Article Text

Abstract
Background: There is currently no universal consensus on nomenclature for spondyloarthropathy (SpA), or on activity and severity criteria for ankylosing spondylitis (AS).
Method: Points of agreement and majority opinions among 28 international experts in the field were identified by questionnaire. Agreement was defined as >80% concurrence, clear majority as >60% concurrence, and a majority or trend as >50% concurrence.
Results: Respondents agreed on the need for one term that reflects the inflammatory nature of the disease, but no agreement was reached on a specific term. Agreement included subdivision of patients with SpA into AS, psoriatic arthritis, inflammatory bowel disease associated arthritis, and undifferentiated spondyloarthritis/spondyloarthropathy. A majority of experts defined active disease as fulfilling classification criteria for AS and/or a SpA, and disease activity measured by a Bath AS Disease Activity Index (BASDAI) score >4 determined by two patient visits during a two month period, but no maximum radiographic score. The majority of participants considered failure of treatment response to non-steroidal anti-inflammatory drugs (NSAIDs) alone to be a prerequisite for active/severe AS, and 15/28 (54%) thought that NSAID treatment failure should be defined as lack of response to two or more NSAIDs.
Conclusions: Respondents agreed that a two to five year study is the ethical method to demonstrate effects of anti-tumour necrosis factor α (TNFα) therapy on radiographic progression of AS, and that inclusion criteria should include a certain level of disease activity (measured by BASDAI) and failure of certain treatments. After the efficacy of anti-TNFα therapy in AS and psoriatic arthritis is proved, respondents agreed that more studies will be needed to show efficacy for other SpA subsets.
- ankylosing spondylitis
- spondyloarthropathy
- spondyloarthritis
- tumour necrosis factor α
- AS, ankylosing spondylitis
- ASAS, Ankylosing Spondylitis Assessment (Working Group)
- BASDAI, Bath AS Disease Activity Index
- BASFI, Bath AS Functional Index
- BASRI, Bath AS Radiological Index
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- ESSG, European Spondylarthropathy Study Group
- IBD-A, inflammatory bowel disease related arthritis
- MRI, magnetic resonance imaging
- NSAIDs, non-steroidal anti-inflammatory drugs
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- ReA, reactive arthritis
- SpA, spondyloarthropathy
- TNFα, tumour necrosis factor α
- uSpA, undifferentiated spondyloarthropathy
Statistics from Altmetric.com
- AS, ankylosing spondylitis
- ASAS, Ankylosing Spondylitis Assessment (Working Group)
- BASDAI, Bath AS Disease Activity Index
- BASFI, Bath AS Functional Index
- BASRI, Bath AS Radiological Index
- CRP, C reactive protein
- DMARDs, disease modifying antirheumatic drugs
- ESSG, European Spondylarthropathy Study Group
- IBD-A, inflammatory bowel disease related arthritis
- MRI, magnetic resonance imaging
- NSAIDs, non-steroidal anti-inflammatory drugs
- PsA, psoriatic arthritis
- RA, rheumatoid arthritis
- ReA, reactive arthritis
- SpA, spondyloarthropathy
- TNFα, tumour necrosis factor α
- uSpA, undifferentiated spondyloarthropathy
With the advent of new biological treatment options for ankylosing spondylitis (AS), such as the anti-tumour necrosis factor α (TNFα) agents, there is a fundamental need to establish universal standards for nomenclature, disease classification, and assessment of treatment outcome, if the precise role of these agents in disease management is to be defined. Uniformity in these areas will facilitate global communication of scientific, clinical, and epidemiological information that can further the understanding of the pathogenesis and treatment of the disease. Disease classification is particularly important in clinical practice because it guides treatment strategy and helps to predict response to treatment and prognosis. Additionally, standardisation of scientific terminology and treatment assessments will enable investigators to design clinical trials with the intention of producing conclusive and reproducible end points that have clinical application in well defined patient populations. Furthermore, such trials will allow valid comparisons of therapeutic outcomes.
AS belongs to a group of interrelated inflammatory arthropathies sharing clinical and genetic (that is, association with human leucocyte antigen (HLA)-B27) characteristics that differentiate them from rheumatoid arthritis (RA).1 The term “spondyloarthropathy” (SpA) was coined to describe this group of diseases.2,3 Other arthropathies included in this family include reactive arthritis (ReA), psoriatic arthritis (PsA), inflammatory bowel disease related arthritis (IBD-A), and undifferentiated SpA (uSpA). Criteria for the classification of SpAs developed by the European Spondylarthropathy Study Group (ESSG) (table 1) have been widely used.2 Categorisation of individual patients into each subset of SpA, however, can be difficult because of symptom overlap and the lack of well defined criteria for disease diagnosis and classification.1,4 The report of a recent international workshop on ReA exemplifies these difficulties.4
Criteria for classification of spondyloarthropathy developed by the European Spondylarthropathy Study Group (ESSG)2
AS is considered the prototype of the SpAs2 and the most frequently occurring form of SpA, followed by uSpA.5 Difficulty in reaching consensus for AS terminology and classification dates back to the earliest descriptions of the disease by Wladimir von Bechterew in 1893, Adolph Stuempell in 1894, and Pierre Marie in 1898. These early rheumatologists described cases of complete ankylosis of the spine and proximal joints. In Europe, the terms “spondylarthrite ankylosante” (ankylosing spondylitis) and Bechterew’s disease (primarily in Germany) were used. In America, however, the preferred term for the disease was “rheumatoid spondylitis” and remained so until 1963 when the American Rheumatism Association officially approved the name “ankylosing spondylitis”.6 However, there is a continuing struggle to establish consensus in many clinical aspects of AS. As discussed by van der Heijde et al in “Treatment trials in ankylosing spondylitis: current and future considerations” within this supplement (see p iii24), multiple sets of criteria have been developed for AS, but none have been deemed optimal.
In preparation for the International Workshop on New Treatment Strategies in Ankylosing Spondylitis held in Berlin, Germany, 18–19 January 2002, we sent a questionnaire to 30 international experts from countries in Europe and North and Central America to identify points of agreement and disagreement with nomenclature, disease classification, and study design for future trials. Experts were selected on the basis of personal knowledge and significant relevant publications. Many of the questions were designed in the context of indication for anti-TNFα therapy, either in clinical practice or in clinical trials.
The questionnaire was composed of 36 questions to be answered by either “yes/no” or selection of one multiple choice item. Twenty eight of the 30 international experts (93%) responded to the questionnaire (Appendix). The survey results are presented and discussed herein. Tables 2 and 3 summarise the agreements and disagreements among the respondents. A majority agreement was interpreted as >50% response rate.
Agreements* and disagreements among respondents to the questionnaire
Agreements among respondents to the questionnaire on aspects of future treatment trials
NOMENCLATURE
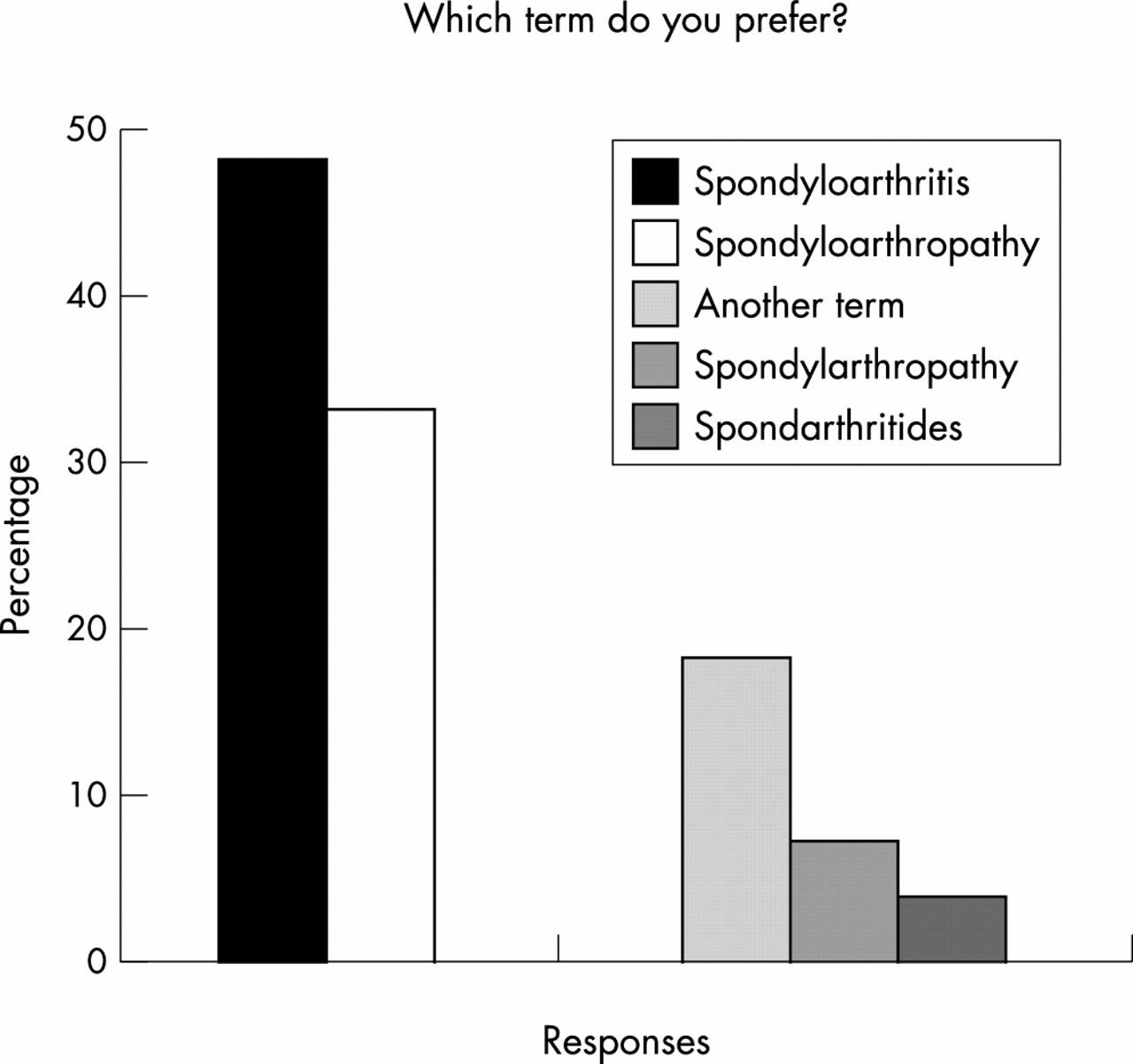
A clear majority of the experts (89%) agreed that it is important to have one common term, “spondyloarthropathy” or “spondyloarthritis,” with the majority (78%) agreeing that it is important for the term agreed upon to emphasise the inflammatory nature of the disease. However, despite the latter response, a majority agreement was not reached in favour of the term “spondyloarthritis” as proposed by a European League Against Rheumatism (EULAR) committee in 19957 (arthritis is defined as an inflammatory disease of the joint); only 48% of the respondents voted for this term. About one third (33%) preferred the term “spondyloarthropathy” (arthropathy is defined as any disease of the joint) (fig 1). Although the questionnaire results did not identify a single term for the disease group, the vast majority of the respondents (93%) were willing to follow a majority decision of the Ankylosing Spondylitis Assessment (ASAS) Working Group members about terminology, even if it contrasted with their current practice. The majority of the experts (96%) agreed to continue to use the term “spondyloarthritis” or “spondyloarthropathy” to distinguish this group of patients from those with RA and other connective tissue diseases.

Respondents’ preferences for the terms “spondyloarthritis” and “spondyloarthropathy.”
The majority of experts (59%) were in favour of using the term “reactive arthritis” instead of “Reiter’s disease,” and 37% were in favour of abandoning the term “Reiter’s disease” (fig 2). Approximately one quarter (26%) of the respondents thought the term “Reiter’s disease” should be reserved for reference to the classic triad of arthritis, urethritis, and conjunctivitis. Consistent with these results, the majority of experts participating in an earlier international workshop on ReA agreed to use the term “reactive arthritis” in clinical situations associated with the HLA-B27 antigen (19/30 (63%) experts); bacterial infections caused by Chlamydia, Yersinia, Salmonella, Shigella, or Campylobacter (29/33 (88%)), and a clinical picture (asymmetric arthritis of the lower limbs) that meets the ESSG definition of SpA (24/30 (80%)).4
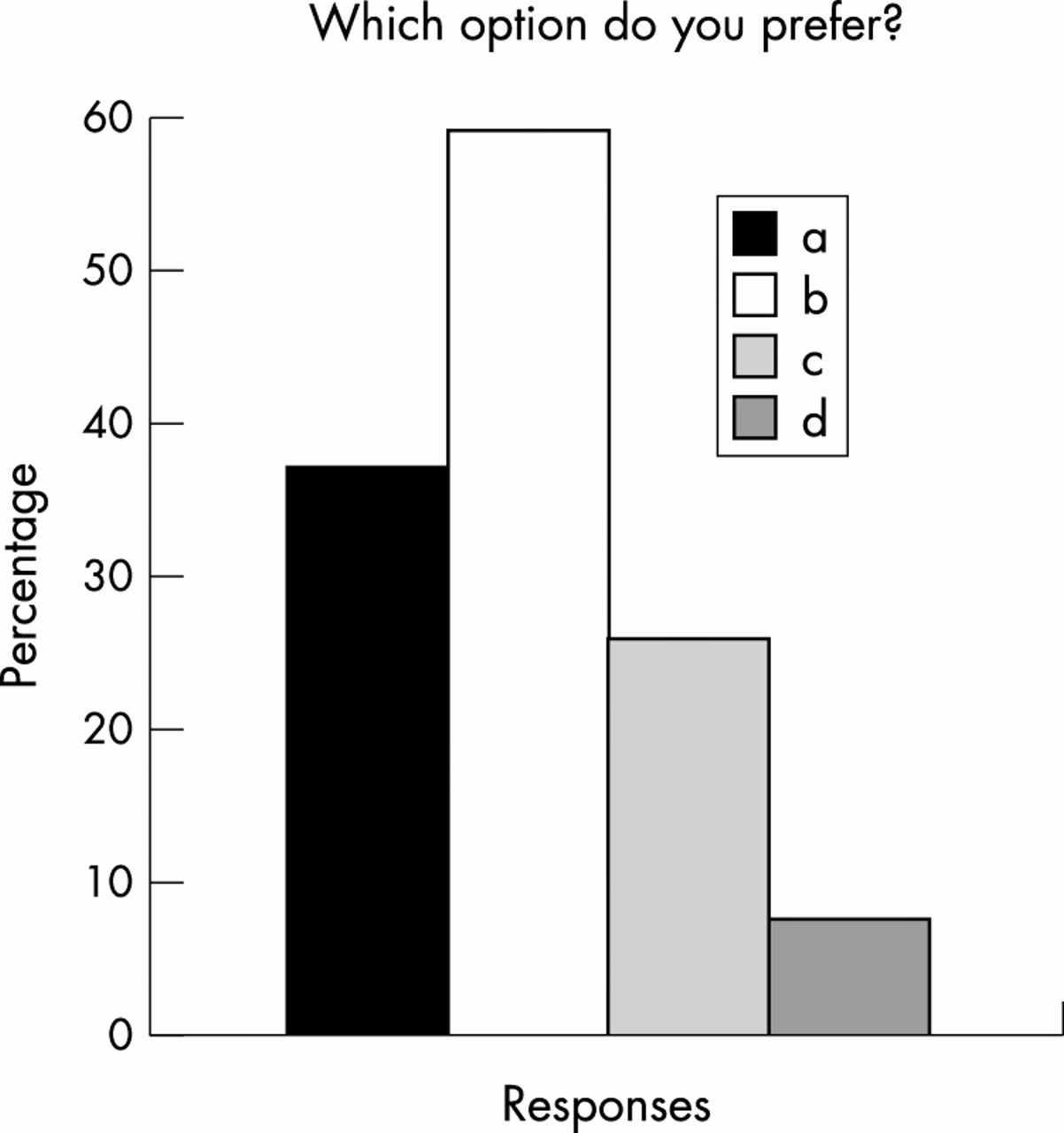
Percentages of respondents choosing to (a) abandon the term “Reiter’s disease”; (b) use the term “reactive arthritis”; (c) use only the term, “Reiter’s disease” in reference to the classic triad of arthritis, urethritis, and conjunctivitis; or (d) not change the terminology.
DISEASE CLASSIFICATION
Disease subcategories
The majority of experts (85%) were in favour of dividing patients with spondyloarthritis/spondyloarthropathy into five subcategories: AS, PsA, ReA, IBD-A, and uSpA.
Active or severe AS
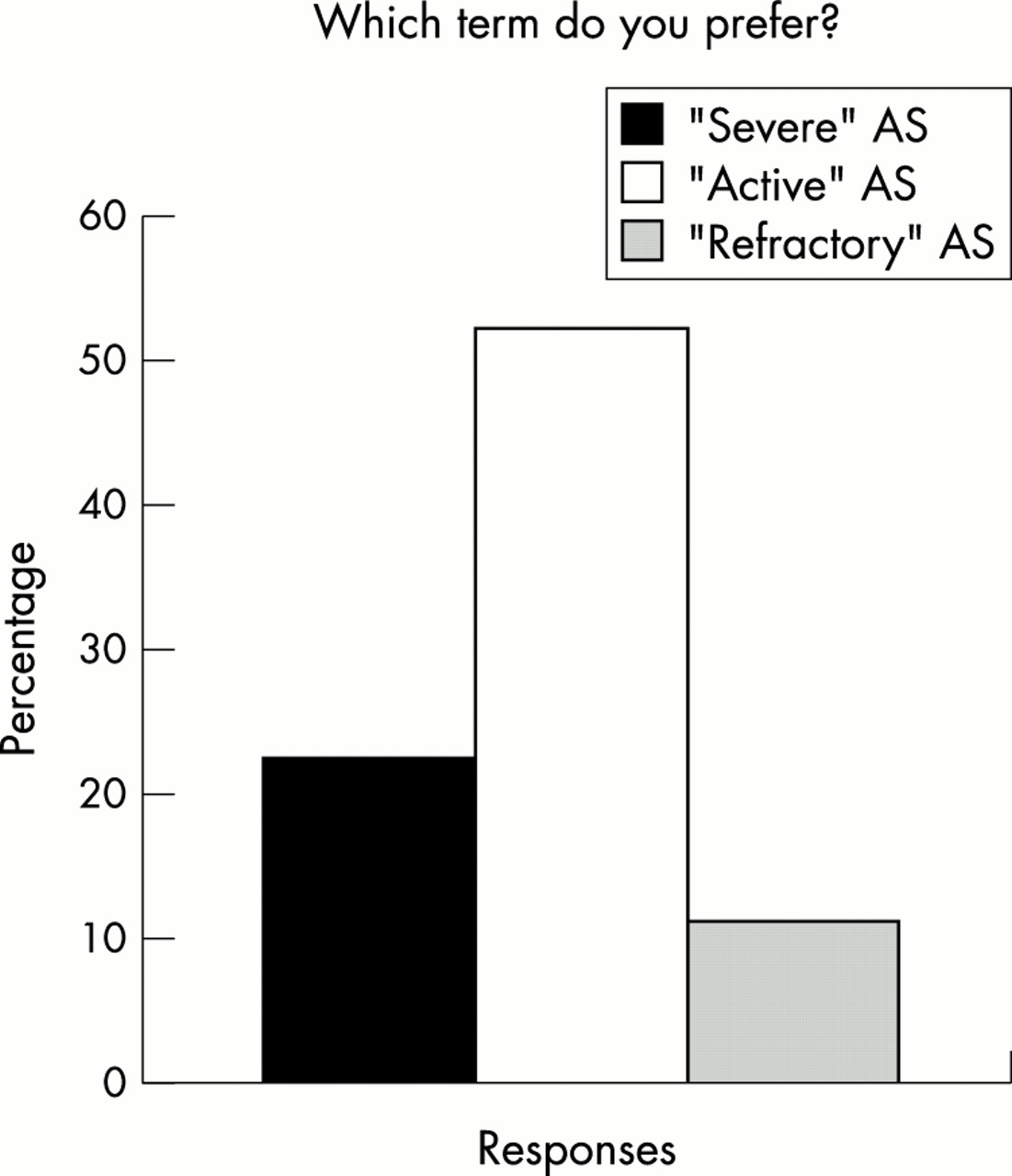
To describe the clinical status of AS in the context of indication for anti-TNFα therapy (that is, AS not adequately managed by conventional treatment), a small majority of respondents (52%) preferred the term “active AS,” 22% preferred “severe AS,” and 11% preferred “refractory AS” (fig 3). This distribution of votes may reflect the ambiguity created by the interrelationship between descriptive terms that are not equivalent in meaning. Whereas rheumatic disease activity usually refers to pain and other clinical signs of inflammation, severity can have at least two possible meanings, disease activity associated with (a) pain, loss of function, high C reactive protein (CRP) level, or multilocular spondylitis visualised by magnetic resonance imaging (MRI); or (b) structural damage or loss of mobility and function. In addition, a time component is involved. For example, active disease usually exists before the disease progresses to a severe state, and active and severe disease are precedents to refractory disease—that is, disease which is unresponsive to standard treatment. Although inflammatory pain without significant loss of mobility may be characteristic of active disease versus severely reduced mobility in the absence of pain in severe disease, the pain of active disease usually limits spinal mobility, further complicating the differentiation of active versus severe disease.8 However, the majority of the experts preferred the term “active disease.” This term becomes appropriate when considering the indications for anti-TNFα therapy because raised CRP levels are predictive of response to infliximab.9

Percentages of respondents preferring the term “severe,” “active,” or refractory” ankylosing spondylitis in the context of indication for anti-TNF treatment.
The majority of the respondents (59%) thought that patients classified as having active/severe AS should have disease duration of at least six months and fulfil the 1984 modified New York criteria,10 whereas 41% did not think this was necessary. In contrast, 100% of the experts thought that patients with uSpAs could be classified as having “active/severe” disease if they fulfilled the ESSG criteria,2 without fulfilling the New York criteria.
To assess disease activity, instruments such as the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) that are based on the absence or presence of several parameters, including joint pain/swelling, neck/back/hip pain, morning stiffness, and effectiveness of medication, are useful.11,12 In addition, the use of new diagnostic tools, such as MRI, which allow earlier detection of AS, may result in refinements to the definition of “active” disease and clearly delineate the various levels of disease severity.
AS disease activity indices
The majority of experts (89%) agreed that a certain level of disease activity (as measured by the BASDAI or other instruments) and failure of certain treatments should be a prerequisite for classification as active/severe AS. Only 4% of the respondents disagreed. The majority (56%) thought that a raised BASDAI score should not be the only criterion needed for definition of active/severe AS, whereas 37% of the experts thought it should be. Many of the experts (48%) chose a BASDAI score >4 as the cut off point for definition of active/severe AS, compared with 22% in favour of a BASDAI score >3 and 19% in favour of a BASDAI score >5 (fig 4). The trend for BASDAI score >4 as the preferred cut off point is consistent with inclusion criteria of BASDAI ≥4 in recent clinical evaluations of pharmacological treatments in patients with active/severe AS inadequately managed with conventional treatment.13,14 Furthermore, recent clinical trials of conventional13 and biological9,14–16 treatments have used the BASDAI or percentage improvement in BASDAI scores as a primary efficacy end point.

Percentages of respondents in favour of BASDAI scores >3, >4, >5, or >6 for definition of active/severe AS.
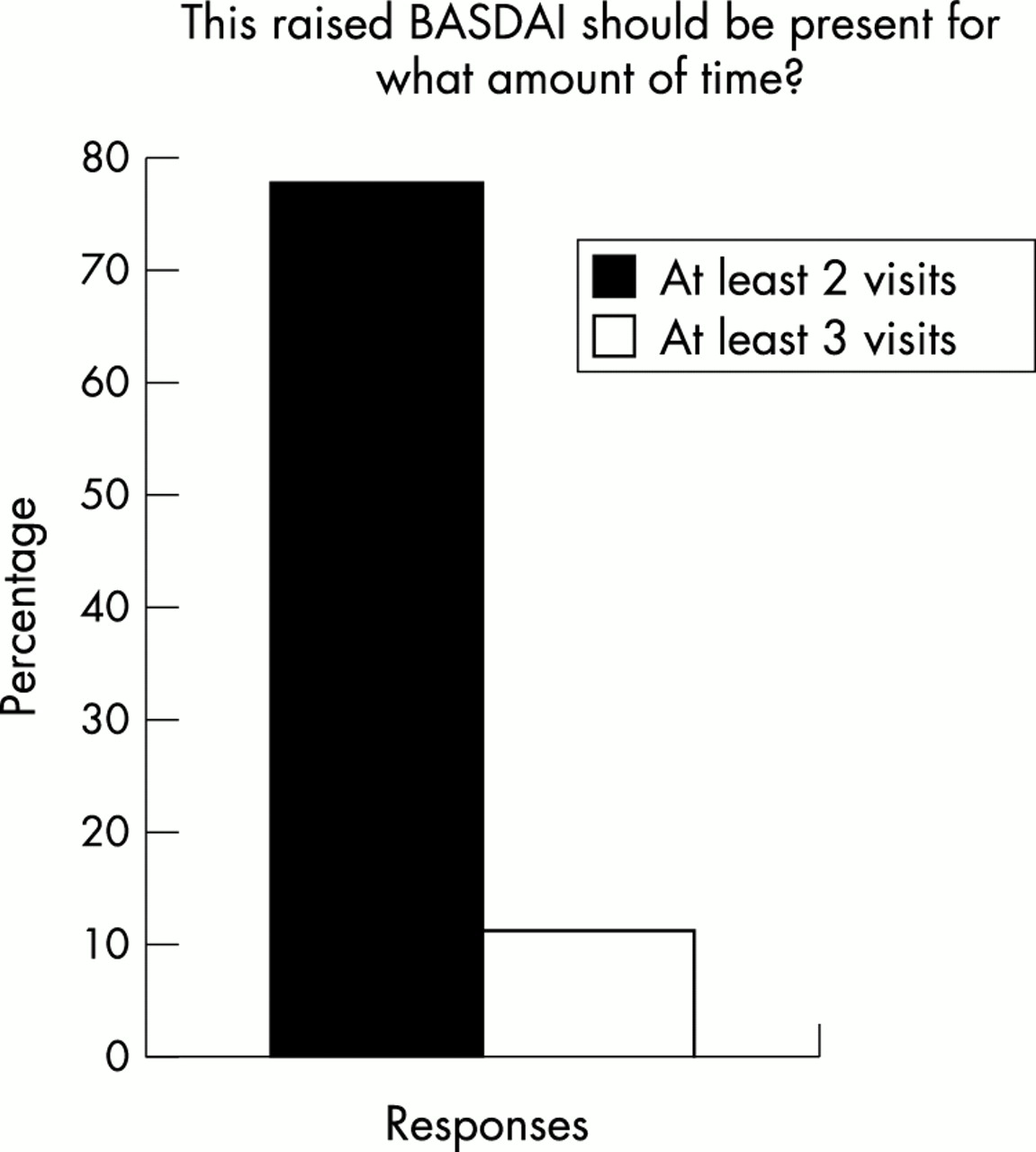
The majority (78%) of experts thought a raised BASDAI score should be present for two doctor visits, and 11% selected three doctor visits (fig 5). A clear cut agreement could not be reached on how long the raised BASDAI should be present: 15% were in favour of the “past two weeks”; 30%, the “past one month”; 15%, the “past two months”; 30%, the past three months; and 7%, the “past six months” (fig 6). Thus, two months seemed to be the best candidate for a compromise. A majority of experts (56%) thought that the use of the Bath AS Functional Index (BASFI) in addition to the BASDAI was not necessary for the definition of disease activity. In comparison, about one third (33%) of the experts were in favour of using the BASFI, among whom 56% chose BASFI >4 as the cut off score. Mindful that AS is not a regressive disease,12 the majority of experts (85%) did not think that a maximal radiographic score, such as a Bath AS Radiological Index (BASRI) ≤11, should be proposed to exclude completely ankylosed patients from receiving new treatments.
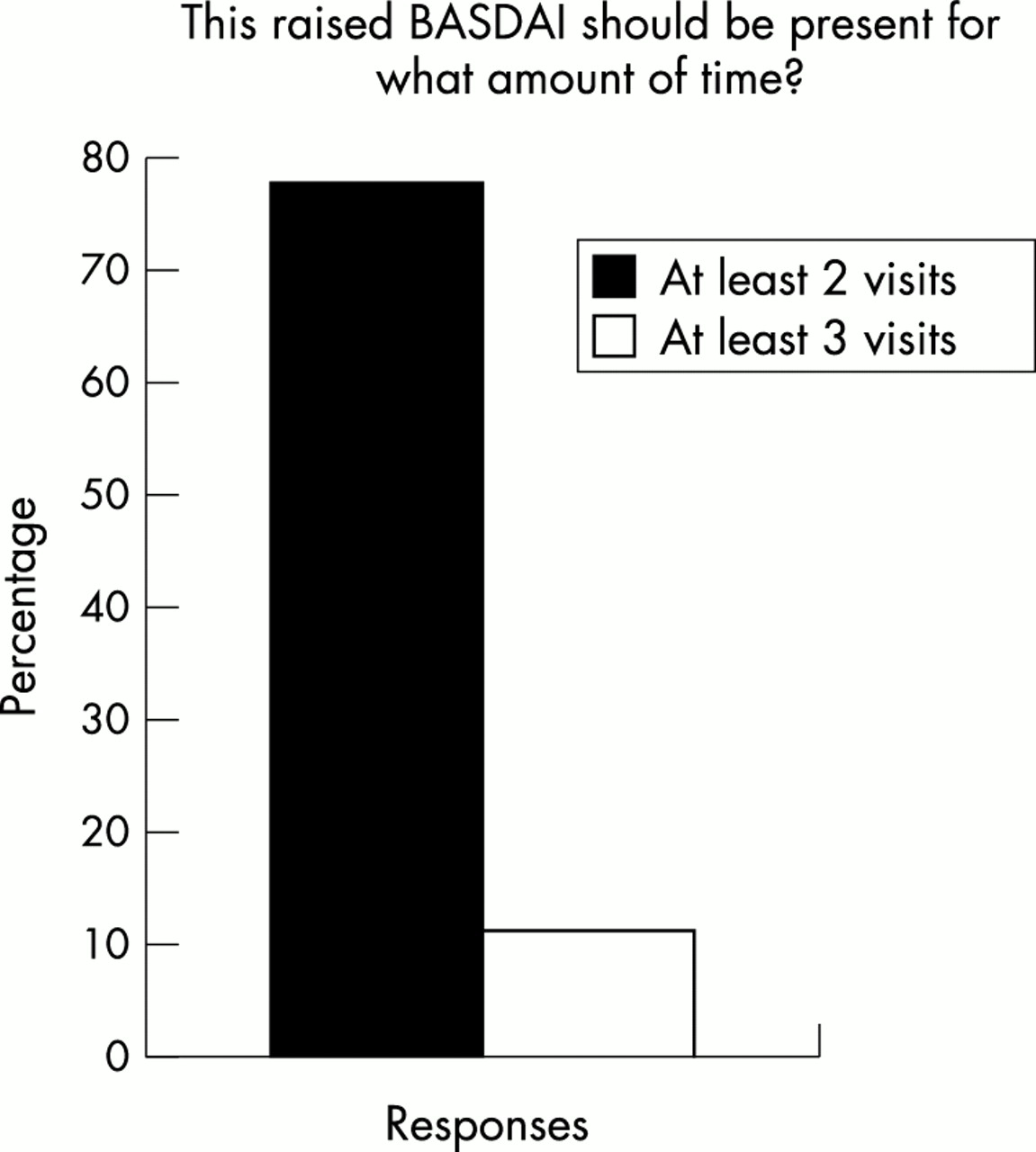
Percentages of respondents in favour of duration of raised BASDAI scores for at least two or at least three office visits. No respondent voted for more than three visits.

Distribution of responses to question about the duration of raised BASDAI scores at presentation.
Physical and laboratory parameters
Although enthesitis is considered to be the hallmark of AS,4,17 the majority of experts (81%) did not think that the presence of peripheral arthritis or enthesitis should be a prerequisite for definition of active/severe disease.
The majority of experts (58%) did not think that spinal involvement should be a requirement for definition of active disease in patients considered for anti-TNFα therapy, whereas 35% thought it should be. Of the experts who thought that spinal involvement should be a prerequisite, 42% stated that clinical diagnosis of spinal involvement is adequate, whereas others thought that spinal involvement should be confirmed by radiography (27%), MRI (14%), or scintigraphy (4%).
The majority of experts (80%) did not consider the presence of peripheral arthritis or enthesitis to be a prerequisite for active disease.
The majority of respondents (65%) did not think that a raised CRP level (fig 7) should be a prerequisite for definition of active/severe AS; 27% disagreed. The majority vote is consistent with results of a recent evaluation of CRP by Spoorenberg et al, in which CRP (and erythrocyte sedimentation rate) was found to have limited value in assessing or predicting disease activity.18 Thus in the clinical evaluation of new treatments for AS, CRP does not appear to be a reliable diagnostic (inclusion) criterion or a reproducible outcome variable. However, as previously mentioned, patients with raised CRP levels apparently respond better to anti-TNFα therapy with infliximab.9

Percentages of respondents in favour of (Yes) and against (No) the requirement of raised CRP for definition of active/severe AS.
The majority (73%) did not think that a certain amount of physical therapy should be required for definition of active/severe AS; 27% disagreed.
Treatment failure
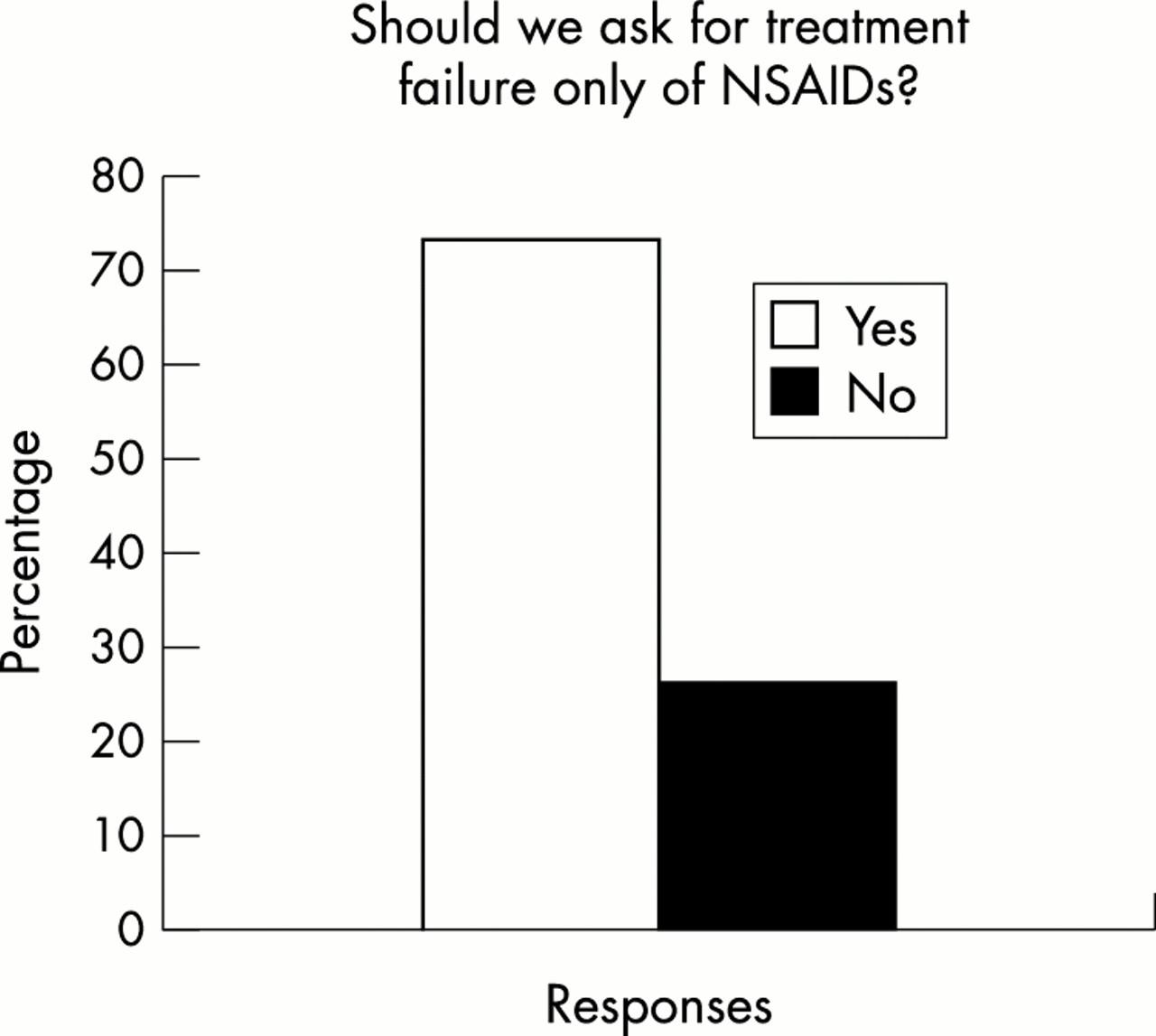
The majority of the respondents (73%) thought that treatment failure of non-steroidal anti-inflammatory drugs (NSAIDs) alone is sufficient as a prerequisite for definition of active/severe AS; approximately one quarter of the experts (27%) disagreed (fig 8). This response is consistent with the requirement for NSAID intake as one of the five items used in a disease activity scoring system proposed by Dougados et al,8 reflecting the status of NSAID treatment as first line drug treatment for SpAs.19 The majority of experts (54%) thought NSAID treatment failure should be defined as failure of >2 NSAIDs, whereas 23% were in favour of failure of >3 NSAIDs (fig 9). The majority (73%) indicated that NSAID treatment should have failed at maximum doses; 8% thought lack of response at any dose was an adequate indication of treatment failure.

Percentages of respondents supporting failure of NSAID treatment alone to be sufficient for definition of active/severe AS.

Percentages of respondents in favour of failure of >2 NSAIDs, >3 NSAIDs, maximal NSAID dose, or any NSAID dose as a prerequisite for definition of active/severe AS.
The majority of experts (89%) did not think that failure of the phenylbutazone treatment should be a prerequisite for definition of active/severe AS. Consistent with the lack of controlled data demonstrating the efficacy of other disease modifying antirheumatic drugs (DMARDs) in AS,20,21 73% of the experts did not think that failure of DMARDs should be a criterion for classification of active/severe AS (fig 10). However, no agreement was reached on the failure of sulfasalazine as a prerequisite for classification as active/severe AS; the respondents were equally divided on this issue with 46% in favour of, and 46% against sulfasalazine failure (fig 11). Among those in favour of sulfasalazine failure as a prerequisite, there was a 92% agreement that treatment failure should be at the maximum drug dose (3 g/day). This split in thinking reflects the controversy surrounding the use of sulfasalazine as second line treatment.8,22 Two double blind, placebo controlled studies failed to demonstrate the efficacy of sulfasalazine at doses of 3 g/day and 2 g/day, respectively, relative to placebo for the relief of pain in patients with active AS who were being treated with an NSAID.23,24 At variance with these findings, results of a meta-analysis of five randomised controlled trials of sulfasalazine showed potential clinical benefit for the short term treatment of AS.25 There is some indication that sulfasalazine is helpful for treating peripheral arthritis in patients with AS, but it is unclear whether it is useful in early active spinal disease.

Percentages of respondents in favour of (Yes) and against (No) failure of treatment with other DMARDs as a prerequisite for classification as active/severe AS.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disagreement among respondents as to whether failure of sulfasalazine should be a prerequisite for classification as active/severe AS.
FUTURE STUDIES
As with any new drug that has the potential to impede disease progression and provide symptomatic relief, investigators face difficulties in designing an ethical, double blind, placebo controlled, long term prospective study of anti-TNFα for the treatment of AS. Inherent difficulties associated with clinical investigations are compounded by the absence of standardised outcome assessments. The majority of the experts (59%) thought that it would not be ethically possible to conduct a double blind, placebo controlled trial over a two year period to evaluate the efficacy of anti-TNFα therapy in ameliorating radiographic progression and preventing ankylosis in AS. The majority of experts (85%) thought that a two to five year follow up of a cohort with active disease receiving treatment with an anti-TNFα agent is the only way to demonstrate these treatment goals, whereas 11% of the experts disagreed. The majority of the experts (56%) thought that a minimum duration of disease should be a prerequisite for active/severe disease warranting anti-TNFα therapy; 41% opposed this requirement. Of the experts in favour of a minimum duration, 60% preferred a duration of six months; 20% preferred a duration of one year.
The majority of experts agreed that after studies have clearly shown that anti-TNFα agents are efficacious in AS and PsA, more studies are needed to demonstrate their efficacy in ReA (70%), IBD-A (74%), and uSpA (74%). The percentages of experts who thought that additional studies for ReA, IBD-A, and uSpA were not necessary were 26%, 26%, and 22%, respectively.
The sensitivity of MRI as a diagnostic tool for AS is becoming evident and may meet the need for prospective evaluation of disease activity. Studies have shown that acute spinal inflammation not detectable by radiography can be visualised by this methodology.14,26–28 The questionnaire showed that the majority (70%) of experts have had experience with spinal MRI, among whom 79% thought that early structural damage such as erosions at the vertebral edges can be reliably detected earlier by MRI than by conventional x ray measurements. Only a few experts (16%) did not think MRI offered this advantage over conventional x rays. Fewer than one third (30%) of experts had no experience with spinal MRI. The majority of the experts with MRI experience (63%) thought that structural changes would be visible by MRI as early as six months into the disease process; 32% disagreed.
For trials of anti-TNFα therapy, the workshop participants informally agreed that annual radiography and biannual MRI would be valuable tools for assessment of treatment effect. An x ray examination would provide basic information about the progression of disease, and MRI would provide valuable data about progressive structural damage and potential sparing of erosion after treatment. The following preliminary suggestions for inclusion criteria for clinical trials of anti-TNFα therapy in patients with AS were proposed: BASDAI score >4, disease duration ≥6 months, and treatment failure with two NSAIDs at maximum doses. Many other aspects of study design, including additional inclusion criteria, exclusion criteria, study protocol, and parameters for assessing efficacy and outcome, remain to be determined. Because anti-TNFα agents have the potential to alter the clinical course through their immunomodulatory effects in patients with SpA,29,30 establishing standardised outcome assessment methods that can precisely characterise treatment effects becomes all the more critical. Until standardised methods are established, an alternative is to use, in parallel, both the BASDAI and the core set of domains established by the ASAS Working Group in clinical studies over the next two to three years to determine optimal assessments.
DISCUSSION
New treatment strategies that have the ability to redress pathogenetic processes offer hope for improved management of AS. Their therapeutic role will be determined by the results of well designed clinical trials. However, standards for nomenclature, diagnosis, and grading of disease need to be clearly defined to facilitate the collection of conclusive, reproducible, clinically relevant data.
The results of the questionnaire disclosed some discrepancies in the terminology and criteria for diagnosis and classification of disease status used by rheumatologists. However, the areas of agreement reached by the experts responding to this questionnaire serve as a foundation for the continued development of standardised nomenclature and disease definition. The points of disagreement will help to focus further discussion.
Significant agreements about nomenclature included the use of a single term that emphasises the inflammatory nature of the disease to refer to the group of related diseases known as spondyloarthropathies, either “spondyloarthritis” or “spondyloarthropathy,” and the use of the term reactive arthritis instead of “Reiter’s disease.” Although no agreement was reached about the use of “spondyloarthritis” or “spondyloarthropathy,” the majority of experts agreed to use whichever term the ASAS Working Group selected.
Significant agreements for disease classification included subdivision of spondyloarthropathies into five categories (AS, PsA, ReA, IBD-A, and uSpA), classification of uSpAs as active/severe based on fulfilment of the ESSG criteria, and a raised BASDAI for at least two office visits and treatment failure of more than two NSAIDs at maximum dose as two prerequisites for classification of active/severe AS.
For clinical evaluations of anti-TNFα therapy, the majority of experts agreed that a two to five year cohort study versus a long term, placebo controlled, double blind study was the only ethical way to prove that anti-TNFα therapy ameliorates radiographic disease progression and prevents the ankylosing process in AS.
In conclusion, currently there is no universal agreement on the terminology used to describe SpAs, or criteria for diagnosis and classification of AS. Agreements in these areas need to be reached for the sake of future clinical evaluations of new and conventional treatments, as individual treatments and in relation to each other. Because data from clinical trials form the basis for designing treatment strategies in clinical practice, consensus in these areas is critical to developing criteria for patient selection, disease characterisation, and treatment outcome assessment. The results of the questionnaire serve as a starting point for further discussion with the intent of reaching worldwide consensus in these areas.
Appendix: Experts who responded to the questionnaire
EM Veys, H Mielants, Belgium; M Dougados, M Breban, France; C Salvarani, Italy; E Collantes-Estevez, Spain; R Burgos-Vargas, Mexico; MA Khan, J Davis, P Mease, USA; R Inman, W Maksymowych, Canada; K Pavelka, Czech Republic; W Ebner, Austria; A Calin, P Emery, H Gaston, O Fitzgerald, D McGonagle, UK; D van der Heijde, A Boonen, S van der Linden, B Dijkmans, The Netherlands; H Zeidler, J Sieper, J Brandt, M Rudwaleit, J Braun, Germany.