
Abstract
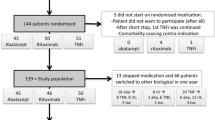
Objective: To compare disease-related medical care and productivity costs, and utilities, in 482 patients with rheumatoid arthritis randomised to receive leflunomide, methotrexate or placebo during a 12-month period.
Design and setting: Prospective pharmacoeconomic analysis of a 1-year randomised double-blind trial set in North America.
Perspective: Societal and the Ontario Ministry of Health.
Methods: Information on healthcare resources, out-of-pocket expenses, loss of working time and time spent on chores, related to the disease or the medication, were collected at 4-week intervals and at study discontinuation. Rating scale and standard gamble (SG) utilities (0 = worse; 100 = best) were collected at baseline and at 6 and 12 months or study exit. Medical care costs in Canadian dollars ($Can) were calculated using Ontario reimbursement schedules. US patients’ expenses were converted to $Can using 1995 purchasing power parity. Lost wages were calculated by age and gender according to 1995 Canadian wage data. All costs were adjusted to 1999 $Can and arithmetic mean costs were compared using the nonparametric bootstrap. Analysis of covariance was performed to compare utilities between groups.
Results: Mean (standard deviation) rating scale values and SG utilities, respectively, for leflunomide, methotrexate and placebo were 67.7 (18.0), 64.8 (18.1) and 57.5 (9.2), and 80.2 (22.1), 83.2 (18.0) and 77.0 (20.5). Both leflunomide and methotrexate had higher rating scale values (p < 0.05) compared with placebo; SG utilities were significantly different between methotrexate and placebo (p < 0.05). Annualised total rheumatoid arthritisb- or drug-related costs for leflunomide, methotrexate and placebo, respectively, were $Can1761, $Can1280 and $Can1324, and medical care costs were $Can753, $Can620 and $Can167 (all costs exclude drug acquisition and monitoring costs). Annual drug acquisition/routine monitoring costs were estimated, respectively, at $Can3853/$Can483 for leflunomide and $Can258/$Can599 for methotrexate. Differences between overall costs (excluding drug acquisition and monitoring costs) and medical care costs were not statistically significant. The costs of treating patients with leflunomide were significantly higher than for methotrexate when drug acquisition and monitoring costs were included (p < 0.0001)
Conclusions: No statistically significant differences in utilities could be found between leflunomide or methotrexate. When drug monitoring and acquisition costs are excluded, leflunomide has an otherwise similar economic profile compared with methotrexate, the current gold standard. The acquisition cost of leflunomide is a driving factor in increasing the costs of therapy. These higher costs need to be assessed relative to the therapeutic value of leflunomide.





Similar content being viewed by others

References
Cooper NJ. Economic burden of rheumatoid arthritis: a systematic review. J Rheumatol 2000: 33
Clarke AE, Zowall H, Levinton C, et al. Direct and indirect medical costs incurred by Canadian patients with rheumatoid arthritis: a 12 year study. J Rheumatol 1997; 24 (6): 1051–60
Anis AH, Tugwell PX, Wells GA, et al. A cost effectiveness analysis of cyclosporine in rheumatoid arthritis. J Rheumatol 1996; 23 (4): 609–16
Kavanaugh A, Heudebert G, Cush J, et al. Cost evaluation of novel therapeutics in rheumatoid arthritis (CENTRA): a decision analysis model. Semin Arthritis Rheum 1996; 25 (5): 297–307
Verhoeven AC, Bibo JC, Boers M, et al. Cost-effectiveness and cost-utility of combination therapy in early rheumatoid arthritis: randomized comparison of combined step-down prednisolone, methotrexate and sulphasalazine with sulphasalazine alone. COBRA Trial Group. Combinatietherapie Bij Reumatoide Artritis. Br J Rheumatol 1998; 37 (10): 1102–9
Strand V, Cohen S, Schiff M, et al. Treatment of active rheumatoid arthritis with leflunomide compared with placebo and methotrexate. Leflunomide Rheumatoid Arthritis Investigators Group. Arch Intern Med 1999; 159 (21): 2542–50
Felson DT, Anderson JJ, Boers M, et al. American College of Rheumatology. Preliminary definition of improvement in rheumatoid arthritis. Arthritis Rheum 1995; 38 (6): 727–35
Canadian Institute for Health Information. CMGTM Directory for Use with Complexity (ICD-9-CM). Canadian Institute for Health Information, 1994
Ontario Ministry of Health. Schedule of Benefits. Physician Services under the Health Insurance Act., 1998. Toronto (ON): Ontario Ministry of Health, 1999
Organization for Economic Cooperation and Development. PPPs and derived indices for all OECD countries [online]. Available from: http://www.oecd.org/pdf/M00009000/M00009294.pdf [accessed 2001 Nov 12]
Canadian Pharmacists Association. Compendium of Pharmaceuticals and Specialties, 1999
Coyle D. Statistical analysis in pharmacoeconomic studies: a review of current issues and standards [see comments]. Pharmacoeconomics 1996; 9 (6): 506–16
Thompson SG, Barber JA. How should cost data in pragmatic randomised trials be analysed? BMJ 2000; 320 (7243): 1197–200
Barber JA, Thompson SG. Analysis of cost data in randomized trials: an application of the non- parametric bootstrap. Stat Med 2000; 19 (23): 3219–36
Gironimi G, Clarke AE, Hamilton VH, et al. Why health care costs more in the US: comparing health care expenditures between systemic lupus erythematosus patients in Stanford and Montreal. Arthritis Rheum 1996; 39 (6): 979–87
Tugwell P, Wells G, Strand V, et al. Clinical improvement as reflected in measures of function and health- related quality of life following treatment with leflunomide compared with methotrexate in patients with rheumatoid arthritis: sensitivity and relative efficiency to detect a treatment effect in a twelve-month, placebo-controlled trial. Leflunomide Rheumatoid Arthritis Investigators Group [published erratum appears in Arthritis Rheum 2000 Jun;43(6):1345]. Arthritis Rheum 2000; 43 (3): 506–14
Verhoeven AC, Bibo JC, Boers M, et al. Cost-effectiveness and cost-utility of combination therapy in early rheumatoid arthritis: randomized comparison of combined step-down prednisolone, methotrexate and sulphasalazine with sulphasalazine alone. COBRA Trial Group. Combinatietherapie Bij Reumatoide Artritis. Br J Rheumatol 1998; 37 (10): 1102–9
Acknowledgements
This study was supported by an unrestricted grant to the Arthritis and Autoimmunity Research Centre from Aventis Canada Inc. The terms of the contract stipulated that the authors should retain the right to absolute control of the methods, conclusions and means of publication of the study. Drs Bombardier, Tugwell, Strand and Wells are consultants to Aventis. Dr. Maetzel is supported by a Ph.D. fellowship (health research) from the Medical Research Council.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Maetzel, A., Strand, V., Tugwell, P. et al. Economic Comparison of Leflunomide and Methotrexate in Patients with Rheumatoid Arthritis. Pharmacoeconomics 20, 61–70 (2002). https://doi.org/10.2165/00019053-200220010-00006
Published:
Issue Date:
DOI: https://doi.org/10.2165/00019053-200220010-00006