Article Text

Abstract
Background: The extensor tendons over fingers are devoid of a tendon sheath, so that the term paratenonitis is used to describe extra-articular hyperemia or anechoic fluid collections along the extensor tendons of the fingers. Although the grading of paratenonitis is found in one sonographic scoring system of RA known as German US7, the clinical significance of paratenonitis is not fully understood.
Objectives: To determine the clinical significance of finger extensor paratenonitis detected by ultrasound (US), especially in the patients with RA.
Methods: We reviewed 1200 reports of the US examination underwent in our division since April 2015. The items necessary for scoring US5 scores (the ‘hand-limited version’ of the German US7) have been routinely recorded. The cases with finger extensor paratenonitis over the dorsal metacarpophalangeal joint (MCPJ) were determined. The severity of articular synovitis in the perilesional MCPJ were subjectively graded for grey-scale (GS) and power Doppler (PD) on a four-step scale (0-3) and scored using EULAR-OMERACT combined scoring system. In RA patients, US5 scores were determined for the involved hands.
Results: Paratenonitis was found in 44 fingers in the 38 hands of the 36 patients with rheumatic diseases/disorders including 25 patients with RA (11 early RA and 14 established RA). Non-RA diseases/disorders included 4 cases of undifferentiated arthritis, 2 cases of PsA, 1 case each of SLE, Sjogren syndrome, reactive arthritis and other disorders.

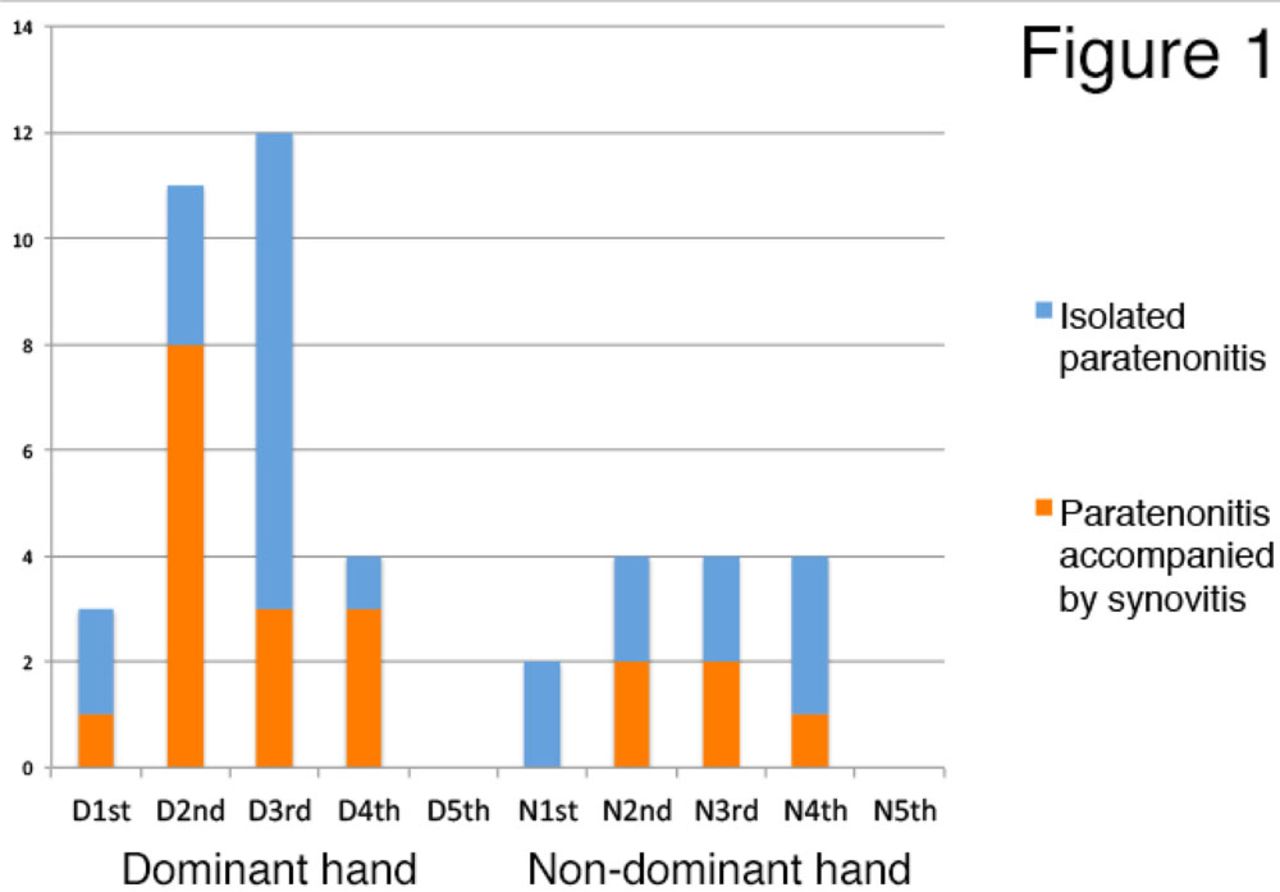
The 44 fingers were classified according to the absence or presence of articular synovitis in the perilesional MCPJ into “isolated paratenonitis” or “paratenonitis accompanied by synovitis”. The distribution of paratenonitis over the 1st-5th fingers of the dominant or non-dominant hands is shown in Figure 1. Paratenonitis was relatively frequently found in the 3rd and 2nd fingers of the dominant hands. Interestingly, articular synovitis in the perilesional MCPJ were found significantly more frequent in the cases of MCP2 in the dominant hands (73%) than in the cases of MCP3 in the dominant hands (25%) (p=0.039).

{kind=link}
{kind=link}
Among the 27 hands with paratenonitis of 25 RA patients, US5 scores were compared based on the absence or presence of moderate to severe articular synovitis in the perilesional MCPJ (the combined score >1) (Figure 2). GS synovitis score, PD synovitis score and PD tenosynovitis score were significantly higher in those with moderate to severe perilesional MCP synovitis than in those without it (p=0.007, 0.0092 and 0.0458, respectively).
Conclusion: Finger extensor paratenonitis over the dorsal MCPJ tends to occur in the 3rd and 2nd fingers of the dominant hand. In RA patients, paratenonitis accompanied by active perilesional MCPJ synovitis are presumably due to active disease, while isolated paratenonitis can also be caused possibly by degenerative changes due to overuse or deformity. Isolated paratenonitis may be more frequently found in the 3rd finger than in the 2nd finger of the dominant hand.
References: None
Disclosure of Interests: Takeshi Suzuki Speakers bureau: Abbvie, Asahi-kasei, Astellas, Bristol-Myers Squibb, Chugai, Eli Lilly, Mitsubishi-Tanabe, Novartis, UCB, Harumi Shirai: None declared