Article Text

Abstract
Objectives To evaluate malignancies and their associations with baseline risk factors and cardiovascular risk scores with tofacitinib versus tumour necrosis factor inhibitors (TNFi) in patients with rheumatoid arthritis (RA).
Methods In an open-label, randomised controlled trial (ORAL Surveillance; NCT02092467), 4362 patients with RA aged ≥50 years with ≥1 additional cardiovascular risk factor received tofacitinib 5 (N=1455) or 10 mg two times per day (N=1456) or TNFi (N=1451). Incidence rates (IRs; patients with first events/100 patient-years) and HRs were calculated for adjudicated malignancies excluding non-melanoma skin cancer (NMSC), NMSC and subtypes. Post hoc analyses for malignancies excluding NMSC, lung cancer and NMSC included risk factors identified via simple/multivariable Cox models and IRs/HRs categorised by baseline risk factors, history of atherosclerotic cardiovascular disease (HxASCVD) and cardiovascular risk scores.
Results IRs for malignancies excluding NMSC and NMSC were higher with tofacitinib (combined and individual doses) versus TNFi. Risk of lung cancer (most common subtype with tofacitinib) was higher with tofacitinib 10 mg two times per day versus TNFi. In the overall study population, the risk of malignancies excluding NMSC was similar between both tofacitinib doses and TNFi until month 18 and diverged from month 18 onwards (HR (95% CIs) for combined tofacitinib doses: 0.93 (0.53 to 1.62) from baseline to month 18 vs 1.93 (1.22 to 3.06) from month 18 onwards, interaction p=0.0469). Cox analyses identified baseline risk factors across treatment groups for malignancies excluding NMSC, lung cancer and NMSC; interaction analyses generally did not show statistical evidence of interaction between treatment groups and risk factors. HxASCVD or increasing cardiovascular risk scores were associated with higher malignancy IRs across treatments.
Conclusions Risk of malignancies was increased with tofacitinib versus TNFi, and incidence was highest in patients with HxASCVD or increasing cardiovascular risk. This may be due to shared risk factors for cardiovascular risk and cancer.
Trial registration numbers NCT02092467, NCT01262118, NCT01484561, NCT00147498, NCT00413660, NCT00550446, NCT00603512, NCT00687193, NCT01164579, NCT00976599, NCT01059864, NCT01359150, NCT02147587, NCT00960440, NCT00847613, NCT00814307, NCT00856544, NCT00853385, NCT01039688, NCT02281552, NCT02187055, NCT02831855, NCT00413699, NCT00661661
- antirheumatic agents
- arthritis, rheumatoid
- cardiovascular diseases
- tumor necrosis factor inhibitors
Data availability statement
Data are available on reasonable request. On request, and subject to review, Pfizer will provide the data that support the findings of this study. Subject to certain criteria, conditions, and exceptions, Pfizer may also provide access to the related individual deidentified participant data. See https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients with rheumatoid arthritis (RA) have a greater risk of malignancies, including lymphoma and lung cancer, versus the general population. Previous findings from the postauthorisation safety study, ORAL Surveillance, in patients with RA aged ≥50 years with ≥1 additional cardiovascular risk factor demonstrated an increased risk of malignancies with tofacitinib versus tumour necrosis factor inhibitors (TNFi).
Patients with RA have an increased risk of cardiovascular disease, which has itself been associated with an increased risk of cancer. Baseline cardiovascular risk, as a possible predictor of malignancy risk in patients with RA, therefore warrants investigation.
WHAT THIS STUDY ADDS
This study describes the incidence and risk of several subtypes of malignancy and their association with a range of baseline risk factors in patients with RA in ORAL Surveillance beyond those previously reported. The study also assessed the relationship between baseline cardiovascular risk and malignancy risk in patients with RA.
The extended duration of follow-up meant that the risk of a long-latency event such as a malignancy could be more adequately assessed, and in the context of relative risk among patients receiving tofacitinib versus TNFi. In the overall study population, the risk of malignancies excluding non-melanoma skin cancer (NMSC) was similar between tofacitinib and TNFi until month 18 and diverged from month 18 onwards.
Risk factors of interest were identified across all treatment groups via post hoc Cox regression models for a composite endpoint of all malignancies excluding NMSC, lung cancer and NMSC, and were generally consistent with the literature. Incidence of malignancy events was increased in patients with versus without these risk factors across treatments and tended to be higher with tofacitinib versus TNFi. However, interaction analysis generally did not identify baseline risk factors with a differential effect on treatment comparisons.
Across all treatment groups, the incidence of malignancies was highest among patients with a history of atherosclerotic cardiovascular disease (ASCVD) or high baseline cardiovascular risk score versus those with low baseline cardiovascular risk scores; patients with malignancy events had higher mean baseline cardiovascular risk scores than those without malignancies.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These findings, including the higher incidence of malignancies in patients with a history of ASCVD and those with higher baseline cardiovascular risk, may assist in the assessment of the risk–benefit profile of tofacitinib and inform treatment decisions for patients with RA with increased cardiovascular risk.
Introduction
Rheumatoid arthritis (RA) is a chronic systemic immune-mediated inflammatory condition.1 Patients with RA have approximately a 10% increase in overall malignancy risk compared with the general population,2 and a notably higher risk of developing certain malignancies, including lymphoma and lung cancer.2–4 Identifying risk factors for malignancies in patients with RA is important for cancer screening and optimising disease management. High RA disease activity and long-term use of disease-modifying antirheumatic drugs (DMARDs), such as methotrexate, appear to increase malignancies risk,5 6 while use of biological DMARDs and non-steroidal anti-inflammatory drugs reduces the risk of certain malignancies.7 8 The relationship between targeted synthetic DMARDs and malignancies requires further study. Risk of cardiovascular disease, as determined by validated risk-prediction tools, is known to be associated with an increased risk of cancer in the general population, suggesting shared risk factors and pathophysiology.9–11
ORAL Surveillance was a postauthorisation safety study that assessed the relative risk of major adverse cardiovascular events (MACE) and malignancies excluding non-melanoma skin cancer (NMSC) for tofacitinib versus tumour necrosis factor inhibitors (TNFi). To enrich for cardiovascular risk, the study enrolled patients with RA who were aged ≥50 years and had ≥1 additional cardiovascular risk factor.12 For both outcomes, the combined tofacitinib doses (5 and 10 mg two times per day) did not demonstrate non-inferiority versus TNFi as the upper limit of the HR 95% CI was >1.8 (prespecified non-inferiority criterion).12
Here, we characterise malignancy events and evaluate the potential associations of baseline risk factors and cardiovascular risk with malignancies in a cardiovascular risk-enriched RA population from the ORAL Surveillance study.
Methods
Study design and patients
ORAL Surveillance (NCT02092467) was a phase IIIb/IV randomised, parallel-group, open-label, safety endpoint study conducted from March 2014 to July 2020 in patients with moderate to severe RA who were ≥50 years of age with ≥1 additional cardiovascular risk factors (see the online supplemental material). Key exclusion criteria included current or previous malignancy, except adequately treated NMSC or cervical cancer in situ; there were no prespecified screening procedures for malignancies. Full inclusion and exclusion criteria have been reported separately.12 Coprimary endpoints in ORAL Surveillance were adjudicated MACE and malignancies excluding NMSC.
Supplemental material
Patients were randomised 1:1:1 to receive open-label oral tofacitinib 5 or 10 mg two times per day or a subcutaneous TNFi (adalimumab 40 mg every 2 weeks (North America) or etanercept 50 mg once weekly (rest of the world; ROW)). Background methotrexate was continued at the prestudy stable dose, unless modification was clinically indicated. In February 2019, the tofacitinib 10 mg two times per day dose was reduced to 5 mg two times per day as a major protocol amendment following observations of increased frequency of pulmonary embolism with tofacitinib 10 mg two times per day versus TNFi, and an increase in overall mortality with tofacitinib 10 mg two times per day versus 5 mg two times per day and TNFi.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Outcomes
All malignancies were adjudicated as described in the online supplemental material. Malignancies assessed included a composite of all malignancies excluding NMSC, NMSC and cancer subtypes, which comprised the malignancies excluding NMSC outcomes. Cancer subtypes of interest included breast cancer (female patients only), lymphoma, lung cancer (including non-small cell lung cancer and small cell lung cancer), melanoma, prostate cancer (male patients only), colorectal cancer and pancreatic cancer.
Statistical analysis
Analyses were performed using the safety analysis set, which included all randomised patients who received ≥1 dose of trial drug. All patients, including those required to switch from tofacitinib 10 to 5 mg two times per day in February 2019, were analysed in their originally randomised group, with data after the dosage switch included in the tofacitinib 10 mg two times per day group. This analysis also included a combined tofacitinib group, which pooled patients randomised to tofacitinib 5 or 10 mg two times per day.
Malignancy events were counted within a predefined risk period. For malignancies excluding NMSC and its subtypes, this was based on total time (time from the first study dose to last contact date (ie, maximum of event start date, event stop date, last visit date, withdrawal date, telephone contact date or death date)). For NMSC and its subtypes, this was based on 28-day on-treatment time (time from the first study dose to last study dose date +28 days or to last contact date, whichever was earlier). Patients without events were censored at the end of the risk period.
Crude incidence rates (IRs) were expressed as the number of patients with first events per 100 patient-years, along with exact Poisson two-sided 95% CIs.13 HRs and 95% CIs for tofacitinib doses relative to TNFi and for tofacitinib 10 vs 5 mg two times per day were estimated, based on separate Cox proportional hazard models (for comparing combined tofacitinib doses vs TNFi and for pairwise comparisons among treatment groups), with treatment groups (combined tofacitinib doses and TNFi; tofacitinib 5 mg two times per day, tofacitinib 10 mg two times per day and TNFi, in their respective models) as the only covariate.14 In this analysis, for malignancy subtypes, HRs >1 and 95% CIs excluding 1, which corresponded to nominal p<0.05, were interpreted as increased risk.
The number needed to harm (NNH)15 was based on the IR difference of tofacitinib versus TNFi. Positive NNH was defined as the number of patient-years of tofacitinib exposure needed for one more patient to report an additional event versus TNFi; negative NNH was defined as the reverse. The number of patients exposed for 5 years needed to harm was calculated by dividing the number of patient-years needed to harm by 5. NNH was evaluated post hoc for malignancies excluding NMSC, lung cancer and NMSC.
Cumulative probabilities of patients not experiencing a first malignancy (excluding NMSC) at specific time intervals after initiation of each treatment were measured post hoc using Kaplan-Meier estimates of the survivor function. In a piecewise exponential hazard model analysis,16 HRs (95% CIs) were analysed for malignancies excluding NMSC, with one change-point used to divide the timeline into two periods. Two fixed change-points were considered: month 18 (day 540) and month 24 (day 720). Treatment-by-period interaction two-sided p values were calculated based on the difference of the two log-hazard differences (tofacitinib dose group vs TNFi) between the two periods (period 1 vs period 2), using large sample approximation.
Post hoc simple and multivariable Cox models were used to evaluate potential baseline risk factors (online supplemental table 1) for malignancies excluding NMSC, lung cancer and NMSC. Further details on the Cox regression analyses are provided in the online supplemental material. A Cox model with interaction terms, including treatment groups, baseline risk factor and the treatment-group-by-baseline-risk-factor interaction as covariates, was performed to assess whether the treatment effect on the time to event differed across levels of the baseline risk factor. A small interaction p value suggests the presence of such a differential treatment effect.
IRs and HRs for malignancies excluding NMSC, lung cancer and NMSC were provided by baseline risk factors identified in multivariable analyses, by baseline methotrexate dose (>15 vs ≤15 mg/week (15 mg/week was the median dose at baseline)) and by age and smoking status at baseline (aged ≥65 years or ever smoked vs aged 50 to <65 years and never smoked).
IRs for malignancies excluding NMSC, lung cancer and NMSC were also provided by history of atherosclerotic cardiovascular disease (HxASCVD; defined as having a history of at least one of the following: myocardial infarction, coronary heart disease, coronary artery procedure, stable angina pectoris, cerebrovascular disease (stroke or carotid atherosclerosis), peripheral artery disease or ASCVD (undefined)). In line with a recent analysis,17 patients without HxASCVD were further categorised according to their baseline 10-year risk of MACE (low: <5%; borderline: ≥5% to <7.5%; intermediate: ≥7.5% to <20%; high ≥20%). This was calculated by risk scores obtained using the ASCVD-Pooled Cohort Equations calculator (ASCVD-PCE),18 multiplied by 1.5 to align with recommendations from the European Alliance of Associations for Rheumatology19 20 to account for increased cardiovascular risk in patients with RA.
IRs of malignancies excluding NMSC, lung cancer and NMSC from ORAL Surveillance were compared with those from phase I–IIIb/IV and long-term extension studies from the tofacitinib RA clinical development programme (online supplemental table 2; further methods are described in the online supplemental material).
In all analyses, due to their post hoc and exploratory nature, no multiple comparison adjustments were made to the nominal p values. All analyses were completed by using SAS V.9.4 (Linux) (Copyright 2022 SAS Institute).
Results
Patients
Overall, 4362 patients were randomised and treated in ORAL Surveillance (tofacitinib 5 mg two times per day: N=1455; tofacitinib 10 mg two times per day: N=1456; combined tofacitinib doses: N=2911; TNFi: N=1451). Exposure to last trial treatment was 5073.5, 4773.4 and 4940.7 patient-years for tofacitinib 5 mg two times per day, tofacitinib 10 mg two times per day or TNFi, respectively.12 For the tofacitinib 10 mg two times per day group, the exposure prior to the protocol amendment (ie, before patients randomised to tofacitinib 10 mg two times per day had their dose reduced to 5 mg two times per day) accounted for approximately 79% of the total exposure; approximately 21% of exposure occurred after patients had switched to tofacitinib 5 mg two times per day. Median (range) duration of treatment was 44.7 (0.03–69.8), 42.8 (0.03–71.7), 43.9 (0.03–71.7) and 44.0 (0.03–71.1) months for tofacitinib 5 mg two times per day, tofacitinib 10 mg two times per day, combined tofacitinib doses and TNFi, respectively. Patient demographics and baseline disease characteristics were generally similar across treatments; when comparing North America versus ROW, patients in North America were less likely to be female and more likely to be aged ≥65 years, white or to be a past smoker. Overall, the mean (SD) age of patients was 61.2 (7.1) years, 78.2% (n=3410) were female and 48.2% (n=2103) were current or past smokers. The mean (SD) duration of RA across all treatment groups was 10.4 (9.1) years. Selected baseline disease characteristics, overall and by geographical region, are presented in table 1; full characteristics have been reported previously.12
Patient demographics and baseline disease characteristics in ORAL Surveillance (safety analysis set)
Incidence and risk of malignancies
Overall, 164 (3.8%) patients in ORAL Surveillance reported a malignancy excluding NMSC, and 80 (1.8%) patients reported ≥1 NMSC (table 2). For malignancies excluding NMSC, IRs were higher for individual and combined tofacitinib doses versus TNFi and similar between tofacitinib doses. ORAL Surveillance demonstrated an HR of 1.48 (95% CI 1.04 to 2.09) for combined tofacitinib doses versus TNFi; similar HRs were observed for each tofacitinib dose (table 2). This did not meet non-inferiority criteria (HR 95% CI upper limit <1.8) for combined tofacitinib doses versus TNFi.12 IRs for cancer subtypes of interest are shown in table 2; additional cancer subtypes are shown in online supplemental table 3. Further details of patients with malignancies can be found in online supplemental table 4. The most frequently reported malignancy excluding NMSC among tofacitinib-treated patients was lung cancer (1.0%, primarily non-small cell lung cancer); the risk of lung cancer was higher in patients treated with tofacitinib 10 mg two times per day versus TNFi. Breast cancer was the most frequently reported malignancy excluding NMSC for TNFi (0.9%) among female patients; there were no apparent differences in risk of breast cancer across treatments. Lymphoma was reported in 0.3% and 0.1% of patients on tofacitinib and TNFi, respectively; IRs were numerically higher with both tofacitinib doses versus TNFi (table 2). The risk for NMSC was higher for individual and combined tofacitinib doses versus TNFi. NNHs versus TNFi for malignancies excluding NMSC, lung cancer and NMSC were 276 and 275, 929 and 525, and 348 and 272 patient-years, respectively, for tofacitinib 5 and 10 mg two times per day (table 2). This corresponded to 55 patients for malignancies excluding NMSC (for both tofacitinib doses), 186 and 105 patients for lung cancer, and 70 and 54 patients for NMSC, who would need to be treated with tofacitinib 5 and 10 mg two times per day, respectively, for 5 years to have one additional event compared with TNFi (table 2).
IRs (patients with first events/100 PY; 95% CI) and HRs (95% CIs) for malignancies excluding NMSC and subtypes of interest (total time), and NMSC and subtypes of interest (28-day on-treatment time) in ORAL Surveillance
Over 66 months, >93% of patients did not have a malignancy excluding NMSC event, across treatments. Based on visual inspection of the Kaplan-Meier plot (figure 1) and the results from the piecewise exponential hazard models at fixed change-points of 18 and 24 months (table 3), the change-point in rates among treatment groups occurred at month 18. The cumulative probabilities of patients not having a malignancy event were similar between both tofacitinib doses and TNFi until month 18 (ie, HRs <1 and 95% CI including 1 for tofacitinib vs TNFi) and diverged from month 18 onwards (HRs >1.8 and 95% CI excluding 1 for tofacitinib vs TNFi) (change-point analysis at month 18, table 3). Treatment-by-period interaction p values were lower at the month 18 vs month 24 change-point, suggesting that piecewise HRs were different before and after month 18, but were not different before and after month 24, across tofacitinib doses (table 3).
Piecewise HRs (95% CI) for malignancies excluding NMSC based on a piecewise exponential hazard model at fixed change-points of 18 and 24 months and treatment-by-period interaction 2-sided p values

Kaplan-Meier plot of the probability of patients without adjudicated malignancies excluding NMSC. Please also see Ytterberg et al (2022)12 online supplemental figure S4C, which presents the probability of patients with adjudicated malignancies excluding NMSC. For patients randomised to the tofacitinib 10 mg two times per day group who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two times per day group. For malignancies excluding NMSC, the risk period was total time, defined as time from first dose of trial drug until last contact date. P values are based on two simple Cox proportional hazard models (one for comparing combined tofacitinib doses vs TNFi, and the other for comparing tofacitinib 5 and 10 mg two times per day vs TNFi), with treatment as the only covariate. *Includes patients who received tofacitinib 5 or 10 mg two times per day in ORAL Surveillance. BID, two times per day; NMSC, non-melanoma skin cancer; TNFi, tumour necrosis factor inhibitors.
Independent baseline risk factors associated with malignancies excluding NMSC, lung cancer and NMSC in ORAL Surveillance
Results from the simple Cox analyses for malignancies excluding NMSC, lung cancer and NMSC are shown in online supplemental figure 1. Across treatment groups, risk factors identified in the multivariable model (p<0.05) for malignancies excluding NMSC included older age, current or past smoking, race (white), geographical location (North America) and history of chronic lung disease (chronic obstructive pulmonary disease or interstitial lung disease) (figure 2A). Risk factors identified for lung cancer and NMSC across treatment groups (p<0.05) are shown in figure 2B,C, respectively. Notably, the risk for lung cancer was lower among patients with RA disease duration of ≥10 years vs <1 year, and race (non-white) and baseline COX-1 or COX-2 inhibitor use were associated with a decreased risk of NMSC. Generally, interaction analysis of treatment groups by each candidate risk factor did not identify any baseline risk factors with a differential effect on treatment comparisons (online supplemental table 5).
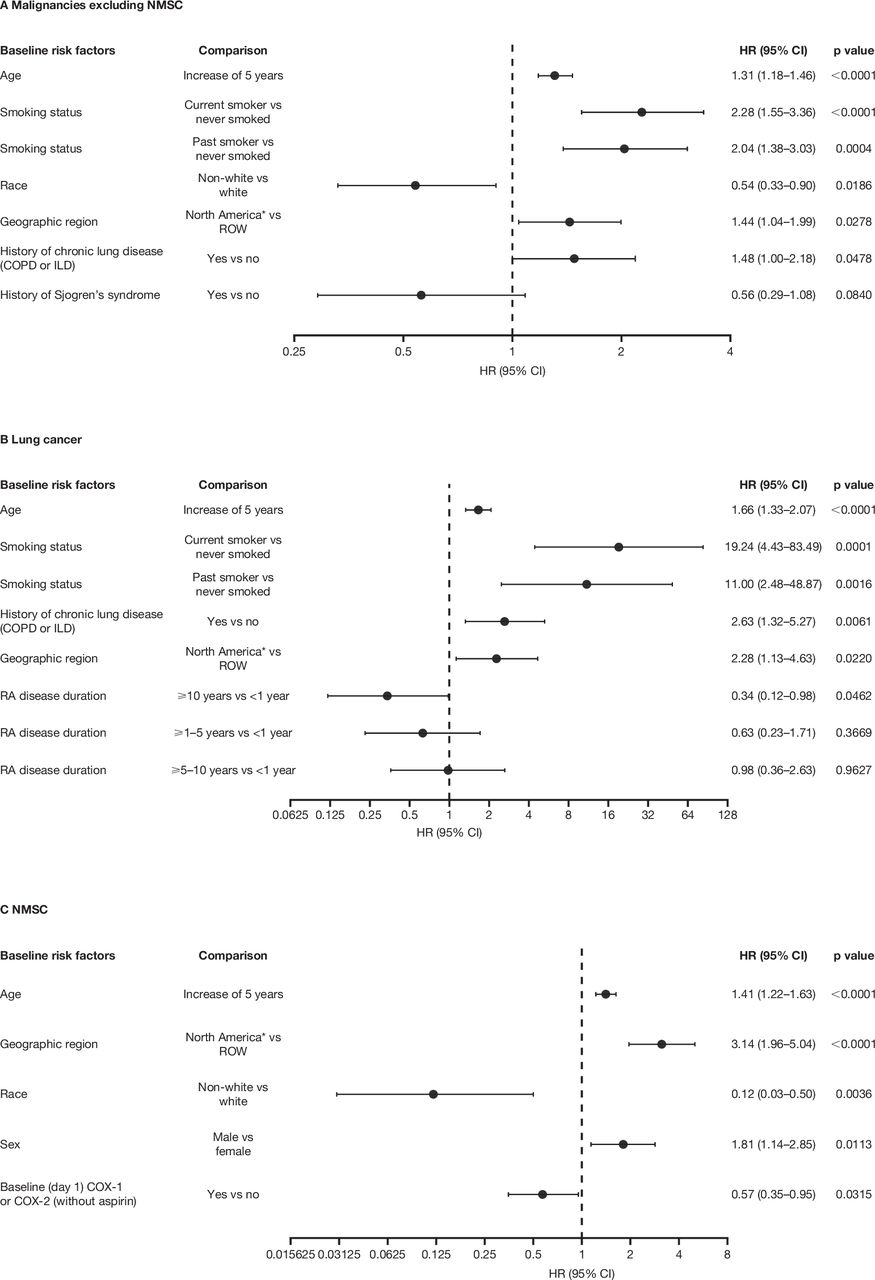
Multivariable analyses of baseline risk factors across treatment groups for (A) malignancies excluding NMSC, (B) lung cancer and (C) NMSC in ORAL Surveillance. Results for baseline risk factors were based on multivariable Cox model using a backward selection algorithm including treatment groups (tofacitinib 5 mg two times per day, tofacitinib 10 mg two times per day and TNFi; not subject to selection) and a set of potential baseline risk factors pre-selected from simple Cox models (results are shown in online supplemental figure 1). A risk factor was retained in the final multivariable model if the risk factor had a p value <0.10 and was considered predictive if the p value was <0.05. For patients randomised to the tofacitinib 10 mg two times per day group who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two times per day group. For malignancies excluding NMSC and lung cancer, the risk period was total time, defined as the time from first dose of trial drug until last contact date. For NMSC, the risk period was the 28-day on-treatment time, defined as the time from first until last dose of trial drug + 28 days, or to last contact date, whichever was earlier. HRs (95% CIs) are shown on a logarithmic scale. *USA, Puerto Rico and Canada. COPD, chronic obstructive pulmonary disease; COX, cyclooxygenase; ILD, interstitial lung disease; NMSC, non-melanoma skin cancer; RA, rheumatoid arthritis; ROW, rest of the world; TNFi, tumour necrosis factor inhibitors.
Incidence and risk of malignancies excluding NMSC, lung cancer and NMSC, by risk factors of interest
Although there was generally no strong statistical evidence of interactions between treatment groups and the risk factors, incidence and risk of malignancies excluding NMSC (online supplemental figure 2), lung cancer (figure 3 and online supplemental figure 3) and NMSC (online supplemental figure 4) were provided by all baseline risk factors with p<0.05 in the multivariable Cox model. Across treatments, IRs for all outcomes were numerically higher among patients aged ≥65 vs 50 to <65 years, aged ≥65 years or ever smoked vs aged 50 to <65 years and never smoked, and in North America versus ROW. Patients who were current or past smokers had numerically higher IRs for malignancies excluding NMSC and lung cancer across treatments than patients who never smoked. Risk of lung cancer was not apparently different between current and past smokers versus patients who had never smoked for tofacitinib 5 mg two times per day and TNFi (95% CIs for HRs included 1) but was increased with tofacitinib 10 mg two times per day, although 95% CIs were wide (HRs (95% CI) 7.57 (1.61 to 35.67) and 8.75 (1.82 to 42.22), respectively). Among current and past smokers, IRs were numerically higher with either tofacitinib dose versus TNFi, with overlapping 95% CIs; HRs did not show an apparent difference in risk between treatments. IRs for malignancies excluding NMSC and NMSC were numerically higher for patients who were white versus non-white. In general, among patients with risk factors, IRs tended to be numerically higher with tofacitinib versus TNFi.

Risk of lung cancer with tofacitinib versus TNFi by smoking status in ORAL Surveillance: (A) IRs (patients with first events/100 PY; 95% CIs) and (B) HRs (95% CIs). For patients randomised to the tofacitinib 10 mg two times per day group who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two times per day group. For lung cancer, the risk period was total time, defined as time from first dose of trial drug until last contact date. HRs (95% CIs) are shown on a logarithmic scale. *Includes patients who received tofacitinib 5 or 10 mg two times per day in ORAL Surveillance. BID, two times per day; IR, incidence rate; N, number of evaluable patients; N, number of patients with events; NI, non-informative (HRs (95% CI) were not informative when the total number of patients with events was ≤2 for the corresponding pair of treatments in the comparison, or when one of the treatments in the comparison had 0 events); PY, patient-years; TNFi, tumour necrosis factor inhibitors.
When considering baseline methotrexate dose, IRs of malignancies excluding NMSC, lung cancer and NMSC were numerically higher in patients treated with baseline methotrexate >15 vs ≤15 mg/week across all treatments (online supplemental figure 5). Among patients with baseline methotrexate dose ≤15 mg/week, those treated with tofacitinib 10 mg two times per day had a numerically higher risk of NMSC versus TNFi (online supplemental figure 5C).
Incidence and risk of malignancies excluding NMSC, lung cancer and NMSC by HxASCVD and baseline cardiovascular risk score
Tofacitinib-treated patients with a HxASCVD had numerically higher IRs of malignancies excluding NMSC, lung cancer and NMSC than TNFi-treated patients (figure 4 and online supplemental figure 6). In patients without a HxASCVD, higher mean baseline ASCVD risk scores were observed for patients with versus without malignancies excluding NMSC, lung cancer and NMSC (table 4). Across treatments, the IRs for malignancies excluding NMSC, lung cancer and NMSC were low in patients with low or borderline risk scores and generally increased in patients with increasing baseline ASCVD risk scores (figure 4 and online supplemental figure 6). IRs of malignancies excluding NMSC were generally higher in patients from North America versus ROW, regardless of baseline ASCVD risk score; IRs generally increased with increasing baseline ASCVD risk scores for both geographical regions (online supplemental figure 7).
Baseline ASCVD risk scores for patients in ORAL Surveillance with and without malignancies excluding NMSC, lung cancer and NMSC

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Malignancies excluding NMSC with tofacitinib versus TNFi by HxASCVD and baseline ASCVD risk scores in ORAL Surveillance. IRs and HRs for malignancies excluding NMSC overall have been presented previously.12 For patients randomised to the tofacitinib 10 mg two times per day group who had their dose of tofacitinib reduced to 5 mg two times per day, the data collected after patients were switched to tofacitinib 5 mg two times per day were counted in the tofacitinib 10 mg two times per day group. The risk period was total time, defined as time from first dose of trial drug until last contact date. *Includes patients who received tofacitinib 5 or 10 mg two times per day in ORAL Surveillance. †In patients without a HxASCVD. ASCVD, atherosclerotic cardiovascular disease. BID, two times per day; HxASCVD, history of atherosclerotic cardiovascular disease; IR, incidence rate; N, number of evaluable patients; N, number of patients with events; NMSC, non-melanoma skin cancer; PY, patient-years; TNFi, tumour necrosis factor inhibitors.
Incidence of malignancies excluding NMSC and NMSC in the tofacitinib RA clinical development programme, overall and by baseline cardiovascular risk
As shown in online supplemental table 6, the IRs for malignancies excluding NMSC, lung cancer and NMSC with tofacitinib were higher in ORAL Surveillance compared with other studies from the tofacitinib RA clinical programme. As expected, the cardiovascular risk was generally lower in the overall tofacitinib cohort (54% of patients had low baseline ASCVD scores vs 20% in ORAL Surveillance). When criteria mimicking ORAL Surveillance were applied to data from the tofacitinib RA clinical programme, 3125/7964 patients (39.2%) met the inclusion criteria (cardiovascular risk-enriched cohort). Baseline ASCVD risk scores in this cardiovascular risk-enriched cohort broadly mirrored those of ORAL Surveillance; trends between patients with versus without malignancies were similar across both cohorts (online supplemental table 7). In general, higher baseline ASCVD scores appeared to be associated with higher risk of malignancies (online supplemental table 7). In the cardiovascular risk-enriched cohort of tofacitinib-treated patients from the tofacitinib RA clinical programme, IRs for malignancies excluding NMSC and for NMSC were generally higher in patients with a HxASCVD and high baseline ASCVD risk scores (online supplemental figure 8).
Discussion
This study details the incidence and baseline risk factors of malignancies in patients with RA aged ≥50 years with ≥1 additional cardiovascular risk factor who participated in ORAL Surveillance. While associations between baseline cardiovascular/malignancy risk and RA have been previously studied independently,2 4 21–24 these analyses focus on the risk of malignancies, and associated risk factors, in a cardiovascular risk-enriched RA population.
The IRs for malignancies excluding NMSC (coprimary endpoint) and NMSC were higher with combined doses of tofacitinib versus TNFi; similar findings were identified with each tofacitinib dose versus TNFi. IRs for lymphoma and lung cancer, which are known to be increased in patients with RA versus the general population, were consistent with previous reports.2 4 IRs for lymphoma were higher in patients treated with tofacitinib versus TNFi, although the number of cases reported in the TNFi treatment group in this study (n=1) were lower than previous reports.25–27 In addition, in the overall study population, the risk of malignancies excluding NMSC with tofacitinib versus TNFi was consistent through month 18 and diverged beyond that time; correspondingly, treatment-by-period interaction p values demonstrated that there was a stronger interaction between treatment duration and the risk of malignancies excluding NMSC at month 18 (before vs after), compared with month 24 (before vs after). These findings are in line with a recent real-world study in patients with RA, which demonstrated that in patients ≥50 years of age with CV risk factors, a numerically increased risk of malignancies was observed with tofacitinib versus TNFi. The study did not demonstrate an increased risk of malignancies with tofacitinib versus TNFi in the overall RA population; however, it was limited by the short follow-up period (mean follow-up of <1 year).28 Physicians should be aware of the signs and symptoms that may be associated with the development of malignancies, and the risks versus the benefits for each patient should be assessed.
Risk factors identified in these multivariable analyses for all outcomes included increasing age and geographical location in North America. Notably, a higher proportion of patients in North America had cardiovascular risk factors (as per the ORAL Surveillance study inclusion criteria), were past smokers and were aged ≥65 years at baseline compared with ROW.12 Across treatments, current or past smoking and history of chronic lung disease were identified as risk factors for malignancies excluding NMSC and lung cancer, while male sex and no baseline COX-1 or COX-2 inhibitor use were risk factors for NMSC. However, while protective effects of COX inhibitors against cancer have been reported, evidence is emerging that nonsteroidal anti-inflammatory drugs, including COX inhibitors, may increase risk for some cancer types.29 30 Therefore, this particular finding should be interpreted with caution. Race (non-white) led to lower risk of malignancies excluding NMSC and NMSC, although the latter should also be interpreted with caution, as 77% of patients in ORAL Surveillance were of white race and light-coloured skin is known to be a risk factor for NMSC.31 32 RA disease duration of ≥10 years (vs <1 year) appeared to reduce the risk of lung cancer. A history of Sjogren’s syndrome and RA disease duration of ≥1 to <5 years and ≥5 to <10 years did not confer higher risk for malignancies excluding NMSC, lung cancer and NMSC. In patients with these risk factors, compared with those without, the incidence of malignancy events was increased across all treatment groups and was generally higher in patients with tofacitinib versus TNFi. Taken together, these findings indicate that patients taking tofacitinib 5 mg two times per day, tofacitinib 10 mg two times per day or TNFi who are older (≥65 years), have ever smoked and have a history of chronic lung disease may be at increased risk of malignancies.
While age, race and sex have been previously established as risk factors for NMSC,33 further studies with larger patient numbers are required to elucidate a potential association between longer RA disease duration (≥10 vs <1 years) and decreased risk of lung cancer, beyond assumed better control of patients’ chronic medical conditions. This may be an artefact of the relatively long follow-up period and the distribution of age in the trial. The risk of NMSC was higher with tofacitinib 10 mg two times per day versus TNFi among patients receiving methotrexate at a baseline dose of ≤15 mg/week; no apparent difference was observed in the risk of malignancies excluding NMSC or lung cancer. Increased risk of skin cancer in patients with RA treated with low-dose methotrexate (<20 mg/week) has been previously established34; increased risk of NMSC with methotrexate has also been demonstrated.35
Patients with RA are known to have an increased risk of cardiovascular morbidity and mortality,36 37 and emerging evidence indicates shared risk factors and pathophysiology between cardiovascular disease and cancer.9–11 Lau et al recently identified an association between 10-year ASCVD risk scores and risk of certain cancer subtypes, including lung cancer in US and Dutch cohorts.9 The analyses from our study assess a unique angle of whether baseline cardiovascular risk scores in patients with RA can predict malignancy risk. Our findings show, across treatments, the incidence of malignancies was higher in patients with a HxASCVD and with increasing baseline ASCVD risk scores. Across all treatments, patients with malignancies had higher baseline mean ASCVD scores than those without malignancies. Similar findings were observed in pooled studies from the wider tofacitinib RA clinical programme. Within baseline ASCVD risk categories, higher rates of malignancies excluding NMSC were generally observed in patients from North America versus ROW. Certain risk factors for malignancies identified in this study, including smoking and older age, are common factors independently associated with the development of RA (and response to RA treatment), increased cardiovascular risk and development of different cancer types.38–42 Additional studies are required to further clarify associations between cardiovascular risk scores and malignancies in patients with RA.
Limitations of this analysis include that ORAL Surveillance was not powered to assess comparisons for malignancy subtypes across treatment groups. The post hoc analyses for evaluating baseline risk factors were exploratory rather than confirmatory, thereby not implying causation. The smaller patient numbers and fewer events for certain risk factors categories could limit the estimation of within-risk-factor comparisons, and no adjustments were made when reporting p values. In addition, while malignancies were adjudicated centrally for standardisation across investigational sites, different countries may have had different practices regarding staging and grading of tumours, and there was no specified screening procedure at baseline. Although geographical region was identified as a risk factor for malignancies, ORAL Surveillance was not able to disentangle the influence of region from the possibility of a drug-specific effect for adalimumab versus etanercept, since region and TNFi use were completely confounded. Finally, we recognise that use of the 1.5-multiplier applied to the ASCVD-PCE calculator to account for the influence of RA is a crude approximation, and may have suboptimal calibration for patients with malignancies.20 It should also be noted that the results from this study are reflective of a cardiovascular risk-enriched RA population, as per the inclusion criteria (~40% of all patients in the tofacitinib RA clinical programme), and therefore, the importance of assessing cardiovascular risk in the RA population for informed treatment decisions should be emphasised.
Conclusions
In patients with RA aged ≥50 years with ≥1 additional cardiovascular risk factor, the risk of adjudicated malignancies excluding NMSC, lung cancer and NMSC were increased with tofacitinib versus TNFi. Lung cancer was the most frequently reported malignancy in tofacitinib-treated patients. In addition, in the overall study population, the risk of malignancies excluding NMSC with tofacitinib was consistent with that of TNFi up to month 18 and diverged beyond that time. In general, independent risk factors identified through multivariable Cox analyses across all treatment groups were consistent with the literature; interaction analysis of treatment groups by each baseline risk factor generally did not identify risk factors with a differential effect on treatment comparisons. The incidence of all malignancies was higher in patients with a HxASCVD and with increasing cardiovascular risk scores for patients treated with tofacitinib and TNFi, potentially due to common factors associated with increased cardiovascular and malignancy risk.
Data availability statement
Data are available on reasonable request. On request, and subject to review, Pfizer will provide the data that support the findings of this study. Subject to certain criteria, conditions, and exceptions, Pfizer may also provide access to the related individual deidentified participant data. See https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was conducted in compliance with the Declaration of Helsinki, Good Clinical Practice Guidelines of the International Council for Harmonisation and local regulations. Patients provided written informed consent. The protocol, amendments and consent documentation were approved by the Institutional Review Board or Independent Ethics Committee for each centre. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
Select data in this manuscript were previously presented at ACR Convergence 2021.43 The authors would like to thank the patients, investigators and study teams involved in the study. Medical writing support, under the guidance of the authors, was provided by Tanya Guha, PhD, and Lauren Hogarth, MSc, CMC Connect, a division of IPG Health Medical Communications, and was funded by Pfizer, New York, New York, USA, in accordance with Good Publication Practice (GPP 2022).44
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Contributors DLB, LMG, NS and CAC conceived or designed the study and data analyses. CAC, CW and JW acquired data. KY, DLB, LMG, NS, CAC, CW, JW and IV analysed the data. All authors had access to the data, were involved in interpretation of data and reviewed and approved the manuscript’s content before submission. JRC accepts final responsibility for this work and controlled the decision to publish.
Funding This study was sponsored by Pfizer.
Competing interests JRC has received research/grant support from Amgen, CorEvitas, Crescendo Bio and Pfizer; and is a consultant for AbbVie, Amgen, Bristol-Myers Squibb, CorEvitas, Eli Lilly, Janssen, Myriad, Pfizer, Roche/Genentech and UCB. KY has received research/grant support from Astellas Pharma, Eisai Pharma, Eli Lilly Japan KK, GlaxoSmithKline, Mitsubishi Tanabe Pharma, MSD, Pfizer and Teijin Pharma; is a consultant for AbbVie, Asahi Kasei Pharma, Astellas Pharma, Eli Lilly Japan KK, Gilead GK, Japan Tobacco and Pfizer; and is part of speakers’ bureau for AbbVie, Actelion Pharmaceuticals Japan, Asahi Kasei Pharma, Astellas Pharma, AYUMI Pharma Co., Boehringer Ingelheim Japan, Bristol-Myers Squibb, Chugai Pharma, Daiichi Sankyo, Eli Lilly Japan KK, Eisai Pharma, Gilead GK, GlaxoSmithKline, Hisamitsu Pharma Co., Janssen, Japan Tobacco, Mitsubishi Tanabe Pharma, MSD, Nippon Kayaku, Nippon Shinyaku, Ono Pharma, Otsuka Pharma, Pfizer, Sanofi and Takeda. Y-HC has received research/grant support from AbbVie, Agnitio Science & Technology, Astellas Pharma, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Chugai Pharma Taiwan, GlaxoSmithKline, Johnson & Johnson, MSD, National Yang-Ming University, Novartis, Pfizer, Roche, Sanofi, Taiwan Ministry of Science and Technology, Taiwan Department of Health and Welfare, Taichung Veterans General Hospital and UCB; and is a consultant for AbbVie, AstraZeneca, Astellas Pharma, Bristol-Myers Squibb, Chugai Pharma Taiwan, Inova Diagnostics, Eli Lilly, Johnson & Johnson, GlaxoSmithKline, MSD, Novartis, Roche, Sanofi, Thermo Fisher Scientific, UCB and United Biopharma. DLB served as a member of the Steering Committee for ORAL Surveillance, with funding from Pfizer paid to Brigham and Women’s Hospital. He is a member of the advisory board for: AngioWave, Bayer, Boehringer Ingelheim, Cardax, CellProthera, Cereno Scientific, Elsevier Practice Update Cardiology, High Enroll, Janssen, Level Ex, Medscape Cardiology, Merck, MyoKardia, NirvaMed, Novo Nordisk, PhaseBio, PLx Pharma, Regado Biosciences, Stasys; Board of Directors: AngioWave (stock options), Boston VA Research Institute, Bristol-Myers Squibb (stock), DRS.LINQ (stock options), High Enroll (stock), Society of Cardiovascular Patient Care, TobeSoft; Chair: Inaugural Chair, American Heart Association Quality Oversight Committee; Data Monitoring Committees: Acesion Pharma, Assistance Publique-Hôpitaux de Paris, Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Boston Scientific (Chair, PEITHO trial), Cleveland Clinic (including for the ExCEED trial, funded by Edwards), Contego Medical (Chair, PERFORMANCE 2), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi Sankyo; for the ABILITY-DM trial, funded by Concept Medical), Novartis, Population Health Research Institute; Rutgers University (for the NIH-funded MINT Trial); Honoraria: American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ACC.org; Chair, ACC Accreditation Oversight Committee), Arnold and Porter law firm (work related to Sanofi/Bristol-Myers Squibb clopidogrel litigation), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee funded by Boehringer Ingelheim; AEGIS-II executive committee funded by CSL Behring), Belvoir Publications (Editor in Chief, Harvard Heart Letter), Canadian Medical and Surgical Knowledge Translation Research Group (clinical trial steering committees), Cowen and Company, Duke Clinical Research Institute (clinical trial steering committees, including for the PRONOUNCE trial, funded by Ferring Pharmaceuticals), HMP Global (Editor in Chief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (Guest Editor; Associate Editor), K2P (Co-Chair, interdisciplinary curriculum), Level Ex, Medtelligence/ReachMD (CME steering committees), MJH Life Sciences, Oakstone CME (Course Director, Comprehensive Review of Interventional Cardiology), Piper Sandler, Population Health Research Institute (for the COMPASS operations committee, publications committee, steering committee, and USA national co-leader, funded by Bayer), Slack Publications (Chief Medical Editor, Cardiology Today’s Intervention), Society of Cardiovascular Patient Care (Secretary/Treasurer), WebMD (CME steering committees), Wiley (steering committee); Other: Clinical Cardiology (Deputy Editor), NCDR-ACTION Registry Steering Committee (Chair), VA CART Research and Publications Committee (Chair); Patent: Sotagliflozin (named on a patent for sotagliflozin assigned to Brigham and Women's Hospital who assigned to Lexicon; DLB/Brigham and Women's Hospital do not receive any income from this patent); Research Funding: Abbott, Acesion Pharma, Afimmune, Aker Biomarine, Amarin, Amgen, AstraZeneca, Bayer, Beren, Boehringer Ingelheim, Boston Scientific, Bristol-Myers Squibb, Cardax, CellProthera, Cereno Scientific, Chiesi, CSL Behring, Eisai, Ethicon, Faraday Pharmaceuticals, Ferring Pharmaceuticals, Forest Laboratories, Fractyl, Garmin, HLS Therapeutics, Idorsia, Ironwood, Ischemix, Janssen, Javelin, Lexicon, Lilly, Medtronic, Merck, Moderna, MyoKardia, NirvaMed, Novartis, Novo Nordisk, Owkin, Pfizer, PhaseBio, PLx Pharma, Recardio, Regeneron, Reid Hoffman Foundation, Roche, Sanofi, Stasys, Synaptic, The Medicines Company, 89Bio; Royalties: Elsevier (Editor, Braunwald’s Heart Disease); Site Co-Investigator: Abbott, Biotronik, Boston Scientific, CSI, Endotronix, St. Jude Medical (now Abbott), Philips, SpectraWAVE, Svelte, Vascular Solutions; Trustee: American College of Cardiology; Unfunded Research: FlowCo, Takeda. LMG, NS, CW, JW, SM and IV are shareholders and employees of Pfizer. CAC was a shareholder and employee of Pfizer at the time of this analysis. JJG-R has received research/grant support from AbbVie, MSD, Pfizer and Roche; is a consultant for Pfizer; and is part of speakers’ bureau for AbbVie, Biogen, Bristol-Myers Squibb, Janssen, MSD, Pfizer and Roche.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.