Article Text

Statistics from Altmetric.com
The ORAL Surveillance trial found that patients with rheumatoid arthritis (RA) aged ≥50 years with ≥1 additional cardiovascular (CV) risk factor had an increased risk of major adverse cardiovascular events (MACE) with tofacitinib versus tumour necrosis factor inhibitors (TNFi).1 A post hoc analysis indicated that the increased risk of MACE with tofacitinib versus TNFi was apparent primarily in patients with a history of atherosclerotic CV disease (ASCVD), that is, pre-existing coronary artery, cerebrovascular or peripheral artery disease.2
Excess risk of MACE was not identified in the wider tofacitinib RA clinical trial programme (consisting of 21 phase 1–3b/4 and 2 long-term extension studies, hereafter collectively referred to as P123LTE).3 To better understand the results from ORAL Surveillance vs P123LTE, we: (1) applied the ORAL Surveillance CV risk-enrichment criteria to P123LTE (patients who received ≥1 tofacitinib dose) to create a CV risk-enriched P123LTE cohort (P123LTE-CV+; patients aged ≥50 years who had ≥1 additional CV risk factor (current smoker, hypertension, high-density lipoprotein cholesterol <40 mg/dL, diabetes mellitus, history of coronary artery disease)) and (2) assessed MACE incidence rates (IRs) in all patients, and separately in patients with and without history of ASCVD, in P123LTE and P123LTE-CV+.
P123LTE included 7964 patients; of these, 3125 (39.2%) were included in P123LTE-CV+. MACE data were summarised by tofacitinib dose (average 5 or 10 mg two times per day, based on an average total daily dose of <15 or ≥15 mg, respectively). IRs (patients with unique events/100 patient-years) with 95% CI were evaluated for adjudicated MACE and compared with previously published data from ORAL Surveillance.1 2 Adjudication of MACE was performed concurrently in phase 3 studies and retrospectively in phases 1 and 2 studies. Baseline CV risk profiles of P123LTE and P123LTE-CV+were determined as previously described.2 Briefly, patients were grouped according to history of ASCVD, and patients with no history of ASCVD were further grouped by categories of predicted 10-year risk of MACE (high (≥20%), intermediate (≥7.5% to <20%), borderline (≥5% to <7.5%) and low (<5%) risk), per the ASCVD-pooled cohort equations calculator4 with a 1.5-multiplier applied.5
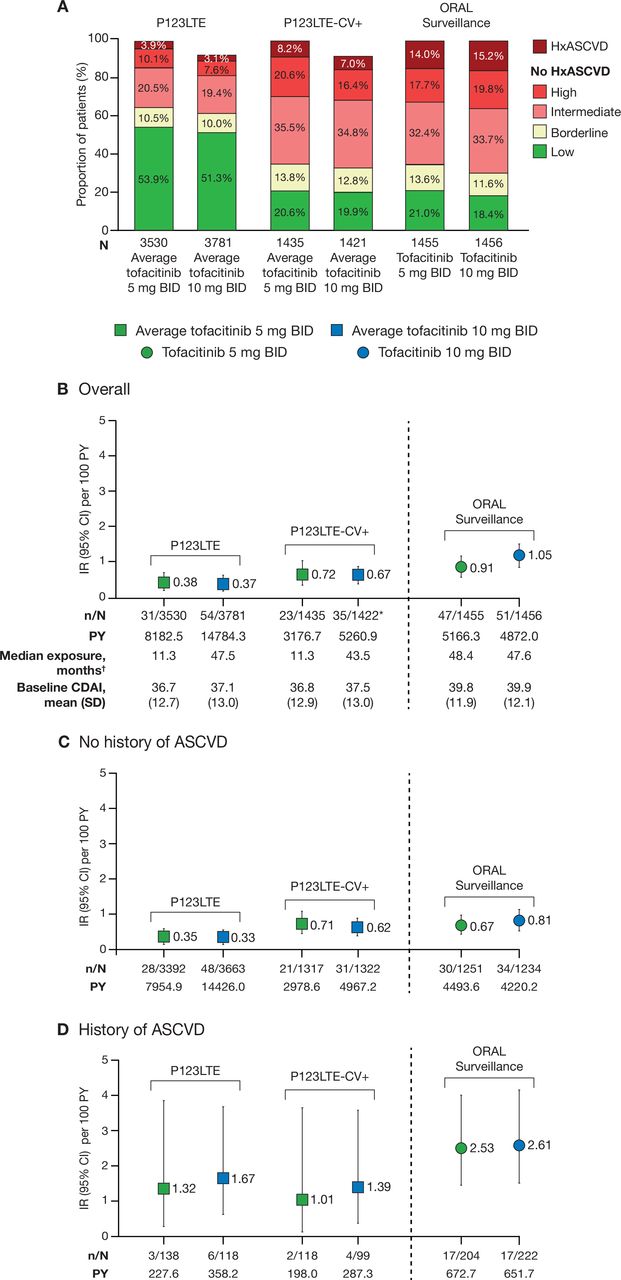
The proportion of patients with a history of ASCVD was higher in ORAL Surveillance (15%) than in P123LTE-CV+ (8%) or P123LTE (4%). Otherwise, the baseline CV risk profile of P123LTE-CV+ was similar to that of ORAL Surveillance (figure 1A).2 Mean baseline disease activity was high across cohorts (figure 1B). MACE IRs were highest in ORAL Surveillance followed by P123LTE-CV+and P123LTE (figure 1B). However, when comparing the patients without history of ASCVD in P123LTE-CV+ and ORAL Surveillance, MACE IRs were similar (figure 1C). There were relatively few patients with history of ASCVD in P123LTE-CV+ and few MACE. Accordingly, due to wide 95% CI for the IRs, differences comparing P123LTE-CV+ and ORAL Surveillance were difficult to interpret (figure 1D).

{kind=link}
Risk of MACE in P123LTE, P123LTE-CV+ and ORAL Surveillance. (A) Baseline risk profiles. Patients without history of ASCVD were categorised according to their 10-year risk of MACE, per the ASCVD-PCE risk calculator4 with a 1.5-multiplier applied.5 The proportions of patients who had no history of ASCVD and were missing ASCVD-PCE risk category data are not shown (P123LTE: average tofacitinib 5 mg two times per day, n=42 (1.2%); average tofacitinib 10 mg two times per day n=321 (8.5%); P123LTE-CV+: average tofacitinib 5 mg two times per day, n=18 (1.3%); average tofacitinib 10 mg two times per day, n=130 (9.1%); ORAL Surveillance: tofacitinib 5 mg two times per day, n=17 (1.2%); tofacitinib 10 mg two times per day, n=18 (1.2%)). (B–D) IRs and 95% CIs (number of patients with first events per 100 PY) for MACE in: (B) all patients; (C) patients with no history of ASCVD; and (D) patients with history of ASCVD. For patients randomised to the tofacitinib 10 mg two times per day group in ORAL Surveillance who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two times per day group. Data for P123LTE cohorts included patients from RA studies (NCT01262118, NCT01484561, NCT00147498, NCT00413660, NCT00550446, NCT00603512, NCT00687193, NCT01164579, NCT00976599, NCT01059864, NCT01359150, NCT02147587, NCT00960440, NCT00847613, NCT00814307, NCT00856544, NCT00853385, NCT01039688, NCT02281552, NCT02187055, NCT02831855, NCT00413699, NCT00661661) with the CV adjudication process applied after 25 February 2009. Data from ORAL Surveillance (NCT02092467) have been published.1 2 *One patient included in the overall analyses was excluded from the analyses by CV risk history due to an inactive Standardised MedDRA Query. †Treatment exposure was assessed in P123LTE as the time between first and last tofacitinib doses (including patients in studies prior to 25 February 2009 with no CV adjudication) and in ORAL Surveillance as the time from randomisation to last contact. ASCVD, atherosclerotic cardiovascular disease; BID, two times per day; CDAI, Clinical Disease Activity Index; CV, cardiovascular; HxASCVD, history of ASCVD; IR, incidence rate; MACE, major adverse CV events; n, number of patients with event; N, number of evaluable patients; P123LTE, Phase 1–3b/4 and long-term extension studies; P123LTE-CV+, CV risk-enriched population of P123LTE; PCE, pooled cohort equations; PY, patient-years; RA, rheumatoid arthritis.
In ORAL Surveillance, markedly higher MACE IRs were reported in tofacitinib-treated patients with history of ASCVD than in patients who had CV risk factors but no history of ASCVD.2 Also, excess risk of MACE with tofacitinib vs TNFi was apparent primarily in patients with history of ASCVD.2 Data from the wider tofacitinib clinical trial programme did not indicate increased risk of MACE compared with placebo or bDMARDs3 6; however, the comparative analyses were limited by smaller samples and shorter exposure than ORAL Surveillance and were not enriched for CV risk.
Results presented here suggest that an important difference between P123LTE and ORAL Surveillance was the proportion of patients with a history of ASCVD (4% and 15%, respectively). While the mechanism and generalisability of these findings require further study, they provide important context regarding the CV safety of tofacitinib in patients without a history of ASCVD.
Ethics statements
Patient consent for publication
Acknowledgments
Select data in this letter were previously presented at EULAR Congress 2022 (Dougados M, Charles-Schoeman C, Szekanecz Z, et al. Ann Rheum Dis 2022;81[Suppl 1]:175–6). The authors would like to thank the patients, investigators and study teams involved in the tofacitinib clinical trial programme. The authors would like to thank Hyejin Jo and Annette Szumski from Syneos Health for contributing to the statistical analyses.
Footnotes
Handling editor Josef S Smolen
Contributors SRY, DLB, JW, CW, KK, CAC and AY conceived or designed the study and data analyses. KK acquired the data. CC-S, JTG, SRY, DLB, JW, CW, KK and AY analysed the data. All authors had access to the data, were involved in interpretation of data, and reviewed and approved the letter’s content before submission.
Funding This study was sponsored by Pfizer. Medical writing support, under the direction of the authors, was provided by Julia King, PhD, CMC Connect, a division of IPG Health Medical Communications, and was funded by Pfizer, New York, New York, USA, in accordance with Good Publication Practice (GPP 2022) guidelines (Ann Intern Med 2022;175:1298–304).
Disclaimer The views expressed in this article are those of the authors and not necessarily those of the National Health Service, the National Institute for Health Research or the Department of Health.
Competing interests MD has acted as a consultant for AbbVie, Bristol-Myers Squibb, Eli Lilly, Merck, Novartis, Pfizer Inc, Roche and UCB; and has received grant/research support from AbbVie, Bristol-Myers Squibb, Eli Lilly, Merck, Novartis, Pfizer Inc, Roche and UCB. CC-S has acted as a consultant for AbbVie, Gilead Sciences, Pfizer Inc and Regeneron-Sanofi; and has received grant/research support from AbbVie, Bristol-Myers Squibb and Pfizer Inc. ZS has acted as an advisor for AbbVie, Eli Lilly, Gedeon Richter, Novartis, Pfizer Inc and Roche; as a consultant for AbbVie, Eli Lilly, Novartis, Pfizer Inc, Roche and Sanofi; has received grant/research support from Pfizer Inc and UCB; and is a member of the Speakers’ Bureau for AbbVie, Eli Lilly, MSD, Novartis, Pfizer Inc, Roche, Sanofi and UCB. JTG has acted as a consultant for AbbVie, Bristol-Myers Squibb, Eli Lilly, Genentech, Gilead Sciences and UCB; and has received grant/research support from Pfizer Inc. SY has acted as a consultant for Corbus, Janssen, Kezar Life Sciences and Pfizer Inc; and has received remuneration from Pfizer Inc for their services as a member of the Steering Committee for ORAL Surveillance. DLB served as a member of the Steering Committee for ORAL Surveillance, with funding from Pfizer Inc paid to Brigham and Women’s Hospital; has served on Advisory Boards for AngioWave, Bayer, Boehringer Ingelheim, Cardax, CellProthera, Cereno Scientific, Elsevier Practice Update Cardiology, High Enroll, Janssen, Level Ex, Medscape Cardiology, Merck, MyoKardia, NirvaMed, Novo Nordisk, PhaseBio, PLx Pharma, Regado Biosciences and Stasys; has served on the Board of Directors for AngioWave (stock options), Boston VA Research Institute, Bristol Myers Squibb (stock), DRS.LINQ (stock options), High Enroll (stock), the Society of Cardiovascular Patient Care and TobeSoft; was the Inaugural Chair for the American Heart Association Quality Oversight Committee; has served as a consultant for Broadview Ventures; has been on Data Monitoring Committees for Acesion Pharma, Assistance Publique-Hôpitaux de Paris, Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Boston Scientific (Chair, PEITHO trial), Cleveland Clinic (including for the ExCEED trial, funded by Edwards), Contego Medical (Chair, PERFORMANCE 2), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo; for the ABILITY-DM trial, funded by Concept Medical), Novartis, Population Health Research Institute and Rutgers University (for the NIH-funded MINT Trial); has received honoraria from the American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ACC.org; Chair, ACC Accreditation Oversight Committee), Arnold and Porter law firm (work related to Sanofi/Bristol-Myers Squibb clopidogrel litigation), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI Clinical Trial Steering Committee funded by Boehringer Ingelheim; AEGIS-II Executive Committee funded by CSL Behring), Belvoir Publications (Editor in Chief, Harvard Heart Letter), Canadian Medical and Surgical Knowledge Translation Research Group (Clinical Trial Steering Committees), Cowen and Company, Duke Clinical Research Institute (Clinical Trial Steering Committees, including for the PRONOUNCE trial, funded by Ferring Pharmaceuticals), HMP Global (Editor in Chief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (Guest Editor; Associate Editor), K2P (Co-Chair, Interdisciplinary Curriculum), Level Ex, Medtelligence/ReachMD (CME Steering Committees), MJH Life Sciences, Oakstone CME (Course Director, Comprehensive Review of Interventional Cardiology), Piper Sandler, Population Health Research Institute (for the COMPASS Operations Committee, Publications Committee, Steering Committee and USA national co-leader, funded by Bayer), Slack Publications (Chief Medical Editor, Cardiology Today’s Intervention), Society of Cardiovascular Patient Care (Secretary/Treasurer), WebMD (CME Steering Committees) Wiley (Steering Committee), Clinical Cardiology (Deputy Editor), NCDR-ACTION Registry Steering Committee (Chair), and VA CART Research and Publications Committee (Chair); holds patent interests in sotagliflozin (named on a patent for sotagliflozin assigned to Brigham and Women’s Hospital who assigned to Lexicon; neither DLB nor Brigham and Women’s Hospital receive any income from this patent); research funding from Abbott, Acesion Pharma, Afimmune, Aker Biomarine, Amarin, Amgen, AstraZeneca, Bayer, Beren, Boehringer Ingelheim, Boston Scientific, Bristol-Myers Squibb, Cardax, CellProthera, Cereno Scientific, Chiesi, CSL Behring, Eisai, Ethicon, Faraday Pharmaceuticals, Ferring Pharmaceuticals, Forest Laboratories, Fractyl, Garmin, HLS Therapeutics, Idorsia, Ironwood, Ischemix, Janssen, Javelin, Lexicon, Lilly, Medtronic, Merck, Moderna, MyoKardia, NirvaMed, Novartis, Novo Nordisk, Owkin, Pfizer Inc, PhaseBio, PLx Pharma, Recardio, Regeneron, Reid Hoffman Foundation, Roche, Sanofi, Stasys, Synaptic, The Medicines Company, 89Bio; royalties from Elsevier (Editor, Braunwald’s Heart Disease); has served as site co-investigator for Abbott, Biotronik, Boston Scientific, CSI, Endotronix, St. Jude Medical (now Abbott), Philips, SpectraWAVE, Svelte, Vascular Solutions; is a trustee for the American College of Cardiology; and has completed unfunded research for FlowCo and Takeda. GGK is a shareholder of IQVIA; has received grant/research support from AbbVie, Acceleron, Amgen, Arena, AstraZeneca, Cytokinetics, Eli Lilly, Gilead Sciences, GlaxoSmithKline, Huya Bioscience International, Johnson is an employee of the University of North Carolina at Chapel Hill; and has served as a member of the Steering Committee for ORAL Surveillance, with funding from Pfizer Inc paid to the University of North Carolina at Chapel Hill. IV, JW, CW, KK, SM, AY and JLR are employees and stockholders of Pfizer Inc. CAC was an employee and stockholder of Pfizer Inc at the time of this analysis. MHB has acted as a consultant for AbbVie, Eli Lilly, Gilead Sciences, and Pfizer Inc; has received grant/research support from Gilead, Pfizer Inc and UCB; is a member of the Speakers’ Bureau for AbbVie; and is supported by the National Institute for Health Research (NIHR) Manchester Biomedical Research Centre and is in receipt of an NIHR Senior Investigator award.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability Upon request, and subject to review, Pfizer Inc will provide the data that support the findings of this study. Subject to certain criteria, conditions and exceptions, Pfizer Inc may also provide access to the related individual de-identified participant data. See https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information.