Article Text

Abstract
Biological agents targeting tumour necrosis factor (TNF) have revolutionised the treatment of rheumatoid arthritis (RA) and clinical remission has become a realistic treatment goal. Discontinuing anti-TNF therapy after sustained remission has emerged as an important area of investigation in rheumatology from the risk-benefit point of view, including health economic considerations. However, there is little information as to whether ‘biologic-free remission’ is possible after sustained remission following intensive treatment with TNF inhibitors in RA. European studies such as BeSt and OPTIMA in patients with early RA and Japanese studies such as remission induction by remicade in patients with RA and HONOR in patients with long-standing RA encountered during routine clinical practice have shown that, after a reduction in disease activity to clinical remission or low disease activity by infliximab or adalimumab in combination with methotrexate, patients can successfully remain in clinical remission without TNF inhibitors with no radiological and functional damage progression of articular destruction. Experimental findings in TNF-deficient mouse models suggest that TNF inhibitors may change the disease process of RA and bring about the potential of immunological remission, raising the possibility of a ‘treatment holiday’ of TNF inhibitors after intensive treatment.
- Rheumatoid Arthritis
- TNF-alpha
- Treatment
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is a systemic inflammatory disease that causes significant morbidity and mortality.1–4 It is recommended that the treatment of RA is initiated with monotherapy or a combination of disease-modifying antirheumatic drugs (DMARDs).5–8 Patients with active RA, however, are often resistant to DMARD therapy, especially in the context of structural progression. Thus, biological agents targeting proinflammatory cytokines such as tumour necrosis factor (TNF), which plays a pivotal role in the pathological processes of RA leading to joint destruction, have been developed. The combined use of biological agents targeting TNF and methotrexate (MTX) has revolutionised the treatment of RA, producing significant improvements in clinical, structural and functional outcomes that were not previously observed. Accordingly, the concept of treating RA to target by employing a composite measure of disease activity is generally being accepted worldwide.5 Clinical remission is perceived as an appropriate and realistic primary goal in many patients while, in those with long-standing RA, low disease activity is the aim.
After the induction of clinical remission by combination therapy with TNF inhibitors and MTX, it has to be maintained as described in No. 8 of the ‘Treat-to-Target’, which leads to structural remission and functional remission.5 Caution is needed when deciding to reduce or discontinue treatment with synthetic DMARDs because stopping DMARDs in remission was followed by twice as many flare-ups, difficulties in reintroducing remission and a halt in damage, whereas similar studies are not available for the biological agents.5 However, because of the economic burden associated with expensive biological products and the long-term safety by inhibiting a particular cytokine, the possibility of discontinuation of biological products after the maintenance of remission needs to considered. Thus, treatment strategies with TNF inhibitors targeting induction and/or maintenance of clinical remission can potentially lead to subsequent discontinuation of the TNF inhibitors. However, there is no well-established firm evidence that remission can be sustained even if a biological agent is discontinued (ie, ‘biologic-free remission’). In this paper we discuss whether the discontinuation of TNF inhibitors such as adalimumab and infliximab is possible in patients with RA after achieving low disease activity or clinical remission during a certain period with TNF inhibitors.
Is discontinuation of adalimumab possible after sustained remission?
Clinical remission has recently become an achievable goal by the combination therapy of TNF inhibitors and MTX in many patients, and appropriate induction of remission is a prerequisite to halt joint damage and functional disabilities, which revealed improved outcomes with strategic therapeutic approaches.4–8 If a patient is in persistent remission after tapering of glucocorticoids, one can consider tapering TNF inhibitors, especially if this treatment is combined with DMARDs. However, there is little information about the characteristics of patients with long-standing RA in whom adalimumab can be successfully discontinued.
We have carried out a study (Humira discontinuation without functional and radiographic damage progressiON follOwing sustained Remission, HONOR) to investigate whether adalimumab-free remission is maintained after discontinuation of adalimumab in Japanese patients with established RA in sustained remission obtained with adalimumab plus MTX.9 In this study, sustained remission was defined as a persistent Disease Activity Score 28 (DAS28)-erythrocyte sedimentation rate (ESR) of < 2.6 for at least 6 months. Informed consent was obtained from patients aged >18 years who had attained sustained remission with adalimumab plus MTX to discontinue adalimumab and those followed up for >6 months were evaluated. The primary endpoint was the proportion of patients who maintained sustained remission for at least another 6 months after discontinuation. DAS28, simplified disease activity index (SDAI), clinical DAI, health assessment questionnaire-disability index (HAQ-DI) and yearly progression of the modified total Sharp score (ΔmTSS) were assessed before and after discontinuation of adalimumab. To predict retaining adalimumab even after withdrawing it, a logistic regression and receiver-operating characteristic analysis were conducted on clinical variables and cut-off values at discontinuation were determined.
Of the 197 patients who started adalimumab treatment between July 2008 and April 2011 in our department, 69 (35.0%) met the criteria for sustained remission and 51 consented to enter the study. The mean age of the 51 patients was 59.5 years and mean disease duration was 7.1 years, indicating that the population included patients with long-established disease. The mean DAS28-ESR score was 5.1, implying that most patients had active disease despite MTX. Furthermore, because the mean ΔmTSS was 11.5, the addition of TNF inhibitors to MTX was needed to control joint destruction as well as disease activity. Fifty-eight percent of the evaluable 50 patients maintained adalimumab-free remission at 6 months. DAS28-ESR at discontinuation was found significantly to predict the retention of remission with a cut-off value of 2.16. Most patients (94.9%) showed no evidence of radiographic progression (ΔmTSS ≤ 0.5) at 1 year. Moreover, HAQ-DI observed at the time of adalimumab discontinuation was almost preserved at 6 months. Therefore, although the sample size is limited, the results of the HONOR study indicated that, after reaching remission with adalimumab plus MTX, most patients could discontinue adalimumab for more than 6 months without disease flare, functional impairment and radiographic damage progression. Also, deep remission at discontinuation was associated with successful biologic-free remission.
Recently, a multinational double-blind randomised controlled study was performed to determine the optimal protocol for treatment initiation with adalimumab plus MTX in patients with early RA (OPTIMA).10 Outcomes of withdrawal or continuation of adalimumab were assessed in patients who achieved a stable low disease activity target after 26 weeks of initially assigned treatment with adalimumab and MTX. Of the 466 patients with RA treated with adalimumab plus MTX, 207 (44%) achieved stable low disease activity and were re-randomised to placebo or adalimumab plus MTX. At week 78, 86% and 66% of patients treated with adalimumab plus MTX and placebo plus MTX, respectively, achieved DAS28 remission (<2.6). SDAI remission and ΔmTSS remission were comparable for both groups.
Another trial conducted in Germany (HIT HARD) addressed the question of whether early induction therapy with a subsequent step-down strategy leads to a long-term clinical effect in patients with recent onset RA compared with initial and continued MTX monotherapy.11 During the first 24 weeks, 172 patients were treated with adalimumab or placebo plus MTX and, after week 24, both groups were treated with MTX alone for 24 weeks. During the induction phase 47.9% of patients treated with MTX plus adalimumab achieved DAS28 remission and, at week 48, 42.4% were still in remission with 24 weeks of adalimumab-free treatment.
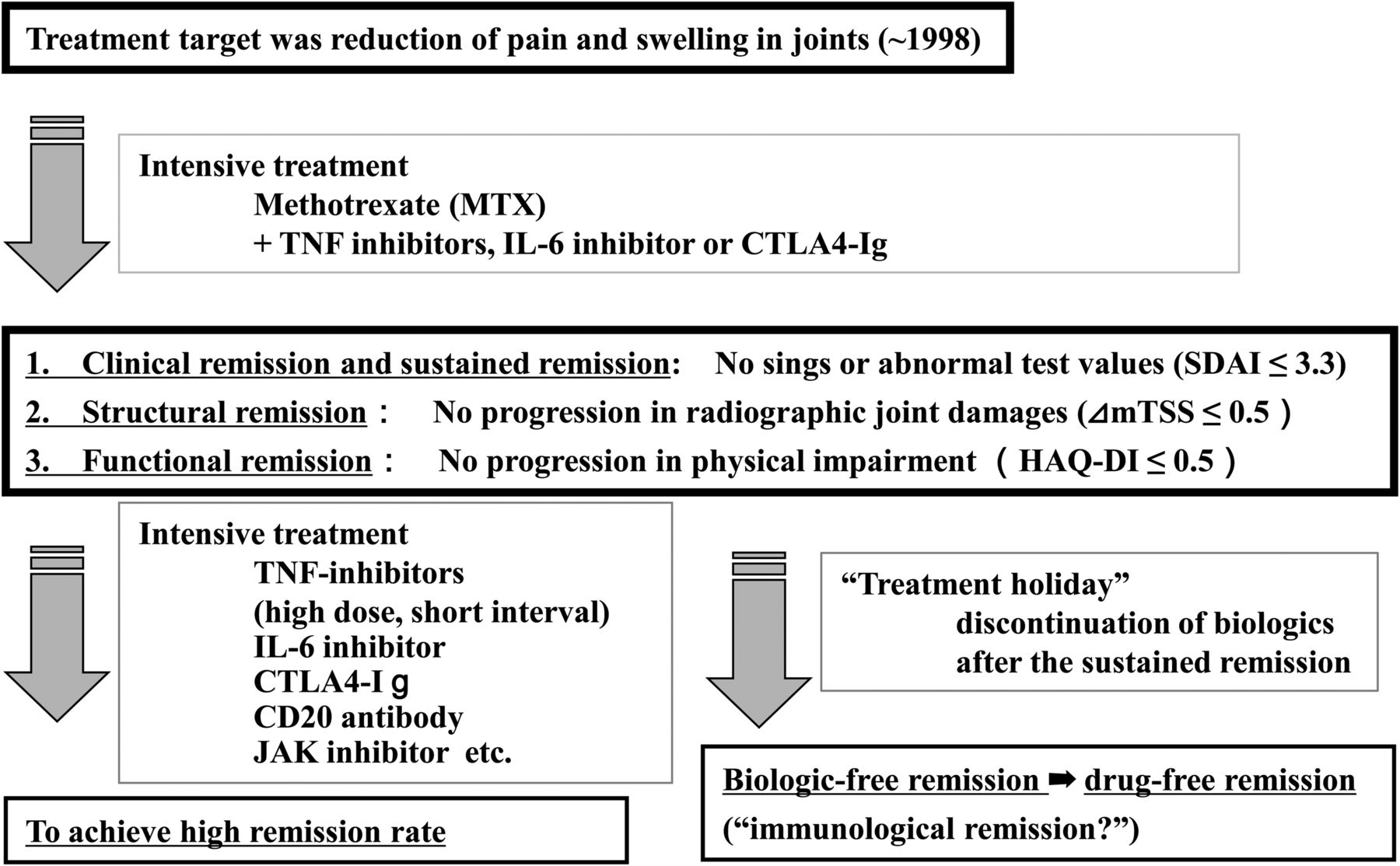
In the OPTIMA and HIT HARD trials, early induction therapy with adalimumab and MTX followed by withdrawal of adalimumab led to a loss of the response gained with the initial combination treatment in a subgroup of patients, but not in all patients. Unlike the HONOR study, among patients with early RA such as those in both studies, some might be capable of comprehensive disease control with initial and continued MTX monotherapy. However, the results of the HONOR study indicate that a ‘treatment holiday’ of biological agents by discontinuing adalimumab is now feasible in patients with RA following sustained remission, even in patients with long-standing RA encountered during routine clinical practice (figure 1).
{kind=link}
The next stage of the treatment of rheumatoid arthritis: intensive treatment and the possibility of a ‘treatment holiday’. IL, interleukin; TNF, tumour necrosis factor.
Is discontinuation of infliximab possible after sustained low disease activity?
We also conducted a study (Remission induction by Remicade in RA patients, RRR) to examine the possibility of biologic-free remission or low disease activity in patients with RA whose mean disease duration was 5.9 years.12 This study included a total of 114 patients with RA from 26 centres. The mean DAS28-ESR score was 5.6, implying that most patients had active disease despite MTX therapy. Furthermore, because the mean ΔmTSS was approximately 14, the addition of TNF inhibitors to MTX was needed to control disease activity and joint destruction. The patients enrolled in the study were those who had reached and maintained low disease activity (DAS28<3.2) for more than 24 weeks with infliximab treatment and who then agreed to discontinue the treatment. Among the 102 evaluable patients who completed the study, 56 (55%) maintained low disease activity after 1 year and showed no progression in radiological damage and functional disturbance, and 44 (43%) remained in clinical remission (DAS28<2.6). The mean disease duration of the group who achieved remission or low disease activity in the RRR study was 4.8±5.9 years, which made this study the first to prove that patients with long disease duration may also aim for discontinuation. Furthermore, ΔmTSS≤0.5 was observed in 67% and the HAQ-DI score was only 0.174 in patients who maintained a low disease activity for 1 year after discontinuation. We therefore conclude that more than half of patients who maintain a low disease state for more than 24 weeks on infliximab can discontinue infliximab and maintain low disease activity for a year without radiographic or functional disease progression.
The possibility of biologic-free remission in patients with RA was initially reported by a TNF20 study.13 The combination of infliximab and MTX in patients with early RA who had symptoms for <12 months provided tight control of the disease activity. Although infliximab was withdrawn at 1 year, low clinical activity and functional abilities were sustained for another year. In the Netherlands, the Behandelstrategieën (BeSt) study was conducted to compare four treatment strategies and to observe clinical outcomes in patients with early RA (disease duration <2 years after onset, mean disease duration 0.8 years).14–16 In this study, 508 patients with high disease activity were allocated to four groups and evaluated by DAS44 every 3 months. In patients with DAS44>2.4 (intermediate or high disease activity) a change or addition of medications was required, in those with DAS44≤2.4 (remission or low disease activity) the current medication was continued and, in patients with DAS44≤2.4 continued over 6 months, concomitant medications including infliximab were decreased and/or discontinued. In the fourth group who started infliximab, 90 of 120 patients (75%) achieved DAS44≤2.4 and infliximab was withdrawn in 77 cases because DAS44≤2.4 was maintained for 6 months. In the fourth group started with MTX and infliximab, the total cost of work loss and medical expenses was less than half that of the other groups started with DMARDs.
The biggest difference between the patient populations in the RRR and BeSt studies was disease duration (mean disease duration 0.8 years in the BeSt study vs 5.9 years in the RRR study), implying that biologic-free remission is possible in patients with early onset RA and also in those with long-established disease. It remains unclear whether discontinuation of biological agents targeting TNF is beneficial for comorbidity such as increased cardiovascular and/or cerebrovascular events. Since nearly a decade has passed since the BeSt study was initiated, some answers to this query may be drawn from the study.
Is TNF involved in the disease processes?
In the BeSt study, 58% of 120 patients discontinued infliximab and 19% of patients have discontinued all DMARDs and remained in clinical remission with minimal joint damage progression 5 years after receiving infliximab and MTX as initial treatment for RA, suggesting the possibility of treatment-free remission.
In our institution, among 577 patients who were treated with infliximab, 88 patients reached biologic-free remission and only five are currently in drug-free remission without MTX. Although both TNF inhibitors and MTX play a role in the treatment, our data suggest that discontinuation of MTX appears to be difficult in patients with long-established RA. The mode of action of MTX is not discussed here, but its continuation is needed as a standard key drug. Discontinuation of biological agents benefits the economic burden of long-term management.
Accumulated studies indicate the involvement of TNF in the disease process in animal arthritis models, especially at the early stages of joint inflammation. Introduction of TNF transgene into the mouse results in typical polyarthritis, with hyperplasia of the synovium, inflammatory infiltrates in the joint space, pannus formation and cartilage and bone destruction. However, the polyarthritis and joint destruction obtained were completely ameliorated by the preventive as well as curative application of TNF inhibitors.17 Meanwhile, TNF deficiency reduced the incidence of autoimmune arthritis in most models.18–20 For instance, K/BxN is a model of arthritis which expresses both T cell receptor (TCR) transgene KRN and the MHC class II molecule Ag7. In the mouse, TCR recognises a self-antigen glucose-6-phosphate isomerase (GPI) and produces anti-GPI antibody, and arthritis is induced by the injection of the serum to naïve mice. Although TNF is highly expressed in K/BxN mice, deficiency of the TNF gene markedly reduced both the incidence and severity of the autoimmune arthritis. SKG is also an inflammatory arthritis model with a point mutation of ZAP-70, a member of spleen tyrosine kinase (Syk) associated with the TCRζ chain. The knockout mutation of the TNF gene in SKG mice showed amelioration of both the incidence and the severity of the arthritis.
If animal data partially reflect the efficacy of TNF inhibitors in patients with RA, it suggests that TNF inhibitors may change the disease course or induce immunological remission in RA. Interestingly, 48% of the 577 patients with RA described became negative for rheumatoid factor (RF) when infliximab was discontinued, although 77% of them were positive for RF at baseline when infliximab was initiated. Although the studies are limited, when the disease course is successfully changed by intensive treatment including the combination of MTX and TNF inhibitors, patients with RA may have the possibility of a ‘treatment holiday’ of TNF inhibitors.
Conclusions
Although the studies are limited, after reduction of disease activity to clinical remission by TNF inhibitors such as infliximab and adalimumab in combination with MTX, patients may be able to discontinue TNF inhibitors without clinical flare, radiographic progression of articular destruction and functional impairment. A ‘treatment holiday’ of biological agents is possible in patients with early RA and also in those with long-established RA. It has to be realised that intensive treatment with a TNF inhibitor is required to bring about the ‘treatment holiday’ efficiently since deep remission was a major factor affecting the success of discontinuation of TNF inhibitors in two Japanese studies. Discontinuation of biological agents during treatment of RA has become an important area of investigation in rheumatology patients and governments from the risk-benefit viewpoint including health economic considerations. Meanwhile, because treatment with TNF inhibitors can bring about the induction of remission, sustained remission and subsequent biologic-free remission—that is, it may change or modify the course of the disease—a clinical and basic research approach to the ‘process-driven disease course’ of RA is warranted from wider standpoints, leading to the elucidation of pathological mechanisms and treatment strategies.
Acknowledgments
The author thanks all medical staff in all institutions for providing the data.
References
Footnotes
-
Funding The series of studies were also supported in part by a Research Grant-In-Aid for Scientific Research by the Ministry of Health, Labor and Welfare of Japan, the Ministry of Education, Culture, Sports, Science and Technology of Japan and the University of Occupational and Environmental Health, Japan.
Competing interests YT has received consulting fees, speaking fees and/or honoraria from Mitsubishi-Tanabe Pharma Corporation, Abbott Japan, Eisai, Chugai Pharmaceutical, Janssen Pharmaceutical, Santen Pharmaceutical, Pfizer Japan, Astellas Pharma, Daiichi-Sankyo, GlaxoSmithKline, Astra-Zeneca, Otsuka Pharmaceutical, Actelion Pharmaceuticals Japan, Eli Lilly Japan, Nippon Kayaku, UCB Japan, Quintiles Transnational Japan, Ono Pharmaceutical and Novartis Pharma and has received research grants from Bristol-Myers Squibb, MSD, Chugai Pharmaceutical, Mitsubishi-Tanabe Pharma Corporation, Astellas Pharma, Abbott Japan, Eisai and Janssen Pharmaceutical.
Provenance and peer review Commissioned; externally peer reviewed.