Article Text

Abstract
Objectives To develop EULAR recommendations for screening and prophylaxis of chronic and opportunistic infections in patients with autoimmune inflammatory rheumatic diseases (AIIRD).
Methods An international Task Force (TF) (22 members/15 countries) formulated recommendations, supported by systematic literature review findings. Level of evidence and grade of recommendation were assigned for each recommendation. Level of agreement was provided anonymously by each TF member.
Results Four overarching principles (OAP) and eight recommendations were developed. The OAPs highlight the need for infections to be discussed with patients and with other medical specialties, in accordance with national regulations. In addition to biologic/targeted synthetic disease-modifying antirheumatic drugs (DMARDs) for which screening for latent tuberculosis (TB) should be performed, screening could be considered also before conventional synthetic DMARDs, glucocorticoids and immunosuppressants. Interferon gamma release assay should be preferred over tuberculin skin test, where available. Hepatitis B (HBV) antiviral treatment should be guided by HBV status defined prior to starting antirheumatic drugs. All patients positive for hepatitis-C-RNA should be referred for antiviral treatment. Also, patients who are non-immune to varicella zoster virus should be informed about the availability of postexposure prophylaxis should they have contact with this pathogen. Prophylaxis against Pneumocystis jirovecii seems to be beneficial in patients treated with daily doses >15–30 mg of prednisolone or equivalent for >2–4 weeks.
Conclusions These recommendations provide guidance on the screening and prevention of chronic and opportunistic infections. Their adoption in clinical practice is recommended to standardise and optimise care to reduce the burden of opportunistic infections in people living with AIIRD.
- Tuberculosis
- Autoimmune Diseases
- Antirheumatic Agents
Statistics from Altmetric.com
Introduction
Opportunistic and chronic infections, that is, those which present more commonly or more severely in people who are immunocompromised,1 are encountered in the setting of autoimmune inflammatory rheumatic diseases (AIIRD) and are often associated with immunosuppressive and immunomodulatory treatments used for these diseases. Although it is recognised that screening procedures and prophylactic measures should be followed, clinical practice is largely heterogeneous and relevant recommendations are often lacking or are disparately located across the literature. There is, therefore, a need for collating evidence for different AIIRD and treatment regimens to be used as a single point of reference in routine clinical practice.2 3
Setting a single set of guidelines for infection screening and prophylaxis is challenging, as recommendations and procedures cannot be unified across all infections and organisms due to differences in area of residence, type of AIIRD and associated risk, the antirheumatic treatment received and other factors that may present additional layers of complexity, such as age and comorbidities.4–6 Our goal was to formulate a set of recommendations, taking these challenges into account, to inform rheumatologists and healthcare providers in their decision making when caring for people living with AIIRD, to ensure that these infections can be identified and adequately managed.
A EULAR Task Force (TF) has been formed, comprised healthcare professionals and patients across different disciplines and countries, to develop the first EULAR recommendations for screening and prophylaxis of chronic and opportunistic infections in patients living with AIIRD based on the best available scientific evidence. This manuscript presents the work of this TF and the final set of recommendations.
Methods
The EULAR standardised operating procedures (SOP)7 were followed throughout the undertaking of this work. The project was approved by the EULAR executive committee (No: CLI 118). The steering committee included a main convenor (KLH) and a co-convenor (JG), one methodologist (EN), a co-methodologist (DSC) and a main fellow (GEF). Two co-fellows (MD and SSZ) supported the undertaking of the systematic literature review (SLR),8 especially during validation steps (see below). TF members were selected based on their experience in the field of infections in the setting of AIIRD, considering also gender and regional equity. The final TF consisted of 22 people (including steering committee members) from 15 different European countries. Two patient research partners, two healthcare professionals in rheumatology, two infectious disease doctors with an interest in rheumatology and one pulmonologist were included in addition to rheumatologists/epidemiologists (including two Emerging EULAR Network (EMEUNET) members).
In preparation of the first TF meeting, the steering group identified research questions of interest and relevance, leading to a scoping review (available on request) by the fellow (GEF). The scoping review provided an overview of the existing literature on chronic and opportunistic infections in AIIRD. During the first TF meeting, which was held virtually in September 2020, the results of the scoping review were presented and the research questions for the main SLR were discussed and modified as deemed appropriate by the TF. In addition, there was review and discussion on the pathogens that would be included in the subsequent SLR (presented in online supplemental material 1), based on the findings of the scoping review as well as expert opinion of TF members including the two infectious disease doctors who reviewed separately the list of pathogens.
Supplemental material
Afterwards, the steering committee transformed the research questions (online supplemental material 1) into epidemiological questions that were addressed via the SLR. The latter was registered in PROSPERO (No: CRD42021244732) and was performed as per guidance provided in the Cochrane Handbook.9 The SLR results were reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.10
The SLR was performed for studies published from inception up to 5 December 2021. However, new studies that were published after this date and up until the date of the second TF meeting (18 January 2022) were also considered, where these provided additional evidence relevant to the research questions. The SLR focused on studies examining the efficacy of screening and prophylaxis for chronic and opportunistic infections. Results as well as details about the methodology of the SLR are presented separately. The results of the SLR were presented in the second virtual meeting (split over December 2021 and January 2022) during which the overarching principles (OAPs) and the recommendations were formulated and voted on. Recommendations and OAPs were accepted if ≥75% of the members agreed in a first round of anonymised voting; if this agreement was not reached, the recommendation/OAPs were reworded with a voting cut-off of ≥67%. If this was not achieved, voting in favour by >50% of the TF members was required as part of a third and final round of voting, after rephrasing. As per EULAR guidance,7 the Oxford Evidence Based Medicine categorisation was followed for applying level of evidence and grade of recommendation (GoR).11 A research agenda was formed, based on the identified unmet need and gaps in the literature found via the SLR and in discussions between TF members. Finally, after the second meeting, TF members provided their level of agreement which each OAP and recommendation from 0 (=no agreement) to 10 (=full agreement), via an anonymised online survey.
Results
These recommendations address the screening procedures and prevention measures that should be followed in people living with AIIRD, treated (or about to be treated) with antirheumatic drugs. After the identification of the pathogens that were covered in the respective SLR, extensive discussions took place (during the second meeting) about the nomenclature that should be followed for the various antirheumatic drugs used. The TF reached consensus (agreed by 88% of the TF members) on the use of a four-category system as follows: (1) biological (b) and targeted synthetic (ts)-disease-modifying antirheumatic drugs (DMARDs): all biological and ts-DMARDs (except apremilast), (2) conventional synthetic (cs)DMARDs: methotrexate, leflunomide. Sulfasalazine and hydroxychloroquine were exempted from this category, and the TF members agreed to name them specifically, if needed, as it was thought that they only have a mild immunomodulatory/immunosuppressive effect. (3) other immunosuppressants: cyclophosphamide, mycophenolate mofetil, azathioprine, ciclosporin, tacrolimus. (4) glucocorticoids. These categories were adopted, with some modifications from recently published expert opinion and other consensus papers. It is recognised that the rheumatology community should discuss and reach a final consensus about the terminology used to describe these drugs.12–14 The term ‘antirheumatic treatment/drugs’ is also used in this manuscript, encompassing all the above-mentioned categories. The TF meetings resulted in the formulation of four OAPs and eight recommendations (table 1).
The EULAR recommendations for screening and prophylaxis of chronic and opportunistic infections in adults with autoimmune inflammatory rheumatic diseases
Overarching principles
OAPs form the basis on which the recommendations were built. They reflect the rationale behind the development of this set of recommendations and they highlight key concepts in the management of AIIRD. In total, four OAPs that apply across all recommendations were formulated and met with high consensus by the TF (table 1).
The risk of chronic and opportunistic infections should be considered and discussed with all patients with AIIRD prior to treatment with csDMARDs, tsDMARDs, bDMARDs, immunosuppressants and/or glucocorticoids and reassessed periodically
Chronic and opportunistic infections are an important aspect of AIIRD and a significant cause of morbidity and mortality.15 16 This principle was regarded as the cornerstone of all formulated recommendations. Antirheumatic treatment is a widely accepted risk for infections and thus the respective risk should be explained and discussed with patients, including how these risks can be minimised. The association of high disease activity with increased infection rates should also be considered.17 18 Shared-decision making is increasingly recognised as an important component of good clinical care in the management of people living with AIIRD,19–22 who should also be educated to identify promptly signs and symptoms of infections and how to seek relevant medical attention. Considering also that escalation or change in treatment might be necessary and late reactivation of latent infections is possible, the respective risk should be reassessed and discussed periodically.
Collaboration between rheumatologists and other specialists including but not limited to infectious disease doctors, gastroenterologists, hepatologists and pulmonologists is important
Rheumatologists carry primary responsibility when it comes to the treatment of people living with AIIRD and should work in close collaboration with other specialties when planning prevention or management of chronic and opportunistic infections in patients receiving antirheumatic drugs. This is an important component of multidisciplinary care and particularly relevant in the setting of these recommendations. Given that tuberculosis (TB) and hepatitis are among the most commonly discussed infections in people with AIIRD, teamwork with pulmonologists and hepatologists/gastroenterologist, respectively, is important. Other specialties including infectious disease doctors, radiologists, haematologists and microbiologists also have a crucial role in guiding the screening and prophylaxis of chronic and opportunistic infections in patients with AIIRD.
Individual risk factors should be considered in the decision for screening and prophylaxis of chronic and opportunistic infections and reassessed periodically
An individualised approach has been identified as a key principle of this set of recommendations, since several factors are known to increase the susceptibility for specific preventable infections.4–6 23–25 These include, but are not limited to, age, comorbidities (eg, lung disease), cotreatment with other medications and travelling/living in endemic areas. Given that these parameters can change, and that escalation in the treatment of AIIRD is not unusual (OAP A), the presence of risk factors for chronic and opportunistic infections should be reassessed periodically. From this point of view, medical history including previous infections, lifestyle (eg, frequent travelling), habits (eg, smoking), vaccination status and previous countries of residence should be taken into account.
National guidelines and recommendations, among other country/region-level factors pertaining to endemic infectious diseases, should be considered
It was recognised by the TF members that there are significant variations in the strategies followed across different regions/countries. This might reflect differences in the geoepidemiology of certain pathogens, as well as in factors related to cost and/or availability. To give an example, TB is more prevalent in specific areas of the world and/or resistance of Mycobacterium tuberculosis varies across countries,26 reflecting in the use of different therapeutic regimes/schemes for prophylaxis against latent TB reactivation. From this point of view, the TF thought it appropriate to have as an OAP that national/regional recommendations should always be taken into consideration in addition to these recommendations.
Recommendations
Screening for latent tuberculosis is recommended in patients prior to starting bDMARDs or tsDMARDs. Screening should also be considered in patients with increased risk for latent tuberculosis prior to starting csDMARDs, immunosuppressants and/or glucocorticoids (according to dose and duration).
Screening for latent TB before starting bDMARDs is included in screening programmes of most national and international rheumatology associations, while the same applies for tsDMARDs, although there is less evidence.27–32 On the other hand, there is some evidence that patients with AIIRD under treatment with csDMARDs and/or glucocorticoids have also increased risk for latent TB reactivation.29 33–37 The minimum dose/duration of glucocorticoids above which latent TB screening should be performed, is unknown. A number of studies and other guidelines have suggested that screening should be considered particularly in those patients likely to receive >15 mg of prednisolone (or equivalent)/day for longer periods of time (eg, >4 weeks).34 35 38 39 In addition, screening for latent TB before commencement of these drugs should be considered in patients who also have accompanying TB risk factors like alcohol abuse, smoking, living with people with TB, living in endemic countries and others.23 40 Finally, despite being suggested that cyclophosphamide might associate with TB development in some AIIRD,23 41 evidence specifically addressing the impact of immunosuppressants is lacking. Recommendation for immunosuppressants at the time of drafting these recommendations, is only based on expert opinion.
Screening for latent tuberculosis should follow national and/or international guidelines and would typically include a chest X-ray, and interferon-gamma release assay (IGRA) over tuberculin skin test (TST) where available.
Evidence suggests that IGRA performs better than TST in the diagnosis of latent TB and is less affected by treatment with glucocorticoids, DMARDs or immunosuppressants.42–51 From this point of view, IGRA should be preferred over TST for TB screening. Given the low agreement between TST and IGRA,42 44 52–71 performing both tests can also be considered in cases of high suspicion for latent TB and/or in high-endemic countries.58 70 72 Concordance between different IGRAs (Quantiferon and EliSPOT) is good thus one is not recommended over the other.47 73–75 In addition, although there is no robust evidence for the usefulness of chest X-Ray, the TF considered it appropriate that this should be included in the TB- screening procedures, especially as a negative IGRA or TST cannot exclude active TB or rule out latent TB.76 Finally, as discussed in the SLR informing current recommendations, conversion (from negative to positive) of TST or IGRA after treatment with bDMARDs has been reported.63 70 77–89 Therefore, periodic rescreening could be considered, especially if risk factors exist or develop over time.23 40 There are no robust data to define how often re-screening should be performed and/or if there is a need to rescreen patients who switch bDMARDs or tsDMARDs; this issue has been added in the research agenda. As stated, given the regional differences in TB-burden and also issues (eg, cost) that might affect the availability of some investigations (eg, Quantiferon), national and international guidelines should also be followed, where available.
Choice and timing of latent tuberculosis therapy should be guided by national and/or international guidelines. Special attention should be given to interactions with drugs commonly used to treat AIIRD.
Various therapeutic schemes have been used for the treatment of latent TB. These include isoniazid for 6–12 months, combination of rifampicin/isoniazid for 3–4 months, rifampicin for 4 months and once-weekly therapy of isoniazid plus rifapentine.29 72 77 83 90–107 Given differences in the TB-burden and drug resistances among regions/countries, the TF members advise adhering to relevant national guidelines.
Interactions between drugs used to treat AIIRD and those used as treatment for latent TB should be considered. Monitoring of liver function tests (LFTs) is necessary in patients cotreated with isoniazid and hepatotoxic drugs like methotrexate and leflunomide.96 108 109 In addition, pharmacokinetics of JAK-inhibitors and glucocorticoids might be affected by coadministration with rifampicin.110 111
All patients being considered for treatment with csDMARDs, bDMARDs, tsDMARDs, immunosuppressants and glucocorticoids (according to dose and duration) should be screened for hepatitis B virus
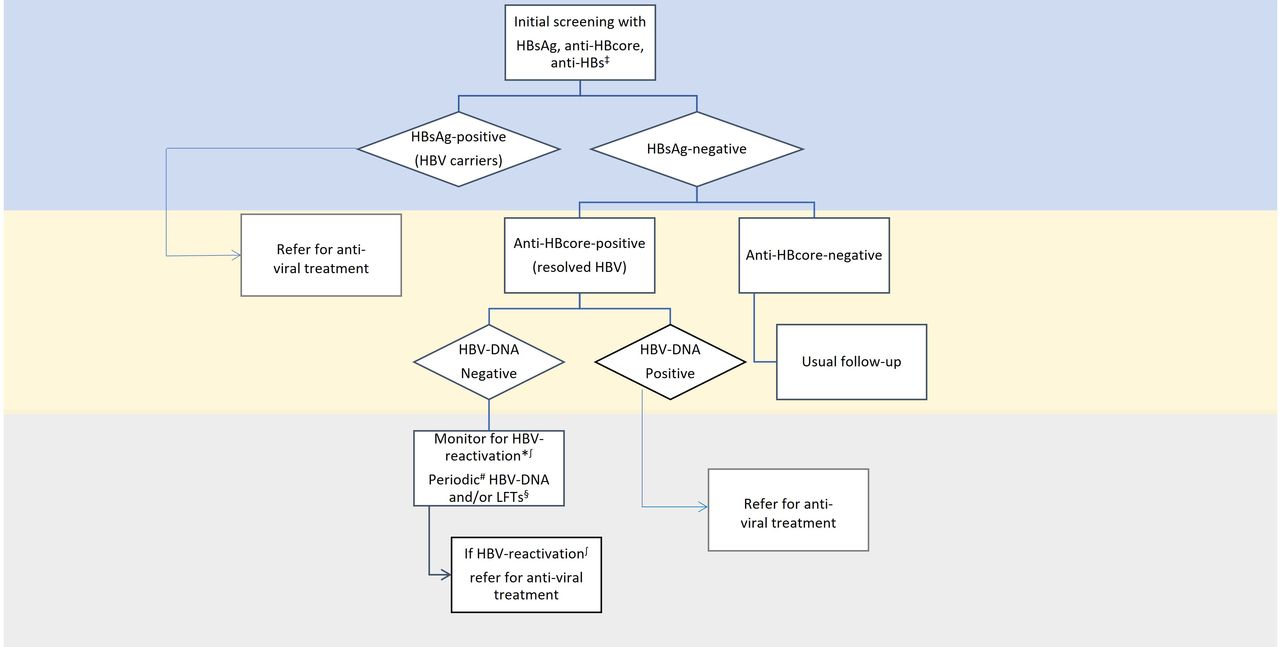
The risk of hepatitis B virus (HBV) reactivation (appearance/rise in HBV-DNA or conversion from HBsAg-negative to HBsAg-positive)112 depends on the HBV-status (unexposed, vaccinated, carrier (ie, HBsAg-positive) and resolved-HBV (anti-HBcore-positive and HBsAg-negative)) and this should be determined before the treatment for AIIRD is commenced. HBV-status would also help identify patients at risk (eg, from their occupation) who should be vaccinated.113 Due to the complex nature of this recommendation, the TF decided to include a figure outlining the suggested procedures according to the HBV status of the patient (figure 1).
{kind=link}
Typical screening for hepatitis B virus (HBV) status include HBsAg, anti-HBcore and anti-HBs. HBsAg-positive patients (HBV carriers) would benefit from prophylactic treatment, and thus it is advised that they should be referred to hepatologist for anti-viral prophylactic treatment. For those who are anti-HBcore-positive and HBsAg-negative (resolved HBV), measurement of HBV-DNA and liver function tests at baseline and then regular monitoring is advised. If HBV reactivation is suspected, based on these tests, referral to hepatologist for anti-viral treatment is recommended. For high-risk patients (eg, commencing treatment with anti-CD20 regimes) prophylactic treatment, irrespective of DNA levels might be considered. ‡Positive anti-HBs without positive HBsAg or anti-HBcore is consistent with prior vaccination. If all three (HBsAg, anti-HBcore, anti-HBs) are negative, means no previous exposure to HBV. *Consider referral for antiviral prophylaxis for those commencing rituximab, having also low titers of anti-HBs. Risk is assessed on an individual basis. ∫HBV-reactivation: rise or appearance of HBV-DNA, or conversion from HBsAg-negative to HBsAg-positive. #Periodic: there are no data to specify the exact time at which re-screening for HBV-reactivation should be performed. However, every 3–6 months is the standard for many national guidelines. Risk factors and cost should also be considered. §Referral to hepatologists is also recommended.
Evidence suggests that HBV carriers (HBsAg-positive) would benefit from prophylactic treatment, and thus it is advised that they should be referred to hepatologist for antiviral prophylactic treatment.114 115 As outlined in the SLR informing these recommendations, data are less robust for drugs116–125 other than bDMARDs.126–136 However, for non-bDMARDs users, referral to a hepatologist for consideration of anti-viral prophylaxis is also recommended. The exact dose and duration of glucocorticoids that would increase HBV reactivation risk cannot be inferred from existing studies. Patients receiving at least 10 mg of prednisolone or equivalent for ≥4 weeks are regarded by the American Gastroenterology Association137 as a high-risk group for HBV reactivation, also supported by expert opinion.138 139
For patients who have resolved-HBV (anti-HBcore-positive and HBsAg-negative), risk for HBV reactivation is lower.119 121–123 140–148 Baseline measurement of LFT and HBV-DNA levels and then regular (eg, every 3–6 months) monitoring of LFT and HBV-DNA levels over universal prophylaxis is advised.132 149–152 Referral to a hepatologist is also recommended for all patients, but is imperative for those with detectable HBV-DNA. Special attention should be given to patients considered as high-risk for HBV reactivation. These are mainly patients treated with rituximab; some investigators as well as rheumatology and/or hepatology societies have suggested that these patients should be referred to a hepatologist for consideration of prophylactic treatment irrespective of HBV-DNA levels.153–157 Of note, compared with people with high titres of anti-HBs antibodies, those with low titres have also been linked with greater risk of reactivation.158–163 In terms of prophylaxis, the TF did not suggest any antiviral drug in favour of the other, as this is a decision that should be made by the treating hepatologist. There are no data to support a recommendation about the timing of anti-viral treatment, but it is reasonable to start ideally before or at least simultaneously with the treatment administered for AIIRD and continuing for least 6–12 months after discontinuation of antirheumatic treatment, as has been proposed in recommendations from rheumatology and hepatology/gastroenterology societies.137 153 155 157 164 165 This proposed time window for prophylaxis continuation might be longer for patients treated with rituximab.137 153 157 165 Given the lack of data, the TF did not make a specific recommendation related to this. Instead, a relevant research agenda item has been agreed (see below).
Screening for chronic hepatitis C should be considered in patients prior to starting csDMARDs, bDMARDs, tsDMARDs, immunosuppressants and glucocorticoids (according to dose and duration). Screening is recommended for patients with elevated alanine aminotransferase or those with known risk factors
Most of the studies examining hepatitis C virus (HCV) reactivation pertain to treatment with bDMARDs, particularly TNF inhibitors, and show that HCV reactivation does occur, although in a low number of patients.166–170 Of note, most of these studies were published before newer, more effective drugs against HCV (eg, direct acting antivirals) were widely available. In the interest of public health, the TF suggests that screening should be considered in AIIRD patients before starting treatment. Considering also cost-effectiveness and geographical variations, the threshold for screening should be lower for patients with concurrent HCV risk factors (eg, intravenous use of drugs) and/or abnormal LFTs, especially ALT. No data exist regarding HCV screening and glucocorticoids or immunosuppressants. Therefore, recommendation for these drug categories is based on expert opinion. Screening for HCV includes anti-HCV antibodies and if these are present, measurement of HCV-RNA levels.164 171 172 Patients with detectable HCV-RNA should be referred for consideration of antiviral treatment. In these patients, regular monitoring with LFTs and viral load is also advised.166 170 173–175
Screening for HIV is recommended prior to treatment with bDMARDs and should be considered prior to treatment with csDMARDs, tsDMARDs, immunosuppressants and glucocorticoids (according to dose and duration)
No robust data exist for the safety of treatment with DMARDs, immunosuppressants or glucocorticoids in patients with HIV; however, the TF supported that screening for HIV should be undertaken prior to treatment with bDMARDs, with appropriate HIV care and treatment given where indicated. Taking also into account the importance of addressing public health and depending on cost-effectiveness and national guidelines, screening of HIV could be performed before commencing other antirheumatic drugs as suggested in other recommendations for specific AIIRD or drugs.176 177
All patients commencing csDMARDs, bDMARDs, tsDMARDs, immunosuppressants and/or glucocorticoids (according to dose and duration) who are non-immune to varicella zoster virus (VZV) should be informed about post-exposure prophylaxis following contact with VZV
In the TF meeting, it was discussed whether AIIRD patients should have serological screening for VZV immunity. Acknowledging that status of VZV-immunity can be affected by various factors, including national regulations, access to testing, as well as previous vaccination or infection history, it was considered appropriate not to formulate a specific recommendation on this issue; however, the TF advocates the importance of establishing VZV-immunity status through a detailed past medical history of previous exposure, for example, chickenpox. Mainly based on published expert opinion178 179 the TF agreed that those identified as non-immune or where there is doubt about their immunity status, should be informed in advance about post-exposure prophylaxis and offered prophylaxis after contact with a person with chickenpox or shingles, according to local guidelines. There is no evidence about the level of immunosuppression/immunomodulation (type of treatment) above which, patients would have a benefit from postexposure prophylaxis. This has been noted in the research agenda.
Prophylaxis with antivirals against reactivation of herpes zoster infection (shingles), as has been suggested by some in the literature (largely expert opinion),179–181 could not be recommended routinely at this stage. It has been suggested that this might benefit patients with AIIRD with a history of recurrent herpes zoster infections; however, the TF considered that there was not enough evidence to support such a recommendation at this stage.
Prophylaxis against Pneumocystis jirovecii pneumonia (PCP) should be considered in patients with AIIRD in whom high doses of glucocorticoids are used, especially in combination with immunosuppressants* and depending on the risk–benefit ratio.
Prophylaxis for PCP has been mostly examined in AIIRD patients treated with glucocorticoids. Although the minimum dose and duration of glucocorticoid treatment above which prophylaxis is recommended is not defined, evidence suggests that in daily doses >15–30 mg of prednisolone or equivalent for >2–4 weeks, prophylaxis is beneficial.182–186 Most studies do not focus on a specific AIIRD. Therefore, it was not possible to make recommendations for PCP prophylaxis in individual diseases although the risk for PCP infection might be significantly different.187 Data specifically addressing the contribution of other antirheumatic drugs in PCP development are limited.188 189 On the other hand, it has been shown that coadministration of immunosuppressants with glucocorticoids184 185 190 increase the risk for PCP. Other features including persistent lymphopenia,5 6 184 185 older age and pre-existing lung disease are also considered risk factors for PCP.4–6
The most commonly used prophylaxis scheme is trimethoprim/sulfamethoxazole (TMP-SMX) 480 mg/day (single-strength) or 960 mg three times a week; of note, there is some evidence that reduced doses (eg, half-strength, daily) may also be effective and associated with fewer adverse events .191–195 It should be noted that adverse events related to TMP-SMX (eg, nausea, headache, rash) are common, affecting about 20% of patients.196 Concerns for higher adverse event rates have been expressed for individuals treated with methotrexate (in specific relation to the combination of TMP and MTX and the risk of cytopenia) or in patients with systemic lupus erythematosus (SLE).187 197
Alternative prophylactic medications include atovaquone, dapsone or nebulised pentamidine. Although there is some disagreement in the literature,198 it seems that they are equally effective compared with TMP-SMX199–201; however, their usage is limited by factors like cost or need for hospital administration.2
Discussion
This is the first set of EULAR recommendations on the screening and prophylaxis of opportunistic and chronic infections in AIIRD. The four OAPs comprise the cornerstones of the eight recommendations produced. The latter are presented and grouped per infectious agent (rather than per underlying rheumatic disease or by individual antirheumatic treatments) as the steering group and the members of the TF concluded that this was the best way to present the evidence in the respective SLR and subsequently formulate the recommendations. They should be considered as a whole for each patient.
During the development of these recommendations, we faced several challenges, mainly pertaining to the variations across different types of AIIRD or antirheumatic drugs used. Initially, we had to decide which pathogens should be included in these recommendations. As discussed, our scoping review identified the bulk of these pathogens, and the TF members made their additions based on their expertise. Contribution of the two infectious disease doctors who participated in this TF and reviewed the list of studies regarding pathogens was crucial. We also reviewed an authoritative consensus about opportunistic infections reporting during clinical trials and post-marketing surveillance of biological therapies in immune-mediated diseases1 and found it to be consistent with the pathogens that were included in our SLR. Of note, infection with SARS-CoV2 was not included in these recommendations, as it is covered by EULAR recommendations dedicated to this topic.202
Some infections are traditionally linked with a specific drug class (eg, TB with TNF-inhibitors) which creates a risk of underestimating the importance of screening before commencing treatment with other drug categories (ie, csDMARDs and glucocorticoids in the example of TB). Stronger recommendations for specific treatments could not always be made as there is a lack of data for many of the commonly used drugs in rheumatology. This includes newer medications such as the JAK-inhibitors but also well-established immunosuppressants, such as cyclophosphamide. In these cases, level and GoR were low, and the respective unmet needs are captured in the research agenda.
To add another level of complexity, there is heterogeneity on clinical grounds about the screening and prevention strategies followed currently across different AIIRD. For example, prophylactic treatment for PCP with TMP-SMX is recommended in patients with ANCA-associated vasculitis203 but not in patients with SLE, as the evidence about the latter is limited thus far.204 As regards treatment with glucocorticoids, risk for specific infections like TB or HBV reactivation differs in relation to dose and duration of treatment. Therefore, where there was evidence available, specific doses/duration of glucocorticoids are proposed in this set of recommendations as a cut-off, in accordance with guidance from other societies.38 137
Finally, some pathogens are more prevalent in specific areas of the world, so special attention should be paid in these cases. Extensive discussions took place during the TF meetings about whether a separate recommendation should be included for rarer pathogens like Histoplasma spp, Coccidioides spp, Strongyloides spp and others which are more prevalent in specific geographical areas. As discussed in the respective SLR, relevant evidence was scarce, despite several expert opinion articles. Eighty-two per cent of the members voted that no recommendation can be formulated at this stage for these less common organisms. On the other hand, TF members agreed, as has been shown,205 that people living with AIIRD benefit when provided with general dietary and environmental advice to reduce their risk of infection from specific pathogens (eg, Listeria spp, Salmonella spp) while receiving treatment with bDMARDs, tsDMARDs, immunosuppressants and high-doses of glucocorticoids. In addition, patients commencing any antirheumatic therapies should be counselled about infection risk as part of self-management.19 Furthermore, increased awareness for atypical or rarer infections (eg, Histoplasma spp) is proposed for patients living or travelling from high-endemic areas.206 207
Considering differences between countries and consistently with other EULAR recommendations21 and EULAR SOP,7 cost-effectiveness was also taken into account in the discussions that took place during the TF meetings, although such formal assessments were not conducted. As captured in the OAPs of this set of recommendation, national regulations, where they exist, should also be considered as a guidance for screening/therapeutic decisions. OAPs were phrased to stress that decision and were made on a case-by-case basis, considering concurrent risk factors (eg, treatment with other medications, comorbidities). Importantly, screening and prophylactic procedures should be reassessed periodically. The importance of the multidisciplinary approach is also highlighted. Even though rheumatologists should always be in close collaboration and refer where appropriate to other professions, the TF underscores the central role of the rheumatologist in the management of chronic and opportunistic infections arising in the context of AIIRD and relating to the antirheumatic treatment received. For example, in HBV reactivation, rheumatologists should be able to understand the meaning of the various HBV screening tests and refer the patient on as appropriate. Our TF included clinicians from other disciplines (eg, infectious diseases, pulmonology) and although recommendations/guidelines from other non-rheumatology societies were not included specifically in our SLR, their views were taken into account.38 137 155 157
In these recommendations, despite discussing prevention strategies, we did not include or discuss studies about vaccination, as this is covered by another set of EULAR recommendations208; however, screening strategies proposed herein might identify individuals who are candidates for vaccinations.
During the TF meetings, it was discussed that the TF members, in collaboration with EULAR, will help towards the implementation of this set of recommendation in clinical practice. As outlined in the EULAR SOP,7 there are various implementation strategies, including audits and inclusion of recommendations in quality indicators. It is expected that apart from EULAR and EMEUNET, the TF members will help in the dissemination of this set of recommendations, in the first instance via their national rheumatology societies. Apart from rheumatologists and health policy makers, HPRs should be also aware of these recommendations given their active role in the education and monitoring of people living with AIIRD.209 It is also important that patient associations and people living with AIIRD, who are encouraged to play an active role in shared decision making and their care pathway, are also aware of these recommendations.19 We believe that implementation of these recommendations will lead to better outcomes for patients, as it has been shown, for example, that rates of TB were significantly decreased after screening recommendations were issued at a national level.102
For some infectious diseases (eg, fungal infections) data are still scarce. Most of these are recognised in the work presented here and in the respective SLR and are captured in the research agenda. Hopefully these issues will be the subject of future research and will be answered in time.
In summary, this is the first set of EULAR recommendations addressing the need for guidance about screening and prophylaxis in people living with AIIRD. Variations relating to treatment, geographical and other differences were taken into account. We believe that these recommendations will be a useful aid for decision making for people living in many countries and working in different healthcare systems.
Research agenda
A research agenda was considered during and after the second TF meeting. Items collected for the research agenda are shown in box 1
Research agenda
General
Does the risk of opportunistic and chronic infections differ between the different classes of disease-modifying antirheumatic drugs (DMARDs) or immunosuppressive drugs?
What is the dose and duration of glucocorticoids above which the risk of opportunistic and chronic infections starts to increase compared to those patients not receiving glucocorticoids? Does this differ by pathogen?
How often should people with autoimmune inflammatory rheumatic diseases (AIIRD) receiving antirheumatic therapies be rescreened for chronic and opportunistic infections?
Is screening and prophylaxis for opportunistic and chronic infections in people with AIIRD receiving antirheumatic therapies cost-effective?
Tuberculosis
Should patients starting immunosuppressants (eg, cyclophosphamide) be screened routinely for latent tuberculosis (TB)?
Should patients starting antirheumatic therapies be screened for non-tuberculous mycobacteria? What is the most effective way to screen for these infections?
How often should patients who have already been tested for tuberculosis, be rescreened? In relation to that, is there a need to rescreen patients who switch biological DMARDs or targeted synthetic-DMARDs?
Hepatitis
When should hepatitis antiviral treatment be started in people living with AIIRD commencing antirheumatic treatment found to be at risk of hepatitis reactivation?
For how long should hepatitis antiviral prophylaxis be continued in patients at risk for hepatitis reactivation after antirheumatic treatment is stopped?
Should patients with chronic or resolved hepatitis B also be screened for hepatitis D?
Other viruses
Is it safe to treat people living with HIV with antirheumatic treatments?
When should antiviral prophylaxis be considered in people with AIIRD who have recurrent herpes zoster infections?
Is postexposure prophylaxis for patients non-immune to VZV who are exposed to VZV beneficial?
Should patients with AIIRD starting antirheumatic therapy be screened for cytomegalovirus?
Pneumocystis jirovecii pneumonia (PCP)
Does the risk of Pneumocystis jirovecii pneumonia (PCP) differ according to underlying AIIRD (eg, giant cell arteritis, systematic literature review, ANCA-associated vasculitis, etc)?
What is the added risk of PCP in patients treated with combination glucocorticoids/immunosuppressive therapies compared to those receiving glucocorticoids along?
What is the safest and most effective regimen for PCP prophylaxis?
How long should patients at risk for PCP receive prophylaxis?
Other pathogens
Does avoidance of certain foods (eg, unpasteurised cheese) reduce the risk of opportunistic and severe infections in patients with AIIRD receiving antirheumatic treatments?
Should people with AIIRD starting antirheumatic therapies living in endemic areas be screened for Leishmania, Histoplasma or Coccidioides?
Should people with AIIRD starting antirheumatic therapies be screened for fungal infections?
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Twitter @FragoulisGeorge, @ElenaNikiUK, @DrMiniDey, @delcourvoisier, @maryanaluys
Correction notice This article has been corrected since it published Online First. The affiliations for Prof G Nagy and Prof Eva Polverino have been corrected as well as Prof Polverino's name.
Contributors All authors contributed and finally approved the current manuscript.
Funding The systematic literature review was funded as part of the EULAR Quality of Care Committee (Cl118) project for the 2022 EULAR recommendations on the screening and prophylaxis of chronic and opportunistic infections. KLH is also supported by the NIHR Manchester Biomedical Research Centre.
Competing interests GEF: Consulting fees/honoraria: Pfizer, Abbvie, Novartis, UCB, AENorasis, Janssen, Pharmaserv-Lilly. EN: speaker fees/honoraria: Celltrion, Pfizer, Sanofi, Gilead, Galapagos, AbbVie, Lilly, Fresenius. Research funding: Pfizer, Lilly. MD: none SZ: consulting fees: UCBDC: None. LA: has received consulting fees and/or research funding from Astra-Zeneca, GSK, Pfizer. FA: none. GMNB: has received consulting fees/honoraria as speaker from Gilead, ViiV Healthcare, Janssen, MSD, Roche, Moderna unrelated to this work. JWJB: none PB: none CAC: none SG-D: none MCK: none KL: has received consulting/speaker fees from Pfizer, Viatris, Celltrion outside of the submitted work. ML: none. JM: none GN: consulting fees/honoraria as speaker from AbbVie, Amgen, Boehringer Ingelheim, Janssen, Miltenyi Biotech, Lilly, Pfizer, Roche unrelated to this work. EP: consulting fees/honoraria as speaker from Bayer, Menarini, Grifols, Zambon, Pfizer, Chiesi, Teva, Shire, Shionogi, Insmed, Boehringer-Ingelheim, unrelated to this work. JvR: none MS: consulting fees: BMS, Boehringer-Ingheleim, Eli Lilly, Celltrion, Amgen, Pfizer, Janssen Cilag. AS: has received consulting fees/honoraria as speaker from AbbVie, Amgen, BMS, Celltrion, Janssen, Lilly, MSD, Pfizer, Roche unrelated to this workAdT: none JG: speaker fees/honoraria: Abbvie, Galapagos, Gilead, Janssen, Lilly, Novartis, Pfizer, UCB. Research funding: Abbvie, Astrazeneca, Galapagos, Gilead, Gritstone, Janssen, Moderna, Novovax, PfizerKH: honoraria from Abbvie; grant income from Pfizer and BMS.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.