Article Text

Abstract
OBJECTIVE To investigate withdrawal from the labour force because of inability to work owing to ankylosing spondylitis (AS) and to determine the characteristics of patients with no job because of work disability attributable to AS.
METHODS A postal questionnaire was sent to 709 patients with AS aged 16–60 years followed up by a rheumatologist. Kaplan-Meier survival statistics were used to assess the time lapse between diagnosis and withdrawal from work. Standardised incidence ratios were calculated to compare withdrawal from the labour force in patients with AS and the general population. Determinants of withdrawal were assessed by Cox's proportional hazard regression analysis using variables assumed to be time independent. Cross sectional characteristics of patients without a job owing to disability were further analysed by simple and multiple regression analyses.
RESULTS A total of 658 patients returned the questionnaire. Of 529 patients with a paid job before diagnosis of AS, 5% had left the labour force within the first year after the diagnosis, 13% after 5 years, 21% after 10 years, 23% after 15 years, and 31% after 20 years. Age and sex adjusted risk for withdrawal was 3.1 (95% CI 2.5 to 3.7) times higher than in the general population. In patients with AS, determinants of withdrawal from work were older age at diagnosis, manual work, and coping strategies characterised by limiting or adapting activities. Patients with work disability at the time of the study were older, came from a lower social class, and were more likely to have total hip replacement, peripheral arthritis, or comorbidity. Moreover, they reported worse physical function (BAS-FI), experienced lower quality of life, and more often had extraspinal disease than those with a job.
CONCLUSION Withdrawal from work is 3.1 times higher in patients with AS than expected in the general population. Within patients, higher age at diagnosis, manual work, and unfavourable coping strategies are important determinants of withdrawal. Patients without a job experience a lower quality of life.
Statistics from Altmetric.com
Ankylosing spondylitis (AS) is a chronic rheumatic disorder with an estimated prevalence of 0.08–0.86%.1 The disease usually starts in the third decade of life and affects men three times as often as women.2 Spinal and extraspinal manifestations may contribute to functional limitations.3 Work disability is an important socioeconomic outcome since it is associated with psychosocial4 and financial5 consequences for patients as well as for society. In a recent cross sectional study we found that age and sex adjusted employment in AS was 11% lower (15% in men, 5% in women) and official work disability was 15% higher (in both sexes) than in the general Dutch population.6 We have undertaken a study of withdrawal from the labour force as a result of AS in patients who had a job before the diagnosis was established. In addition, factors associated with withdrawal and characteristics of patients with work disability attributable to AS were analysed.
Methods
PATIENTS
Patients were selected from the nationwide Dutch Standard Diagnosis Register of Rheumatic Diseases (SDR) in which 37 rheumatology practices (66%) and 80% of all Dutch rheumatologists participated at the time of the study.7 Thirteen regional and two academic practices, geographically spread throughout the country, were invited and agreed to participate. Selected patients had to have a definite diagnosis of AS and to be aged 16–60 years. The estimated total number of patients with AS in the Netherlands is 11 700,8 of whom probably 40–50% are followed up by a rheumatologist, when taking into account the proportion of rheumatologists participating in the SDR and the number of patients with AS in this register.
QUESTIONNAIRE
In September 1997 patients received a postal questionnaire on sociodemographic, disease related, and work related variables. Sociodemographic factors comprised sex, age, race, marital status, family situation, education, profession, income, work status, and conditions at the workplace. Educational level was dichotomised into >12 years and ⩽12 years of formal education. For classification of professions, the Statistics Netherlands Job Classification System was applied.9 Professions were recoded into manual work (jobs in agricultural, industrial, and transport sectors) and non-manual work (jobs in administrative, servicing, and specialist or managerial sectors). Disease related questions assessed age at diagnosis, comorbidity, medication, extraspinal manifestations of AS (inflammatory bowel disease (IBD) and peripheral arthritis), presence of total hip replacement (THR), function measured by the Bath Ankylosing Spondylitis Functional Index (BAS-FI),10 disease activity measured by the Bath Ankylosing Spondylitis Disease Activity Index (BAS-DAI),11 and patient's global well being measured by the Bath Ankylosing Spondylitis Global score (BAS-G).12BAS-FI, BAS-DAI, and BAS-G are scored on a visual analogue scale ranging from 0 to 10. Higher values indicate a worse status. Comorbidity was assessed using a list of 19 comorbid conditions. Peripheral arthritis was defined as having at least one swollen joint indicated on the self-assessment joint score.13 IBD was considered to be present if the patient indicated chronic bowel disease for which he had consulted a specialist within the past 3 months. Coping strategies were assessed by the Coping with Rheumatic Stressors Questionnaire (CORS). This validated questionnaire distinguishes eight coping strategies in patients with rheumatic diseases—three on coping with pain, three on coping with limitations in activities of daily living, and two on coping with dependence.14 The generic health assessment questionnaire RAND-36, which closely resembles the SF-36, was used to assess general health15 ,16 and the Multifactorial Fatigue Index (MFI) was included as a measure of fatigue.17 The presence of psychopathological conditions was measured by the 12-item General Health Questionnaire (GHQ-12) using 3 as the cut off level.18
DEFINITIONS OF END POINTS ON WORK STATUS
In this study work disability is defined as officially recognised inability to perform paid production because of AS. Withdrawal from the labour force refers to those who had a paid job before diagnosis of the disease and had to leave their job completely because of AS related work disability. In the Netherlands the Social Security Association decides on eligibility for work disability payments after 1 year of continuous sick leave. Six categories of work disability are distinguished. Disability of 80–100% is regarded as full, while the other categories are considered as partial work disability. In cases where the disability exceeds 15%, a benefit is allowed incrementally ranging from 25% to 70% of the former gross wage. Benefits are financed through social contributions from employees and employers. Patients with partial work disability can continue in part time jobs. In 1993 disability criteria changed in the Netherlands to reduce the work disability rates. Before 1993 work disability payments were allowed if a person could not perform his or her profession because of medical restrictions, taking into account age and unemployment figures in the region where the person was living. Since 1993 work disability payments are allowed if there are objective medical restrictions to earn the wage of one's present job, independent of age. In addition, the method to calculate the disability benefit changed and the period of attributed disability was restricted to a maximum of 5 years.
STATISTICS
Kaplan-Meier analysis was applied to patients with a paid job before diagnosis of AS. Leaving the labour force completely because of AS related work disability was considered an event. Patients who received partial work disability benefit but continued to work were not considered to have an event and patients who had left the labour force for reasons other than AS were censored. The risk for withdrawal from the labour force in patients with AS was compared with that of the general population by calculating standardised risk ratios (SRR) for five age categories in men and women separately, using incidence rates of complete work disability benefits in the general Dutch population in 1998 (Dutch Central Bureau of Statistics, unpublished data). Determinants of withdrawal from the labour force were assessed using Cox's proportional hazard regression analysis with backward elimination according to the likelihood ratio test (probability for removal = 0.1), with age at diagnosis of disease (dichotomised at ⩾35 years), sex, educational level, profession, and the eight coping strategies as covariates. To assess the influence of the change in work disability criteria in 1993, a time dependent Cox regression was performed with number of years working while suffering from AS before or after 1993 as the time dependent covariate. Possible interactions between the four variables of the final model were assessed in a new Cox's proportional hazard regression, forcing the main effects into the model and selecting all possible interactions by backward elimination. Finally, using the Cox regression equation, three subgroups of patients with different risks for withdrawal from the labour force were formed and Kaplan-Meier survival statistics were computed for each group.
To assess the characteristics of those with work disability at the time of the survey, we first compared the characteristics of patients in each of the following three groups: (1) those having a job without disability, (2) those having a (part time) job and (partial) work disability, and (3) those having work disability but no job. We then compared those having a job without disability with those having work disability and no paid job. The differences between the groups were analysed univariately by the t test, χ2 test, and by multiple logistic regression with backward elimination according to the likelihood ratio test. Interactions between the variables of the final regression model were sought. Finally, the contribution of work disability to variations in BAS-FI, BAS-DAI, BAS-G, RAND-36, GHQ, and MFI was analysed in multiple linear regressions while controlling for demographic (age, sex, and social class) and disease characteristics (disease duration, extraspinal disease, and comorbidity). Statistical tests were performed using SPSS 9.0.
Results
RESPONSE
A total of 1092 patients with AS from the 15 rheumatology practices were sampled. The current postal address of 152 patients could not be retrieved. Of the 940 remaining patients, 709 agreed to participate and received the questionnaire which was completed by 658 patients. This accounts for a response rate of 70.0%. Non-participants did not differ in age and sex from participants. The results of labour force participation and work disability have been described in detail elsewhere.6
WITHDRAWAL FROM LABOUR FORCE
Five hundred and twenty nine of the 658 patients (80.4%) had a paid job before diagnosis of AS. The mean (SD) age at diagnosis was 32.7 (8.6) years, mean disease duration at the time of the study was 12.0 (7.8) years, and 71% were men. After adjusting for age and sex, 79% followed formal education for ⩽12 years compared with 74% in the general Dutch population and 24% performed a manual job compared with 18% in the general Dutch population. Furthermore, 24.0% had peripheral arthritis, 3.4% had IBD, 3.2% had undergone THR, 40.6% had a comorbid condition, and 82.8% currently used NSAIDs. To ascertain that the type of profession was stable over time we analysed change of profession in a subgroup of 85 patients who took part in a more extensive follow up study. Seven patients (8.2%) changed profession because of AS. In two (2.4%) this was a change from a manual to a non-manual profession.
In the total group, 123 patients left the labour force because of AS related work disability and 59 patients left the labour force for other reasons. Kaplan-Meier survival statistics (nine excluded because of missing data) showed that withdrawal from the labour force because of AS related work disability was 5% during the first year after diagnosis, 13% after 5 years, 21% after 10 years, 23% after 15 years, and 31% after 20 years. Age and sex adjusted risk to withdraw from work was 3.1 (95% CI 2.5 to 3.7) times higher than that of the general Dutch population. This was more pronounced for younger than for older patients (table 1) and tended to be more important in male than in female patients with AS. However, the sex difference has to be interpreted with caution because of the low number of observations in women. The change in disability criteria in the Netherlands in 1993 had no statistically significant influence on the withdrawal rate as shown by time dependent Cox regression (p=0.47). Table 2 shows determinants of withdrawal as assessed by Cox's proportional hazard regression analysis. Older age at diagnosis, manual work, and two specific coping strategies but not sex and educational level were associated with withdrawal from the labour force. Figure 1 illustrates the influence of these factors on the Kaplan-Meier survival curves; no interactions were seen.
Age and sex adjusted risk ratios (95% CI) for withdrawal from labour force in ankylosing spondylitis (AS) compared with the general Dutch population
Variables associated with withdrawal from labour force because of ankylosing spondylitis (AS) related work disability, assessed by Cox’s proportional hazard regression analysis
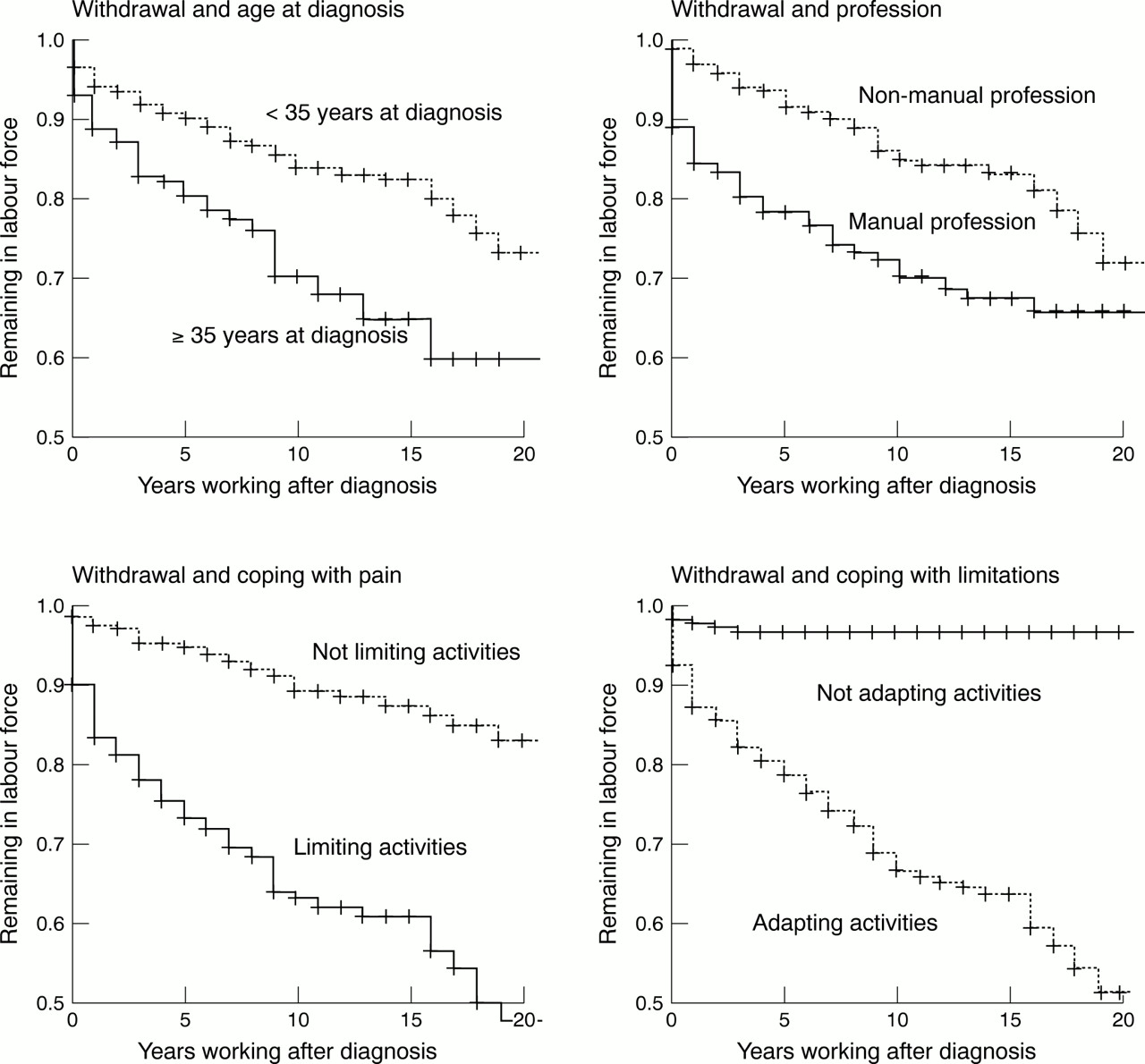
Kaplan-Meier curves illustrating probability to remain in the labour force for each of the risk factors in the Cox regression analysis.
Three different groups at risk for withdrawal from the labour force could be distinguished according to the Cox regression equation. The first group with high risk for withdrawal (36% of patients) had both unfavourable coping strategies (limiting activities when faced with pain and reducing activities when faced with limitations). The second group with low risk for withdrawal (38% of patients) had both favourable coping strategies (not limiting activities when faced with pain and not reducing activities when faced with limitations) and the group with intermediate risk for withdrawal (26% of patients) had one of two unfavourable coping strategies. The Kaplan-Meier survival curves of these three risk groups are shown in fig 2.

{kind=link}
{kind=link}
Kaplan-Meier curves illustrating withdrawal from the labour force for three different risk groups of patients with AS.
CHARACTERISTICS OF WORK DISABLED PATIENTS
At the time of the study, 338 of the 658 patients had a paid job without work disability, 83 patients had a (part-time) job and (partial) work disability, and 136 had work disability but no job. In addition, 27 patients had never had a job and 110 patients had left the labour force but for reasons other than AS related work disability. The sociodemographic and disease characteristics of the three groups with a job and/or work disability are compared in table 3. Older age, longer disease duration, lower social class (educational level and type of job), presence of comorbidity, extraspinal disease (IBD and peripheral arthritis), and THR were characteristics of patients without a job. In multiple logistic regression analysis, patients with a job but no work disability were compared with those who had left the labour force because of work disability. The result of the multiple logistic regression analysis with age, sex, disease duration, education, profession, comorbidity, THR, and extraspinal disease (IBD and peripheral arthritis) are presented in table 4. Sex, disease duration, and IBD were eliminated as independent discriminators. Having a THR was highly associated with being work disabled. No interactions were found between the variables of the final model. The group without a job because of work disability reported an increased frequency of psychopathology (GHQ-12), worse physical function (BAS-FI), higher disease activity (BAS-DAI), worse perceived health (BAS-G and RAND-36), and higher levels of fatigue (MFI) (table 5). Also, when adjustments were made for differences in demographic characteristics, comorbidity, THR and extraspinal disease, work disability remained significantly associated with each of these outcome variables (data not shown separately). Patients still at work reported no more adaptations at the workplace than those with work disability in their last job.
Characteristics of patients with ankylosing spondylitis (AS) who have a job (without work disability) compared with those with a part time job and partial work disability and those with work disability without a job
Multiple logistic regression analysis with sociodemographic (age, sex, education, and profession) and disease related variables (disease duration, inflammatory bowel disease, peripheral arthritis, and total hip replacement) to asssess characteristics of work disabled patients with ankylosing spondylitis (AS) (n=136) compared with patients with AS having a paid job without work disability (n=338) at the time of the survey
Simple regression analyses to compare patients with ankylosing spondylitis (AS) having a job without disability with those with work disability without a job
Discussion
The risk of withdrawal from work because of AS related work disability increases steadily over time resulting in one third of patients having left the labour force after 20 years of disease. Comparison of withdrawal rates with those of the general population shows a threefold increased risk of leaving the labour force for patients with AS.
It should be stressed that we studied only withdrawal due to official work disability. It is possible that some patients left the labour force because of AS but did not receive official work disability benefit. There may therefore be hidden work disability, especially in women. Moreover, only complete withdrawal from the labour force was studied. Patients can receive partial work disability benefit while continuing in a (part time) job. Total withdrawal rates may therefore be higher than withdrawal rates because of complete official work disability.19
Despite the retrospective design of our study, we think survival analysis can be performed meaningfully, although the results have to be interpreted with some caution. Several types of selection bias should be considered. Firstly, in the Netherlands only 40–50% of patients with AS are followed up by a rheumatologist. It has been shown that hospital sampled patients have somewhat more severe disease and more often suffer work disability than population sampled patients with AS.20 This would result in overestimation of the withdrawal rate. Secondly, if patients with more severe disease have higher mortality, they might not have been sampled in our retrospective study and this would have resulted in underestimation of the withdrawal rate. Since mortality from AS seems only slightly increased,21 it is unlikely this will have influenced our patient population considerably. Thirdly, it can be argued that patients with problems at the workplace are more likely to consult a rheumatologist which might have inflated the observed withdrawal rate. However, in The Netherlands the rheumatologist has only a minor role in decisions on eligibility for work disability, reducing the chance that those patients with difficulties at the workplace more often consult a rheumatologist. Apart from selection bias, the change in disability criteria in the Netherlands in 1993 posed an additional problem in our retrospective study. A time dependent Cox analysis showed that this change had no measurable influence on the withdrawal rate for patients with AS. Furthermore, given the design of this study, variables to assess determinants of withdrawal were selected carefully. Age at diagnosis, sex, education, type of profession, and coping strategies,22 although assessed at the time of the survey, are unlikely to have changed after diagnosis of disease and therefore can be used in predictive models. However, information on peripheral arthritis, THR, IBD, comorbidity, disease activity and severity, and quality of life was only available for the time of the survey and could therefore not be used to analyse predictors for work disability in this retrospective study.
The withdrawal rate in our population was slightly lower than in both a Mexican prospective study (n=103) in which a withdrawal rate of 15% was observed after 5 years in patients with a mean disease duration of 10 years,23 and a French longitudinal study (n=186) which reported a cumulative withdrawal of 36% after 20 years of disease.24 A Finnish inception cohort (n=76) showed lower withdrawal rates in the first years of the disease (5% after 10 years), but equal withdrawal after longer disease duration (30% after 25 years).25 These studies did not explicitly state whether or not they assessed AS attributable withdrawal while we specifically studied withdrawal because of AS. This difference might contribute to our somewhat more favourable results. In addition, the French cohort included only patients admitted to hospital and might have dealt with more severe disease. On the other hand, a very low withdrawal rate owing to AS related work disability of 13.2% after a median of 21.4 years of disease was reported in a recent US study on 234 patients.19 Compared with our patients, the proportion having a job as a professional/manager was higher. We can only speculate on the contribution of differences in the social security systems.
As in the French and US cohorts, we found that the type of job was associated with withdrawal from work.19 ,24 Interestingly, in our study two behavioural coping strategies were strongly associated with leaving the labour force—namely, coping with pain by limiting activities and coping with limitations by adapting activities. Coping strategies and their influence on outcome have not yet been thoroughly investigated in AS. Coping measured by the CORS, an arthritis specific coping scale, is considered a personality trait of individuals22 and therefore stable over time. In other musculoskeletal diseases it has been shown that coping strategies are associated with the amount of pain experienced, level of physical functioning, disease activity, and quality of life.26 ,27To our knowledge, this is the first time that coping strategies have been found to be associated with withdrawal from the labour force in musculoskeletal disease. It is clear that unfavourable coping strategies, in the same way as manual professions, may be disease independent risk factors for withdrawal. However, no data are currently available from the general population or other diseases to analyse this issue in more depth.
This study demonstrates the importance of analysing withdrawal from the labour force not only in patients with AS but also in comparison with the general population. Higher age was positively associated with withdrawal within the AS group but negatively associated with withdrawal when compared with the general population.
Withdrawal rates in AS seem lower than in rheumatoid arthritis (RA). Studies in patients with RA published within the last 5 years which have investigated withdrawal from the labour force among patients with a paid job have shown that withdrawal rates are higher than 30% after 10 years of disease while in studies in patients with AS withdrawal rates of 30% are only seen after 20 years.28-34 In a case-control cohort study in the UK the odds ratio to become economically inactive was 32.0 (95% CI 5.4 to 1303) for patients with RA compared with controls, which is about 10 times higher than in our study.34 In RA, as in AS, higher age at onset of disease, lower social class, higher disease activity, and worse physical function were associated with withdrawal from work in several of these studies.29-32 ,34
When patients with a job at the time of the survey were compared with those with work disability, work disabled patients were older, from a lower social class, with comorbidity, peripheral arthritis, and most had THR. Notably, sex, disease duration, and IBD were not independent characteristics. Work disability was significantly associated with worse quality of life (RAND-36), higher levels of fatigue (MFI), and the presence of psychopathology (GHQ), independent of age, sex, disease duration, comorbidity, THR, and peripheral arthritis. Again, the retrospective study design does not allow us to conclude that patients who become work disabled will lose quality of life or are likely to develop a psychopathological condition. Indeed, the reverse could be true. Prospective studies in other chronic diseases suggest that loss of work results in worse perceived health.4 Patients still working did not report adaptations in the workplace more often than those who had left employment in their last job.
Several cross sectional studies of AS reported in the literature found that higher age, lower education, and worse physical function are associated with present work disability.35-37 One other study also concluded that patients without employment more often report depression.35 In contrast to our findings, a Norwegian study of 99 patients showed that female sex, but not peripheral arthritis, THR, or the presence of a psychopathological condition (GHQ), were associated with inability to work.37Comparison of data on work status from different countries is, however, difficult. Demographic and disease characteristics can vary, and changes in the local labour market or differences in the social security systems can pose varying incentives to leave or remain in the labour force.
In conclusion, withdrawal from the labour force in AS is substantial. Coping strategies may contribute to withdrawal. Work disabled patients with AS report a worse quality of life. This aspect should not be neglected in any holistic approach of the patient.
Acknowledgments
We gratefully thank all rheumatologists from the following centres who participate in the SDR and took part in this study: Sint Antoniusziekenhuis Nieuwegein, Rode Kruisziekenhuis Den Haag, Bosch Medicentrum Den Bosch, Sint Laurentiusziekenhuis Roermond, Sint Jansgasthuis Weert, Groene Hartziekenhuis Gouda, Albert Schweitzerziekenhuis Dordrecht, Kennemer Gasthuis locatie Deo Haarlem, Lievensberg Ziekenhuis Bergen op Zoom, Tweesteden Ziekenhuis Tilburg, Rijnstate Ziekenhuis Arnhem, St Maartenskliniek Nijmegen, Medisch Spectrum Twente Enschede.