Article Text

Abstract
This paper presents the wrist joint MR images of the EULAR–OMERACT rheumatoid arthritis MRI reference image atlas. Reference images for scoring synovitis, bone oedema, and bone erosions according to the OMERACT RA MRI scoring (RAMRIS) system are provided. All grades (0–3) of synovitis are illustrated in each of the three wrist joint areas defined in the scoring system—that is, the distal radioulnar joint, the radiocarpal joint, and the intercarpal-carpometacarpal joints. For reasons of feasibility, examples of bone abnormalities are limited to five selected bones: the radius, scaphoid, lunate, capitate, and a metacarpal base. In these bones, grades 0–3 of bone oedema are illustrated, and for bone erosion, grades 0–3 and examples of higher grades are presented. The presented reference images can be used to guide scoring of wrist joints according to the OMERACT RA MRI scoring system.
- EULAR, European League Against Rheumatism
- Gd, gadolinium containing contrast agent
- MCP, metacarpophalangeal
- MRI, magnetic resonance imaging
- OMERACT, Outcome Measures in Rheumatology Clinical Trials
- RA, rheumatoid arthritis
- magnetic resonance imaging
- erosion
- rheumatoid arthritis
- synovitis
- wrist
Statistics from Altmetric.com
- EULAR, European League Against Rheumatism
- Gd, gadolinium containing contrast agent
- MCP, metacarpophalangeal
- MRI, magnetic resonance imaging
- OMERACT, Outcome Measures in Rheumatology Clinical Trials
- RA, rheumatoid arthritis
The wrist joints are very frequently involved in rheumatoid arthritis (RA), including early RA, and assessment of wrist joints is included in conventional radiological and clinical scoring systems.1–4 Numerous studies using magnetic resonance imaging (MRI) in RA have examined the wrist joint, either alone or in combination with the metacarpophalangeal (MCP) joints. A predictive value of magnetic resonance imaging (MRI) findings (synovitis, bone oedema, and MRI bone erosions) in the wrist joint with respect to short term (one year,5–7) as well as long term (five to six years,8,9) radiographic destructive bone damage has been reported. Furthermore, recent data suggest that MRI of wrist joints is more sensitive to erosive change than MRI of MCP joints,10 perhaps due to the higher number of bones in the wrist. The majority of the validation studies of MRI in RA performed by members of the Outcome Measures in Rheumatology Clinical Trials (OMERACT) and European League Against Rheumatism (EULAR) groups have included wrist joints.11–15
The OMERACT 2002 RA MRI scoring system includes assessment of wrist joints.16 The aim of this section of the EULAR–OMERACT RA MRI reference image atlas is to provide wrist joint reference images for scoring according to the OMERACT RA MRI scoring (RAMRIS) system, described in more detail by Østergaard et al in this supplement.17
THE WRIST JOINT REFERENCE IMAGES
This atlas illustrates synovitis in the three regions of the wrist that are recommended for assessment when using the OMERACT scoring method—that is, the distal radioulnar joint, the radiocarpal joint and the intercarpal-carpometacarpophalangeal joints. Furthermore, example images are provided for semiquantitative scoring of bone erosions and bone oedema in five selected bones of the wrist: the radius, scaphoid, lunate, capitate and a metacarpal base. Representative examples of each grade of synovitis and a selection of grades for bone abnormalities are presented. For reasons regarding feasibility not all bones and grades are included.
The examples for this atlas were selected by consensus in the OMERACT MRI in RA group. Details of the selection process and applied MRI sequences can be found in the paper by Bird et al in this supplement.18
A description of the reference image sheets presented on the following pages, and how to use them, is provided in figs 1–3 (see page 46–page 47).
We hope the presented reference images will be useful to guide scoring of wrist joints according to the OMERACT RA MRI scoring system.







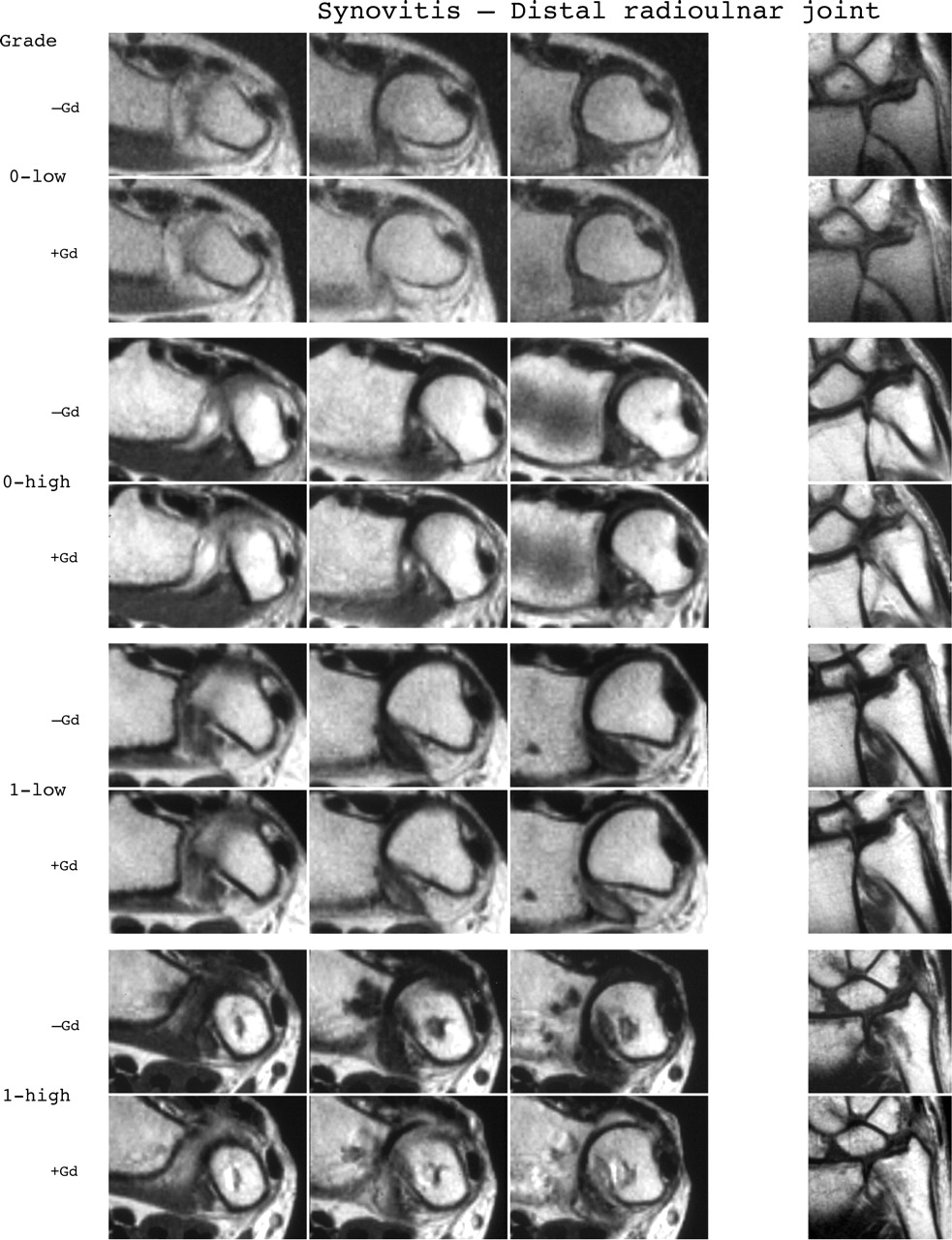
Synovitis reference image sheets (pages i24–i29, total 6). Reference image sheets for synovitis in the distal radioulnar joint, the radiocarpal joint, and the intercarpal-carpometacarpophalangeal joints are illustrated on two single-page sheets each. Examples are provided from the low end and high end of each grade (0–3). Synovitis is graded 0–3 (normal, mild, moderate, severe) as estimated by thirds of the presumed maximum volume of enhancing tissue as described in the OMERACT RAMRIS (see table 1, reference 11). The MRI set to be assessed should be compared with the axial precontrast and postcontrast T1 weighted reference images and the joint assigned the score of the best possible match. The first carpometacarpal joint should not be scored. All axial slices covering the joint should be taken into account. A total score (range 0–9) can be calculated. The diagram above describes the positions and types of images included.




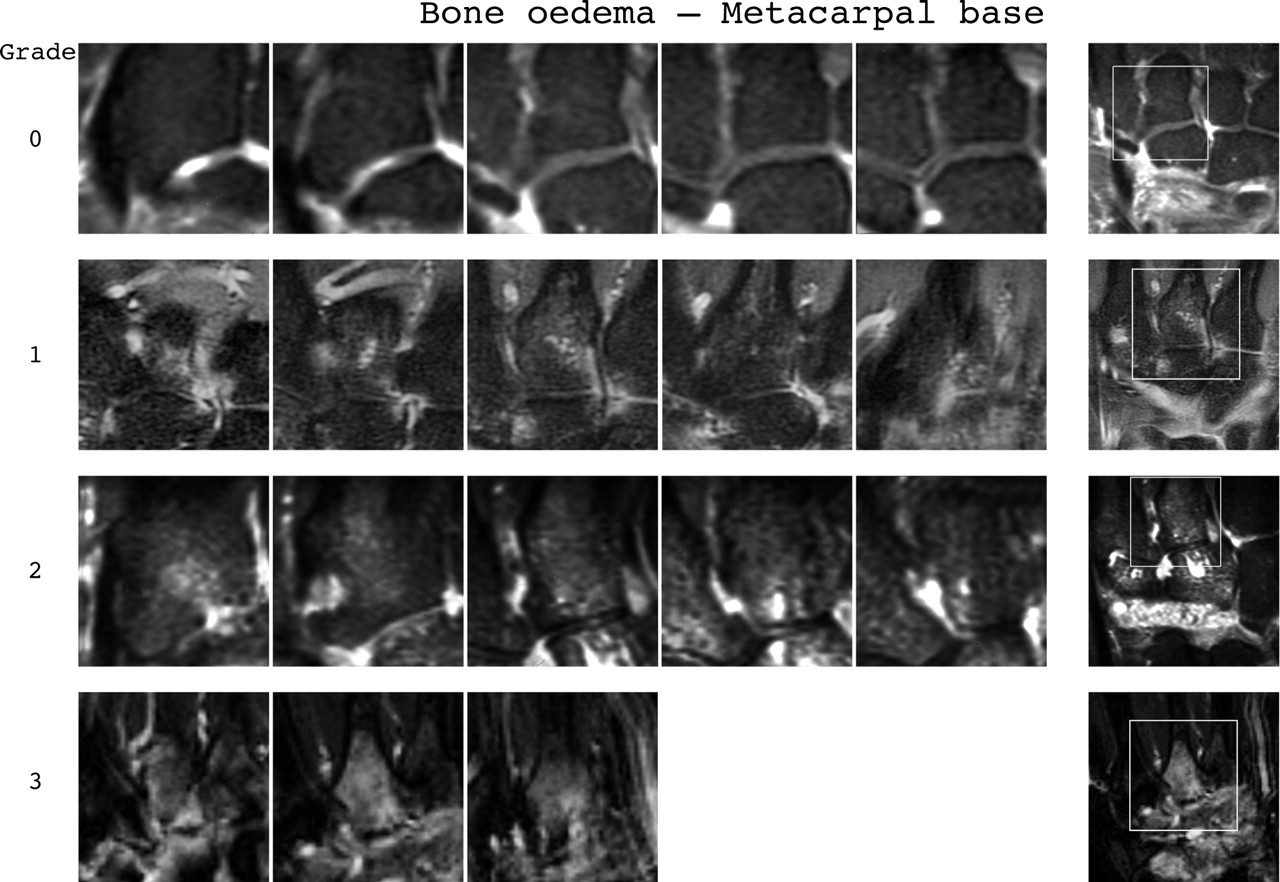

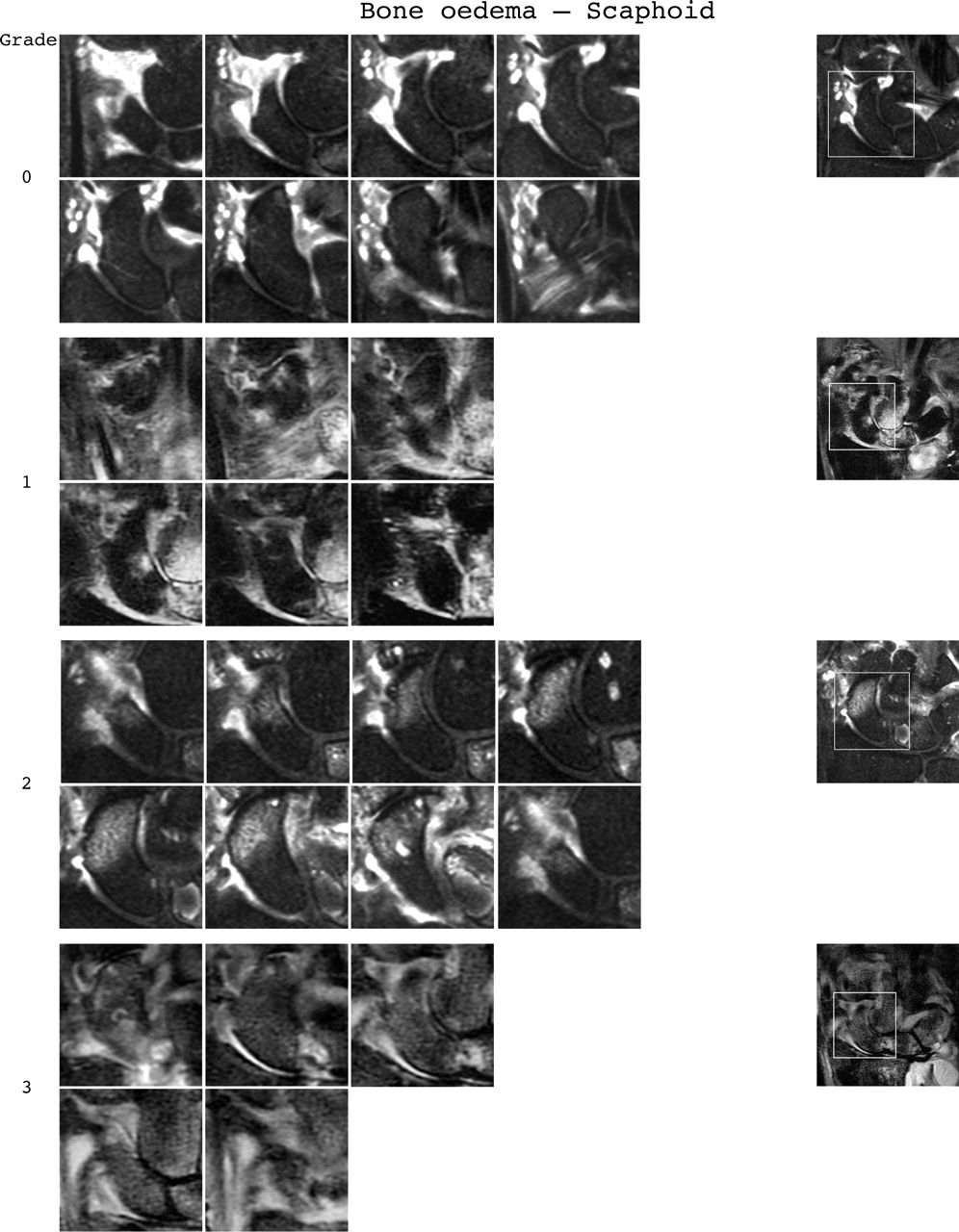
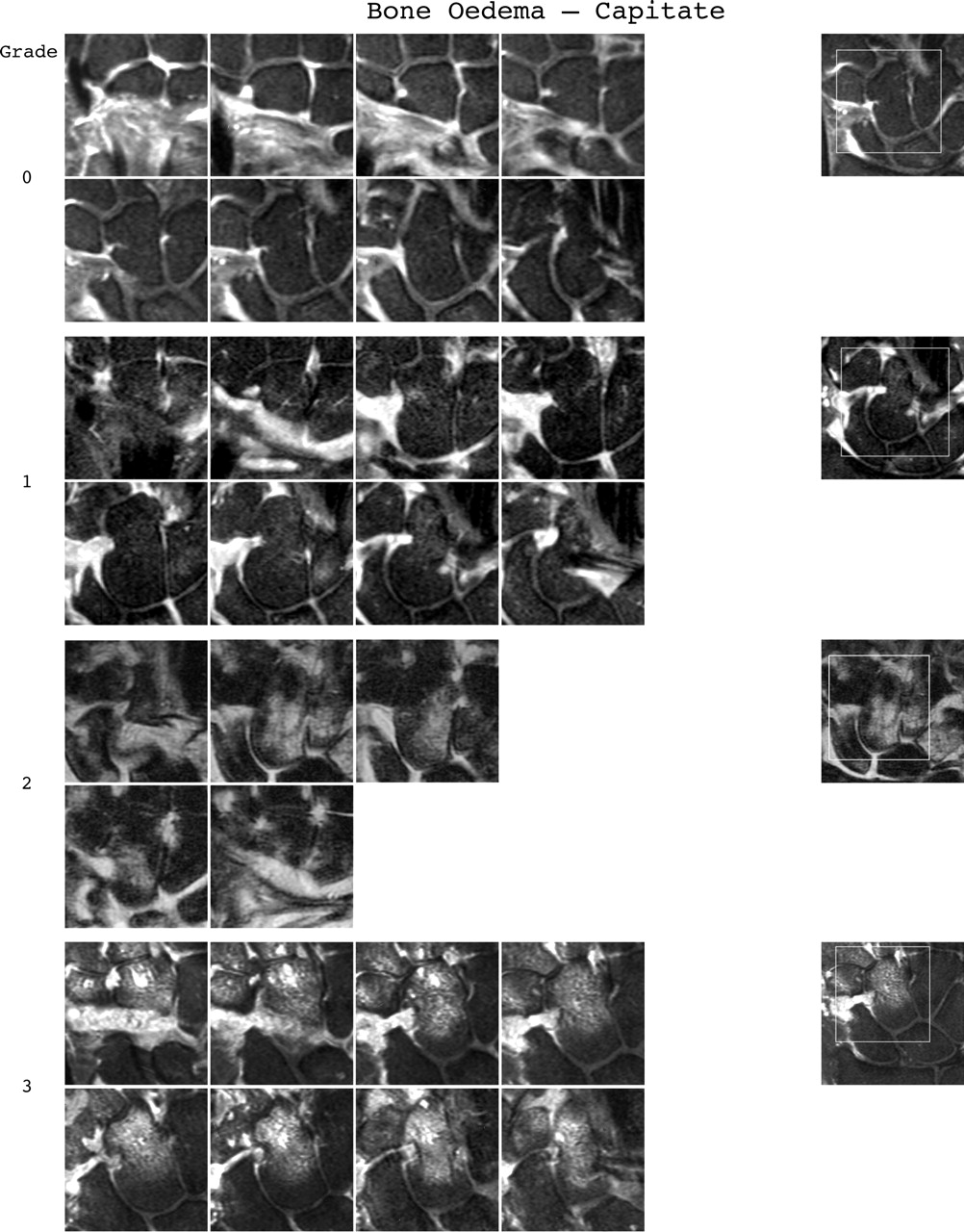
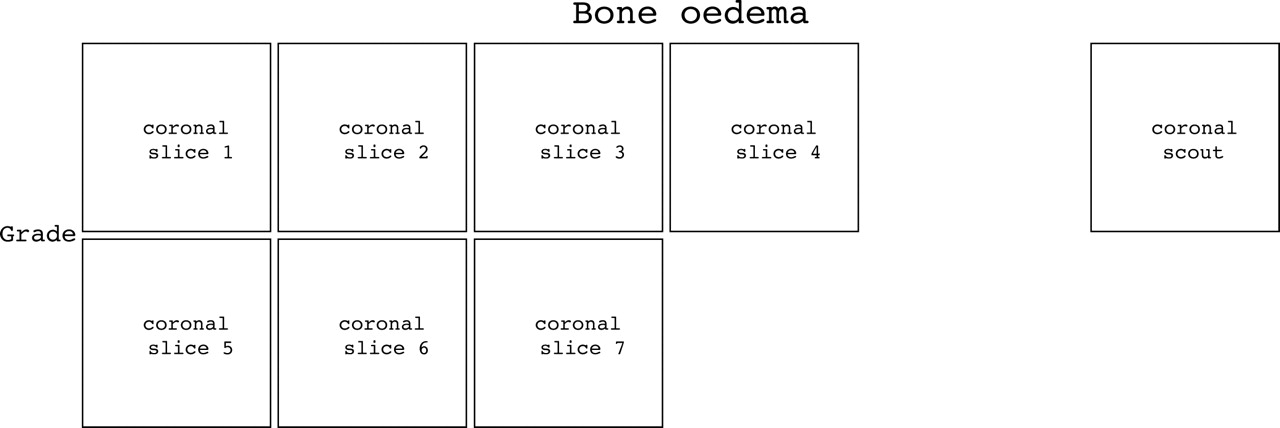
Bone oedema reference image sheets (pages i30–i34, total 5). Bone oedema in the radius, scaphoid, lunate, capitate, and a metacarpal base is illustrated on a single-page sheet each. All grades (0–3) are presented except when appropriate examples could not be found. Bone oedema is graded by percentage volume (0–3, by 33% volume increments) of the assessed bone as described in the OMERACT RAMRIS (see table 1, reference 17). For long bones (radius, ulna, metacarpal bases), the “assessed bone volume” is from the articular surface (or its best estimated position if absent) to a depth of 1 cm, and in carpal bones it is the whole bone. If erosion and oedema are concurrently present, oedema is scored as the proportion of the original bone. All coronal slices (T2 weighted fat saturated or short tau inversion recovery (STIR)) covering the bone need to be assessed to estimate the percentage of the total volume occupied by the oedema. The atlas reference images can be used for guidance and calibration. Each bone of the wrist should be scored separately. A total score (range 0–45) can be calculated. The diagram above describes the positions and types of images included. The varying number of coronal slices needed to cover the bone reflects varying bone sizes and varying slice thickness (2–3 mm).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
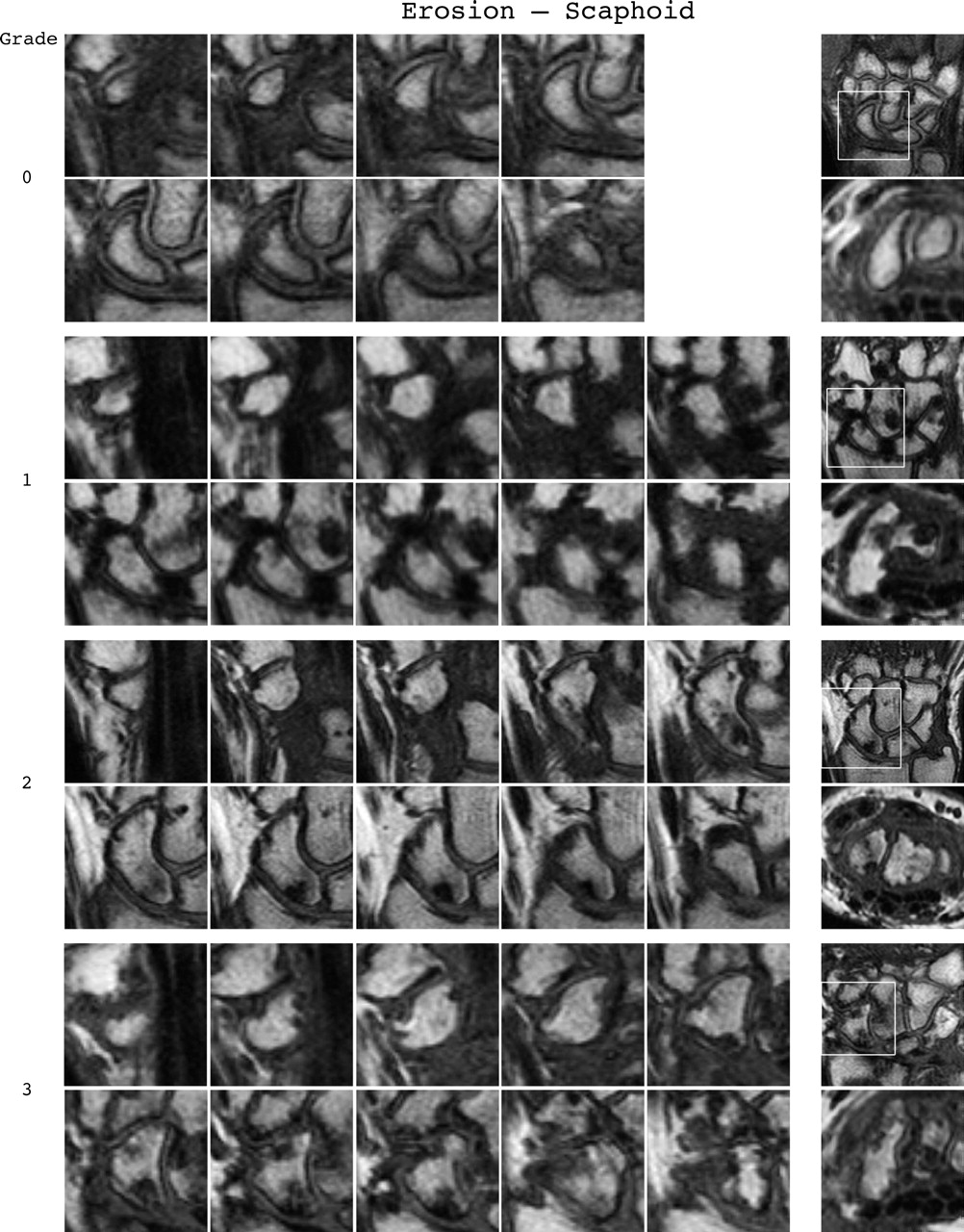
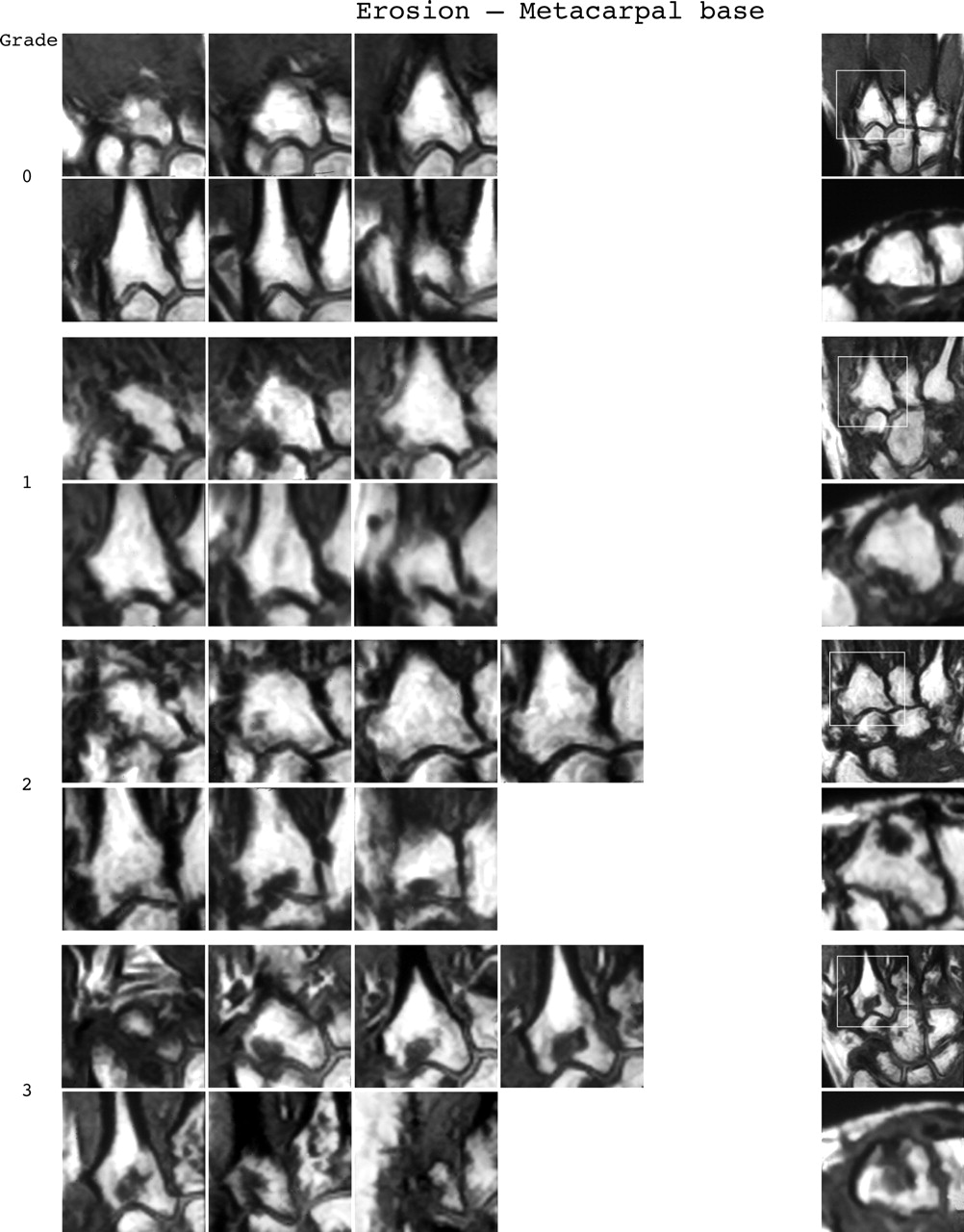
Bone erosion reference image sheets (pages i36–i45, total 10). Bone erosion in the radius, scaphoid, lunate, capitate and a metacarpal base is illustrated on two single-page sheets each. Grades 0–3 supplemented with examples of three higher grades are provided. Bone erosion is graded by assessing percentage volume (1–10, by 10% volume increments) of the assessed bone volume as described in the OMERACT RAMRIS (see table 1, reference 17). The “assessed bone volume” is defined as described above. It should be emphasised that all coronal slices covering the bone should be assessed to estimate the percentage of the total volume occupied by the erosion. The atlas reference images can be used for guidance and calibration. Each bone of the wrist should be scored separately. A total score (range 0–150) can be calculated. The drawing above explains the types and positions of images presented. The varying number of coronal slices needed to cover the bone reflects varying bone sizes and varying slice thickness (2–3 mm).
Acknowledgments
Photographer S Østergaard is acknowledged for skilful assistance with image preparation and set-up.
The European League Against Rheumatism (EULAR) is acknowledged for financial support of the publication of this atlas.