any prognostic implication (tables 3and 4).
Variables in relation to prognosis in 100 patients with systemic sclerosis, first visit clinical assessment, mean follow up time 7.7 years
Proportion of abnormal or normal variables among non-survivors. Figures refer to number of patients
There was an inverse correlation between skin score and VC (p<0.001), and age and Cr-EDTA clearance (p<0.001). There was a correlation between VC and Cr-EDTA clearance (p=0.001), and inverse correlation between Cr-EDTA clearance and the formation of calcium deposits (p=0.016).
Table 2 shows the severity scoring system. No mean change in the severity index score was observed for Cr-EDTA in 81%, for VC/Cst in 71%, for cinematography/[14C]triolein in 75%, for skin score in 75%, and haemoglobin in 80% of the patients during the follow up period. The mean time from the onset of symptoms to recruitment into the study was 4.8 years (table 1). Figure 1illustrates years of survival after recruitment, and deaths related to age, showing that 50% of the patients that die do so within the first five years after recruitment.

Survival time in non-survivors. Within six years from recruitment into the study 16 of 30 non-survivors died, 2/3 of them were over 50 years of age at the time of death.
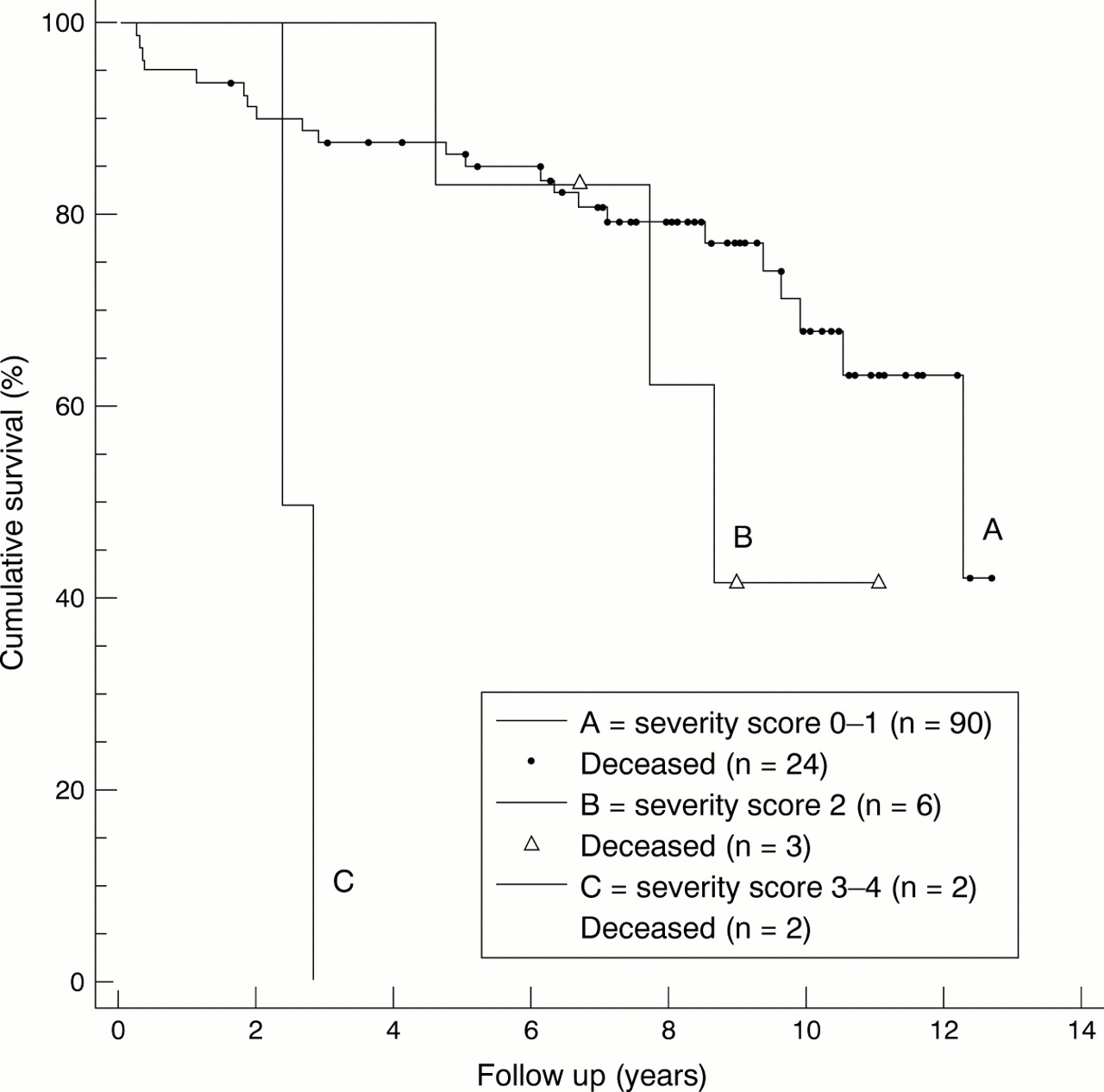
By using Kaplan-Meier cumulative survival plots, we estimated survival function according to initial organ system severity score for each of the five organ systems, and type of disease, during the period of follow up. Diffuse skin involvement was as expected a prognostic factor, with a significantly decreased patient survival compared with those with limited skin involvement (fig 2). When skin score was used as a determinant of survival no difference in survival for patients with severity score 0–1 and severity scores 2 and 3–4 was seen. When Cr-EDTA clearance was taken as a determinant of survival, patients with a severity score of 0–1 had better survival than patients with severity score 2 or more (fig 3). Haemoglobin as a determinant of survival differentiated between patients with score 0–1 and score 2 (fig 4). VC and Cst as a measure of lung function were variables that differentiated for survival between patients with severity score 0–1, severity score 2, and severity score 3–4 (fig 5). Difference in survival was also seen over time between groups with variable gastrointestinal function (fig 6).

Kaplan-Meier cumulative survival plot. Skin involvement as a determinant of survival in systemic sclerosis. Improved survival for patients with limited systemic sclerosis (p=0.015).

Kaplan-Meier cumulative survival plot. Renal function measured by Cr-EDTA clearance as a determinant of survival in systemic sclerosis, grouping of patients according to severity score 0–1, 2, and 3–4. There is a significantly improved survival for those with severity score of 0–1 compared with severity score 2 (p<0.001).

Kaplan-Meier cumulative survival plot. Haemoglobin as a determinant of survival in systemic sclerosis. There is a significantly improved survival for patients with severity score of 0–1 compared with severity score 2 (p= 0.0003).

Kaplan-Meier cumulative survival plot. Lung function measured by vital capacity and static lung compliance as a determinant of survival in systemic sclerosis. Grouping of patients according to severity score 0–1, 2, and 3–4. Improved survival for those patients with severity score of 0–1 compared with severity scores 2 and 3–4 (p=0.0077).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier cumulative survival plot. Gastrointestinal function measured by cinematography and triolein test as a determinant of survival in systemic sclerosis. Grouping of patients according to severity score 0–1, 2, and 3–4, showing improved survival for patients with severity score of 0–1 compared with severity scores 2 and 3–4 (p<0.0001).
Mortality was analysed according to the causes of death and its relationship with SSc. Ten deaths were judged as definitely related to SSc, four of which were due to intrinsic lung disease with respiratory insufficiency and four further cases to cardiac failure considered to be secondary to scleroderma heart disease, one of those had acute effusive pericarditis with cardiac compression as a contributory cause. One death was due to pulmonary hypertension, and one was caused by scleroderma renal crisis. Six patients died from infections probably related to SSc. Three of these had intrinsic lung disease and terminal pneumonia. Peritonitis secondary to intestinal perforation occurred in one case, one died of septicaemia, and one died of meningitis. Most deaths because of causes possibly related to SSc were attributable to lung cancer (n=4) and myocardial infarction (n=2), one patient died of haemolytic anaemia and one of suicide. Of the deaths not considered to be related to SSc five were due to cancer, of breast (n=2), pancreas, liver and uterus, and one died of stroke. The overall standardised mortality ratio was 3.5 and 3.7 for men and women, respectively. The group of patients who died were older at the time of diagnosis (mean age 48.7 years (range 14–74)) than the group as a whole (table 1).
Discussion
This study examined a series of unselected patients with SSc in whom the outcome could be assessed in 100% of cases 14 years after the initial observation. Owing to the gradual onset of the disease as well as to variability in referral practices, the disease onset was estimated to have occurred four to five years before actual inclusion. Thus our study is not informative about very early disease developments. This is common to several other studies.18 ,19 It was possible to identify dermal, pulmonary, cardiac, renal, and gastrointestinal variables with influence on survival. We cannot exclude the possibility that any of the organ involvement variables might have been more sensitive predictors than others in earlier phases of the disease, with the exception of truncal skin involvement.
One important message of the longitudinal observations is the relative stability of organ functions over the observation time. This is not explained by the insensitivity to change of the instrument, but emphasises the fact that in 70–80% of the patients organ damage had already reached a plateau at inclusion. Such data are obviously important for the proper design and evaluation of therapeutic studies. Other investigators have made similar observations.10 ,20 ,21 Nevertheless, negative changes in organ function score were seen in 9–11% of the patients and, with the exception of skin score, these changes also correlated with mortality. We did not explore the potential of a composite organ score, which possibly would have been more sensitive, but would have blurred the distinction between influences from different organ manifestations. Current therapeutic approaches often target individual organ disease owing to a lack of means to influence general disease activity.
The dominating group of patients in our series are women with lSSc. This group has a rather benign disease, with a standardised mortality ratio lower than the group as a whole, but men with lSSc have a standardised mortality ratio not different from that of the general population. Consequently, this group should not as a rule be exposed to therapeutic trials with potentially dangerous drugs. However, the subjects within this group whose disease does progress need to be identified as early as possible. Thus changes in a severity score may be of clinical help, and this hypothesis should be put to the test.
The dominating cause of death in this as in other recent series20-23 is related to pulmonary disease. Therefore it was of particular interest that the severity score for pulmonary disease correlated with outcome and differentiated between the patients with scores of 0–1, 2, and 3–4, respectively. Because treatment of pulmonary fibrosis with cyclophosphamide and similar toxic drugs is increasingly used, it is important to have reliable clinical instruments to select and monitor these patients.
Our data confirm that simple ECG registration can identify patients with early cardiac mortality, although this occurred with low frequency. Thus cardiac exercise tests may not be necessary in routine clinical practice. Distribution of skin involvement is the main distinguishing feature between lSSc and dSSc, and thus of undisputed prognostic value. However, changes in skin involvement in advanced disease are not informative about the disease course in most patients, and we and others24 have recorded the apparent discrepancy between improvement in skin score and worsening of internal organ involvement. In a multicentre study with a follow up of 264 patients with SSc for an average of 5.2 years, Altman et alfound that renal, cardiac, pulmonary, and gastrointestinal disease predicted reduced survival.25 However, data on organ system involvement at study entry could not be used to predict which affected organ system would be the primary cause of death. In another study26 the extent of skin involvement was found to be the determining prognostic factor, together with scleroderma lung disease.
The multicentre severity score approach taken by the European, North American group12 did show that relatively simple and generally available measures could be used to assess disease severity in SSc over a short period. We show the potential of a similar approach when applied to long term outcome. Such instruments will be important tools in future disease modifying treatment of SSc.