Article Text

Abstract
Interleukin 6 (IL6) is a pleiotropic cytokine with a wide range of biological activities. IL6 transgene into mice gives rise to the abnormalities such as hyper-γ-globulinaemia, thrombocytosis, infiltration of inflammatory cells into the tissues, mesangial cell proliferation of the kidney as well as splenomegaly and lymphadenopathy, which are predictable by the biological functions of IL6 shown in vitro. Continuous overproduction of IL6 is observed in patients with some immune-inflammatory diseases such as Castleman's disease and rheumatoid arthritis that are frequently associated with similar abnormalities to those of IL6 transgenic mice, strongly suggesting the involvement of IL6 in the human diseases. Successful treatment of the model animals for immune-inflammatory diseases with anti-IL6 receptor (IL6R) antibody thus indicates the possible application of IL6 blocking agents to treat the IL6 related immune-inflammatory diseases of humans. In this review, the new therapeutic strategy for Castleman's disease and RA using humanised antibody to human IL6 receptor, MRA, is discussed.
- interleukin 6
- anti-inteleukin 6 receptor antibody
- rheumatoid arthritis
- Castleman's disease
Statistics from Altmetric.com
As each monoclonal antibody grasps a specific target antigen epitope, it has been widely used as a research device or a diagnostic drug. It was also expected as a “magic bullet” to treat cancer patients, but the attempt to apply monoclonal antibodies to treat cancer patients fell out of favour because of the failure caused by unexpected toxicity in some clinical trials in the late 1980s.1 Similarly, clinical trials of several antibodies targeted against the blood infection sepsis were halted because the treated patients were found to be more likely to die than untreated patients in the early 1990s.1 However, after accumulation of knowledge about the function and distribution of target molecules and also after working out new strategies to use chimerised or humanised antibodies of which varying amounts were replaced with human antibody sequences, therapeutic antibodies have begun to be applied to treat patients not only with cancers but also with immune-inflammatory disorders or acute rejection after organ transplantation. Interleukin 6 (IL6) is a pleiotropic cytokine that regulates immunological reactions in host defence, inflammation, haematopoiesis, and oncogenesis.2 ,3 Although IL6 plays important parts in the host immune system, dysregulated overproduction of IL6 causes unfavourable clinical symptoms and laboratory findings in the patients with immune-inflammatory diseases. In this review, pathological significance of IL6 overproduction in immune-inflammatory diseases and the therapeutic approach by blocking IL6 function using humanised anti-IL6 receptor (IL6R) antibody, MRA, are discussed.
Rationale for IL6 blocking treatment in immune-inflammatory diseases
PREIOTROPIC FUNCTIONS OF IL6
IL6 was originally identified as a B cell differentiation factor (BCDF) in the culture supernatants of mitogen or antigen stimulated peripheral mononuclear cells, which induced B cells to produce immunoglobulin4 ,5 and the cDNA encoding human IL6 was cloned in 1986.6 IL6 was then proved to be a pleiotropic cytokine with a wide range of biological activities (fig 1) and produced by various types of lymphoid and non-lymphoid cells, such as T cells, B cells, monocytes, fibroblasts, keratinocytes, endothelial cells, mesangial cells, and several tumour cells.3 In addition to BCDF activity, IL6 induces T cell growth and cytotoxic T cell differentiation7-12 through augmentation of IL2 receptor expression7 and IL2 production.13IL6 acts synergistically with IL3 on haematopoiesis to support the formation of multi-lineage blast cell colonies,14-18suggesting that it prompts haematopoietic stem cells in the G0 phase to enter into the G1 phase. Furthermore, IL6 is a potent inducer of terminal macrophage differentiation19 and osteoclast differentiation,20 and also induces platelet production by functioning as a megakaryocytic differentiation factor.21-23 In the acute phase reaction, IL6 stimulates hepatocytes to produce acute phase proteins such as C reactive protein (CRP), fibrinogen, α1 antitrypsin, and serum amyloid A (SAA)24 ,25 while it simultaneously suppresses the albumin production.26 Leucocytosis and fever have been found to be the result of in vivo administration of IL6.27 As a cell growth factor, IL6 can induce the proliferation of mesangial cells,28 epidermal keratinocytes,29 ,30 and various tumour cells such as plasmacytoma cells,31multiple myeloma cells,32 and renal carcinoma cells.33

Schematic model of IL6 functions. IL6 is a pleiotropic cytokine with a wide range of biological activities.
ABNORMAL FINDINGS OBSERVED IN IL6 TRANSGENIC MICE
From a study using IL6 transgenic mice, we can learn what kinds of abnormalities IL6 hyperproduction causes in vivo. Transgenic mice were produced by introduction of the human IL6 gene under the transcription control of the immunoglobulin μ heavy chain enhancer (Eμ) into C57BL/6 mice.34 Polyclonal hyper-γ-globulinaemia with massive plasmacytosis in the spleen and lymph nodes was then observed in Eμ-IL6 transgenic mice (fig 2, table 1). They showed increased levels of serum fibrinogen and reduced levels of serum albumin as well as an increased number of megakaryocytes in the bone marrow. IL6 transgenic mice also showed mesangial cell proliferation in the glomerulus (fig 3A), and lymphocyte proliferation with plasma cell infiltration in the interlobular septa and adjacent alveolar septa in the lung (fig 3C), and died within four or five months. These data indicate that IL6 can function in vivo in the same way as it does in vitro. Furthermore, these abnormal findings may represent some of the features observed in human immune-inflammatory disease such as Castleman's disease and rheumatoid arthritis (RA), and the patients with active disease are always associated with overproduction of IL6 in vivo.35-39
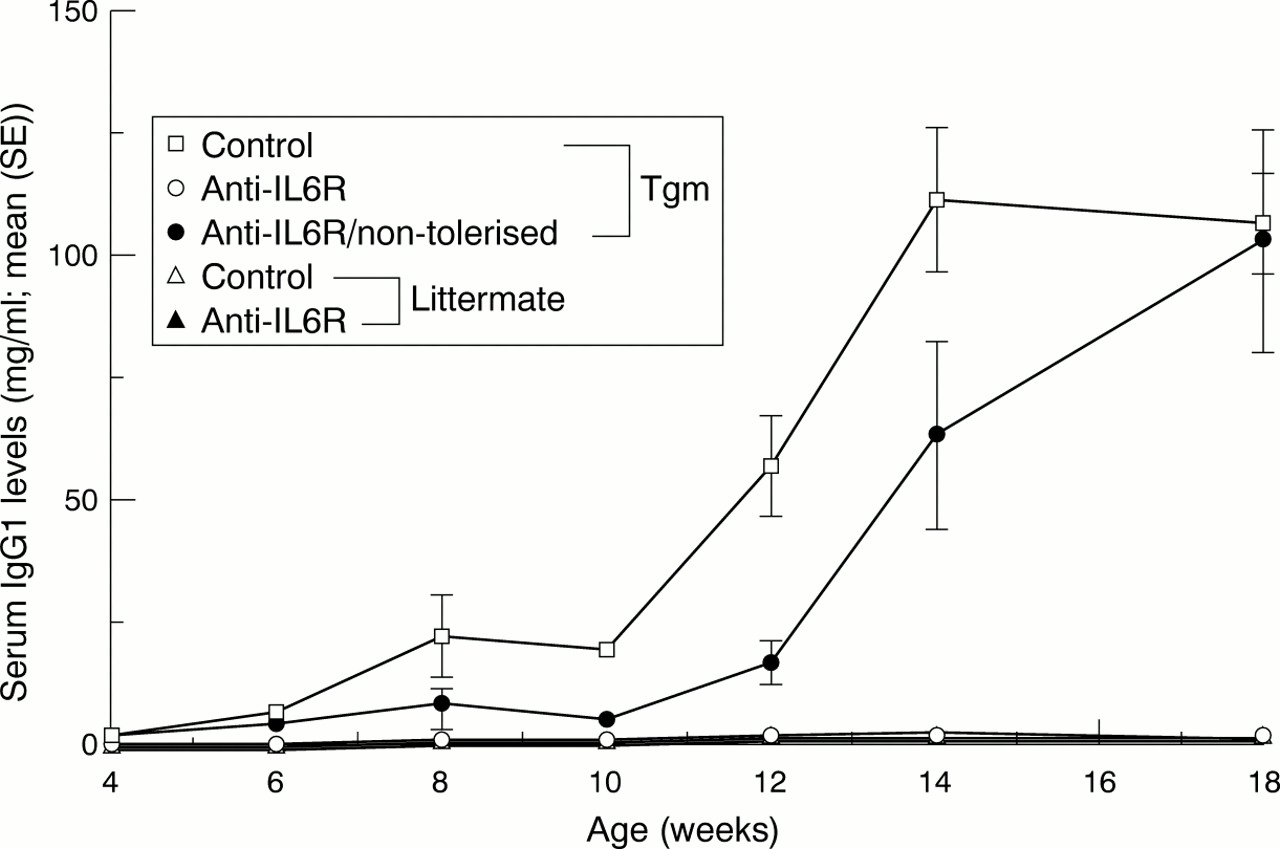
Anti-IL6R antibody treatment suppressed the increase in serum IgG1 levels in IL6 transgenic mice. C57BL/6J human IL6 transgenic mice (tgm) were first intraveneously treated with 2 mg/body of rat antimouse IL6R antibody (MR16–1) at 4 weeks of age to induce tolerance to the mice against rat IgG, then subcutaneously treated with 100 μg/body twice weekly from 5 to 17 weeks of age. Serum IgG1 levels were analysed by ELISA.
Abnormal findings in IL6 transgenic mice (C57 Bl/6J)

Anti-IL6R antibody treatment inhibited the development of mesangial proliferative glomerulonephritis and lymphocytic interstitial pneumonia in IL6 transgenic mice. C57BL/6J human IL6 transgenic mice (tgm) were treated with rat antimouse IL6R antibody (MR16–1) similarly to that of figure 2. Left kidneys and lungs were removed and fixed with 20% neutral buffered formalin for histological examination.
ANTI-IL6R ANTIBODY TREATMENT IN ANIMAL MODELS
The IL6R complex comprises two functional different membrane proteins: an 80 kDa ligand binding chain (IL6R, IL6R α-chain, CD126) and a 130 kDa non-ligand binding but signal transducing chain (gp130, IL6R β-chain, CD130). IL6R has a very short intracytoplasmic portion containing only 82 amino acids that is not essential for signal transduction. IL6, when bound to either a membrane anchored or soluble form of IL6R (sIL6R), induces the homodimerisation of gp130, resulting in a high affinity functional receptor.40 Therefore, several approaches can be proposed to block IL6 signal transduction: (1) inhibition of IL6 production or neutralisation of IL6; (2) blockade of IL6 binding to IL6R; (3) blockade of IL6/IL6R complex binding to gp130; (4) blockade of the intracytoplasmic signal through gp130. We have used anti-IL6R antibody to block IL6 signal transduction as a therapeutic strategy. This concept was tested in animal models: IL6 transgenic mice and collagen induced arthritis (CIA) mice.
As we described above, Eμ-IL6 transgenic mice developed hyper-γ-globulinaemia with massive plasma cell infiltration in the spleen and lymph nodes. Treatment with rat antimouse IL6R antibody, MR16–1, completely inhibited the increase in serum γ-globulin levels (fig 2) as well as plasmacytosis. The mice also suffered from mesangial proliferative glomerulonephritis and they started to show proteinuria and haematuria at the age of 8–10 weeks. MR16–1 treatment prevented the occurrence of proteinuria and haematuria in the mice. It was confirmed by the histological findings that mice treated by MR16–1 showed normal glomerulus (fig 3B) while untreated mice showed mesangial cell proliferation with occlusion of the glomerular capillaries (fig3A). The IL6 transgenic mice also showed lymphocyte infiltration in the many organs and developed the histological feature characteristic to lymphocytic interstitial pneumonia (LIP) in the lung (fig 3C). However, MR16–1 treatment completely prevented the pathological change of lung (fig 3D). Similarly, all the other abnormalities such as increase in serum fibrinogen, SAA and platelet counts as well as decrease in serum albumin observed in the IL6 transgenic mice were ameliorated by the administration of MR16–1.
CIA in DBA/1J mice is an experimental arthritis model widely used for the evaluation of therapeutic agents for human RA. As inactivation of the IL6 gene completely protected DBA/1J mice from CIA41or it delayed the onset of CIA and also reduced the severity,42 IL6 seems to be required for the development of CIA. Antimouse IL6R antibody treatment also suppressed the development of arthritis and protected knee joints from destructive change in DBA/1J mice immunised with bovine type II collagen.43 Amounts of 0.5 mg, 2 mg, or 8 mg of rat antimouse IL6R antibody, MR16–1, were administered into DBA/1J mice once on the day of the first collagen immunisation. This MR16–1 treatment prevented the development of CIA in a dose dependent manner assessed by a visual scoring system for arthritis in four limbs. Although MR16–1 treatment on the day 3 after the immunisation similarly suppressed the development of arthritis, anti-arthritis effects were not observed when the same dose of MR16–1 was administered on the day 7 or later.43 Taken together with the findings that treatment of CIA with anti-TNFα and anti-IL1 antibodies has been shown to be effective on established murine CIA,44 ,45 IL6 may act earlier in the course of CIA than that of TNFα and IL1.
As a monoclonal antibody recognises a specific antigen epitope, a monoclonal antibody to human antigen epitope does not always cross react with that of other species. The safety and in vivo effect of humanised antihuman IL6R antibody, MRA, on the development of CIA were thus examined in cynomolgus monkeys (Macaca fascicularis) because MRA cross reacts with their IL6R46 but not with that of murine. Joint swelling and stiffness as well as limb oedema appeared at four weeks after the first immunisation with bovine type II collagen with complete adjuvant and increased both in the number and in the degree up to six to eight weeks. Although the inflammation of joints spontaneously decreased, destructive changes remained in the joints. Intravenous administration of MRA (10 mg/kg, once a week) significantly inhibited the onset of joint inflammation as well as the increase of serum CRP, fibrinogen levels and erythrocyte sedimentation rate (ESR) in the monkeys immunised with type II collagen. Histological examination at 14 weeks revealed that pathological changes did not occur in the MRA treated group while synovial proliferation, pannus formation, infiltration of neutrophils, angiogenesis, and cartilage and bone destruction were observed in the joints of the control group monkeys, most of which looked closely like the pathological changes of human RA joints. These findings clearly demonstrate that MRA prevented the development of CIA in cynomolgus monkey. Furthermore, administration of MRA did not affect blood cell, liver, kidney or heart in the cynomolgus monkey.
These data suggest that MRA can be a therapeutic agent for the treatment of human RA.
PATHOLOGICAL SIGNIFICANCE OF IL6 IN CASTLEMAN'S DISEASE
Castleman's disease,47 an atypical lymphoproliferative disorder, can be classified into two types: hyaline-vascular and plasma-cell type according to the histological features of the affected lymph nodes.48 ,49 The latter type is frequently associated with systemic manifestations characterised by chronic inflammatory symptoms such as fever, general fatigue, anaemia, an increased ESR, increased levels of CRP and fibrinogen35 ,48-50 and immunological abnormalities such as polyclonal hyper-γ-globulinaemia, and the presence of autoantibodies. Patients with Castleman's disease frequently show lymphocytic interstitial pneumonia51 and mesangial proliferative glomerulonephritis (MPGN), and sometimes develop autoimmune haemolytic anaemia as complications. Some of these findings resemble those seen in the IL6 transgenic mice. In cases of localised Castleman's disease, these clinical abnormalities may resolve after excision of the affected lymph nodes.35 ,48-50 On the other hand, the multicentric form of Castleman's disease is often refractory to treatment even with corticosteroids or chemotherapy, and consequently the prognosis of such patients is poor. Therefore, a new therapeutic strategy has been required. Recently, Kaposi's sarcoma associated herpesvirus (also called human herpesvirus type 8, KSHV/HHV-8) was reported to be an aetiological agent of this disease, especially in human immunodeficiency virus (HIV) infected patients.52-54
We previously demonstrated constitutive overproduction of IL6 from the germinal centres of hyperplastic lymph nodes and a correlation between serum IL6 levels and clinical abnormalities of patients with plasma-cell type Castleman's disease. And then we suggested that dysregulated IL6 production from affected lymph nodes might be responsible for the systemic manifestations of this disease.35
Beck et al 55 showed that the in vivo administration of murine anti-IL6 neutralising antibody to a patient with Castleman's disease seemed to be therapeutically effective, thus confirming the in vivo function of IL6 in this disease. However, such a therapeutic effect might be transient, either because of the emergence of neutralising human antibodies against murine anti-IL6 antibody or because of the inability to attain serum concentrations of anti-IL6 monoclonal antibody sufficient to neutralise increasing IL6 levels.56 Therefore, the therapeutic value of murine anti-IL6 antibody for human patients remained limited and then humanised anti-IL6R antibody treatment can constitute a new therapeutic strategy for patients with multicentric Castleman's disease.
PATHOLOGICAL SIGNIFICANCE OF IL6 IN RA
RA is a typical immune-inflammatory disease characterised by persistent synovitis with synovial cell proliferation and destructive changes in bone and cartilage of multiple joints. Emergence of rheumatoid factors and increase in platelet counts, γ-globulin, CRP, ESR, and serum amyloid A protein levels and decrease in serum albumin may be explained by uncontrolled IL6 overproduction.57 As IL6 in the presence of soluble IL6R activates osteoclasts to induce bone absorption in vitro,20 and also as anti-IL6 antibody treatment prevented the osteoporosis in vivo in ovariectomised rats,58 IL6 may be involved in the osteoporosis and bone and cartilage destruction of RA. As IL6 can upregulate the expression of intercellular adhesion molecule (ICAM)-1,59 it may recruit immunocompetent cells into the inflammatory tissues. Large amounts of IL6 were indeed observed both in the sera and synovial fluids from the affected joints of RA patients.36-39Taken together, these findings indicate that it is probable that IL6 plays important parts in the pathogenesis of RA. Wendlinget al reported that the administration of mouse monoclonal anti-IL6 antibody to the patients with RA resulted in improvement of symptoms and laboratory findings of RA although the effects were transient.60 The fact confirmed that IL6 plays an important part in this disease.
Treatment of Castleman's diseases and RA with humanised anti-IL6R antibody, MRA
HUMANISED ANTI-IL6R ANTIBODY
To be effective as therapeutic agents administered to patients in repeated doses, mouse antibodies must therefore be engineered to look like human antibodies. Reshaped human PM-1 (rhPM-1) is constructed by grafting the complementarity determining regions (CDR) from mouse PM-1, a specific monoclonal antibody against human IL6R, into human IgG to recreate a properly functioning antigen binding site in a reshaped human antibody.61 rhPM-1 is equivalent to both mouse and chimeric PM-1 in terms of antigen binding and growth inhibition of myeloma cells in vitro.61 ,62 It looks very much like a human antibody and can therefore be expected to have less immunogenicity in vivo in human. rhPM-1 is now named MRA.
We have attempted to inhibit IL6 signal transduction by using this humanised antibody against the human IL6R.
TREATMENT OF CASTLEMAN'S DISEASE
We used humanised anti-IL6 receptor antibody, MRA, to treat seven patients with multicentric plasma-cell type or mixed type Castleman's disease.63 All patients had active disease at the start of MRA treatment, and four of them had previously been treated with prednisolone or immune suppressive agents for more than three months. Three patients had amyloidosis secondary to Castleman's disease, and five had lymphocytic interstitial pneumonia. After obtaining their informed consent and an approval of the Ethical Committee of Osaka University, 50–100 mg of MRA was administered either once or twice weekly. The trough level of serum MRA was 10 μg/ml during maintenance treatment using 50 mg MRA twice a week, and decreased to 5 μg/ml using treatment at 100 mg MRA once a week. There were no differences in responses in terms of constitutional symptoms observed between the two regimens. Ten μg/ml of MRA had previously been proved to inhibit the IL6 induced proliferation of myeloma/plasmacytoma cells in vitro.62 Treatment was well tolerated except for a transient and mild decrease in granulocyte counts on the day after MRA administration in two patients that spontaneously recovered within two days. No decrease in T cell function was observed, assessed either by a skin test with purified protein derivative of tuberculin or by a mixed lymphocyte culture (MLC) test with allogeneic T cells. Representative data of the MRA treatment for Castleman's disease are shown in figure4. Immediately after the MRA administration, fever and fatigue disappeared, and anaemia as well as serum levels of CRP, fibrinogen, SAA and albumin started to improve. After three months of treatment, hyper-γ-globulinaemia and lymphadenopathy were also remarkably alleviated, as were renal function abnormalities in patients with amyloidosis. Autoantibodies such as antinuclear antibody and anti-DNA antibody disappeared after MRA treatment. Histopathological examination of lymph nodes revealed reduction in follicular hyperplasia and vascularity after MRA treatment. The findings imply an important pathogenic mechanism of IL6 in the follicular hyperplasia of affected lymph nodes as well as infiltration of hyaline capillaries with endothelial cell proliferation. These data showed humanised anti-IL6R monoclonal antibody, MRA, can achieve marked responses in the refractory form of this disease without significant adverse reactions or development of neutralising antibodies. It also confirmed the pathophysiological significance of IL6 in Castleman's disease, and blockade of the IL6 signal by MRA may have potential as a new treatment based on the pathophysiological mechanism of multicentric form Castleman's disease.

Improvement in Castleman's disease by humanised anti-IL6R antibody treatment.
TREATMENT OF RA
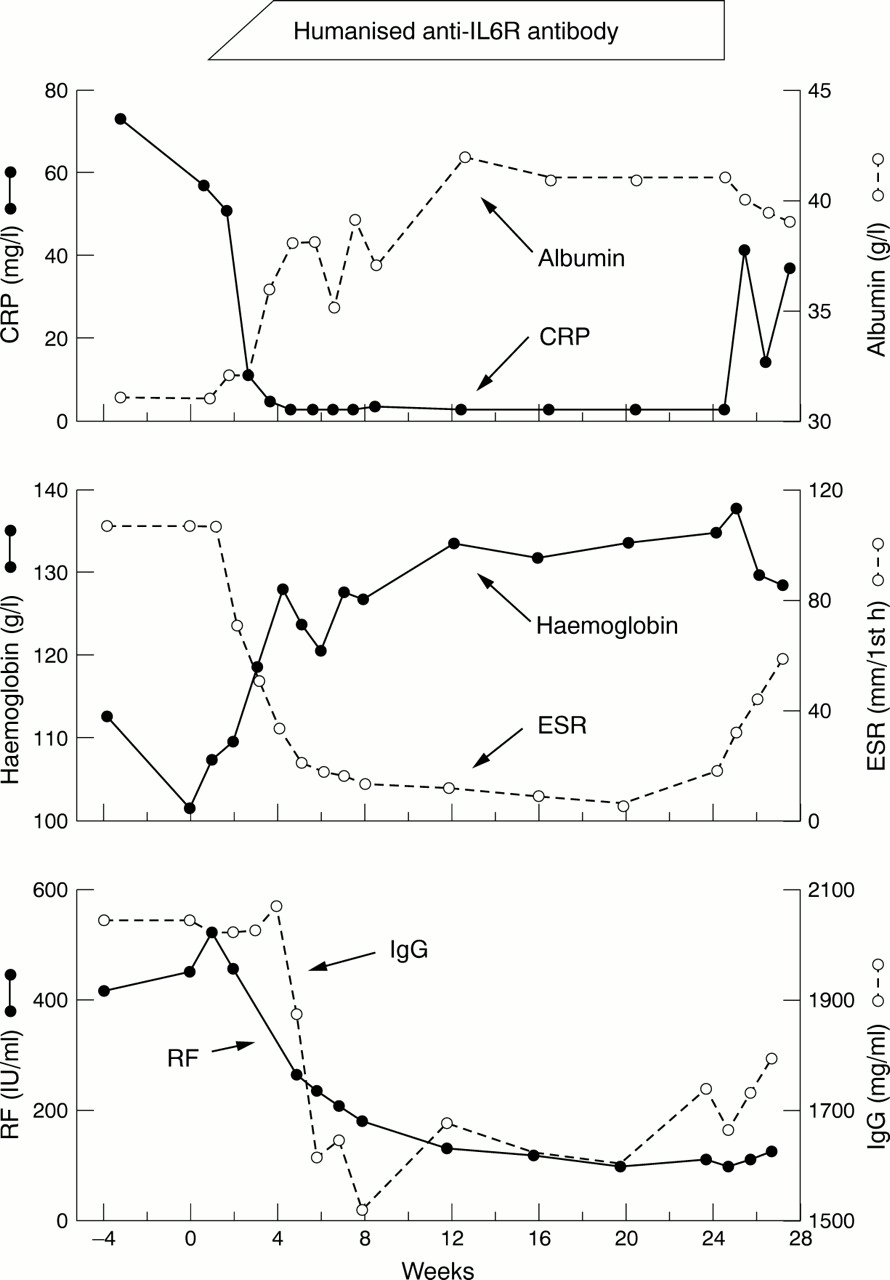
Before the clinical trial of humanised anti-IL6R antibody, MRA, we compassionately treated 11 patients with refractory RA by MRA after obtaining the permission of ethical committee of our institute.57 Before MRA treatment, they all had active disease resistant to any conventional treatment using various disease modifying antirheumatic drugs (DMARDs) including methotrexate, and corticosteroids. The patients were treated with MRA in the same regimen as that for Castleman's disease. The treatment was well tolerated and no major side effect was observed except an appearance of anti-idiotypic antibody in one case, who was therefore withdrawn. Two additional patients were withdrawn: one was because of occurrence of angina attack the relation of which to MRA administration could not be classified, and the other was because of her private reasons. A transit decrease in neutrophil counts mostly within normal range was observed in most of the cases on the next day after MRA administration similarly to Castleman's disease patients. In the eight patients who received the MRA treatment for more than eight weeks, both clinical and biological improvement appeared during the treatment. Representative data of a patient treated with MRA are shown in figure 5. At eight weeks, clinical response was 88% assessed by ACR20 criteria, and 50% by ACR50. Similar response was obtained in the four patients who received MRA treatment for 24 weeks (unpublished data). These results indicate that MRA is relatively safe and useful for the treatment of RA. On the basis of our data, phase I/II clinical trial of MRA in Japan and phase I trial in the United Kingdom are now in progress.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Improvement in RA by humanised anti-IL6R antibody treatment.
Conclusion
Recent progress in the study of immune-inflammatory diseases revealed the pathological significance of some proinflammatory cytokines in the diseases. In addition, the advances in molecular technology made it possible to constitute a new strategy to use humanised monoclonal antibody to modulate the cytokine signals. There are anti-cytokine treatments such as recombinant soluble TNF receptor-Fc fusion protein (Etanercept)64 for RA and chimeric anti-TNFα monoclonal antibody (Infliximab) for RA65 ,66 and Crohn's disease67 already approved in the USA. IL1 receptor antagonist, which blocks IL1 function, and other cytokine inhibitors or even anti-inflammatory cytokine such as IL10 are now under evaluation for their safety and efficacy. Interference of IL6 signal transduction with a humanised anti-IL6 receptor antibody is one of these therapeutic approaches. Each of these agents is to be evaluated specifically for their long term safety and efficacy for these chronic diseases. As many proinflammatory cytokines and immunoregulatory cytokines seem to play an integral part in the pathogenesis of immune-inflammatory disease, combination treatment consisting of some agents may be more effective than that of a single agent. Studies are necessary to understand the intracellular events, such as signal transduction and gene regulation, in the cytokine network which physiologically regulates the over-function of each cytokine in vivo.