Article Text

Abstract
Objectives Fatigue is a frequent symptom in rheumatoid arthritis (RA) and has high impact on quality of life. We explored associations between disease activity and fatigue in patients with early RA during the initial 24 months of modern treat-to-target therapy and predictors of fatigue after 24 months of follow-up.
Methods Data were obtained from the treat-to-target, tight control Aiming for Remission in Rheumatoid Arthritis: a Randomised Trial Examining the Benefit of Ultrasound in a Clinical Tight Control Regime (ARCTIC) trial. Fatigue was measured on a visual analogue scale (VAS) from 0 to 100 mm and defined as clinically relevant if VAS was ≥20 mm. Baseline predictors of fatigue at 24 months were analysed by multivariable logistic regression.
Results 205 patients with fatigue data at baseline and 24 months were included. Median (25th, 75th percentiles) symptom duration was 5.4 months (2.8, 10.4), fatigue VAS 37.0 mm (13.0, 62.0) and mean Disease Activity Score (DAS) 3.4 (SD 1.1) at baseline. Prevalence of fatigue declined from 69% at baseline to 38% at 24 months. Fewer swollen joints (OR 0.92, 95% CI 0.87 to 0.98, p=0.006), lower power Doppler ultrasound score (OR 0.95, 95% CI 0.90 to 0.99, p=0.027) and higher patient global assessment (PGA) (OR 1.03, 95% CI 1.01 to 1.04, p<0.001) increased the risk of clinically relevant fatigue at 24 months. Not achieving remission at 6 months was associated with a higher risk of reporting fatigue at 24 months.
Conclusions Fatigue in patients with early RA was prevalent at disease onset, with a rapid and sustained reduction during treatment. Low objective disease activity and high PGA at baseline were predictors of clinically relevant fatigue at 24 months.
- arthritis
- rheumatoid
- ultrasonography
- patient-reported outcome measures
- inflammation
Data availability statement
Data are available upon reasonable request. The authors commit to making the relevant anonymised patient level data available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Fatigue is common in patients with rheumatoid arthritis (RA). Knowledge about the causes of fatigue is limited, and associations between fatigue and disease activity are uncertain.
What does this study add?
This study shows that there is an association between disease activity and fatigue, and that achieving early disease remission decreases the risk of fatigue. Baseline predictors of fatigue at 24 months are lower number of swollen joints, lower ultrasound power Doppler score and higher patient global assessment.
How might this impact on clinical practice or future developments?
These results support the effect of early treat-to-target treatment on fatigue in a majority of patients with early RA and provide baseline predictors of fatigue at 24 months. A non-pharmacological approach to fatigue might be favourable in the presence of these predictors.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory disease characterised by joint inflammation with subsequent joint destruction and loss of function.1 Up to 70% of patients with RA experience fatigue,2 and patients have ranked fatigue as one of the most important disease-related outcomes in RA.3 4 There is no generally accepted definition of RA-related fatigue, but the symptoms have been described ‘as an overwhelming, debilitating, and sustained sense of exhaustion that decreases the ability to function and carry out daily activities’.5
Fatigue is considered a multidimensional phenomenon involving disease processes, personal and social aspects,2 and with implications for the patient’s quality of life as well as increased societal costs related to reduced work productivity and frequent physician consultations.6 Physical function, age, gender, mental health, pain, sleep disturbances and inflammation have been found to be associated with fatigue. However, none of these variables show a consistently strong relationship with fatigue across studies in systematic reviews, and the impact of inflammatory disease activity on fatigue has not been established.6–9
The goal in modern RA treatment is sustained remission and augmentation of long-term health-related quality of life through control of symptoms, prevention of structural damage, and participation in social and work-related activities.10 11 In addition to the introduction of biological disease-modifying antirheumatic drugs (DMARDs), more aggressive treatment with higher doses of methotrexate, earlier initiation of DMARDs and tight control strategies have led to a large proportion of patients with early RA reaching sustained remission.11 However, fatigue in patients with early RA treated according to modern treatment strategies is still not well understood.
The objectives of this study were, first, to explore the longitudinal prevalence of fatigue in patients with early RA followed up in a treat-to-target strategy trial and to investigate the relationship between fatigue and disease activity. Second, we aimed to identify baseline predictors of unresolved fatigue after 24 months of follow-up and, finally, to assess the impact of early treatment response and remission on fatigue.
Materials and methods
Study design
Data were obtained from the Aiming for Remission in Rheumatoid Arthritis: a Randomised Trial Examining the Benefit of Ultrasound in a Clinical Tight Control Regime (ARCTIC) trial.12 Participants were randomised 1:1 to a treat-to-target strategy with or without applying musculoskeletal ultrasonography in clinical examinations and treatment decisions. All patients were treated according to a predefined algorithm that started with a combination of methotrexate (15 mg/week escalated to 20–25 mg/week) and prednisolone (15 mg tapered to 0 mg) during the initial 7 weeks. The treatment target was remission defined as Disease Activity Score (DAS) in 44 joints of <1.6 and no swollen joints, with an additional target of no power Doppler signal in any examined joint in the ultrasound arm. Each patient was scheduled for 13 visits during the 2-year follow-up.12
Participants
Patients (18–75 years) who fulfilled the American College of Rheumatology (ACR)/European Alliance of Associations for Rheumatology (EULAR) classification criteria for RA13 were recruited from 11 Norwegian rheumatology centres between 2010 and 2013. All patients provided written consent, and all had symptom duration of less than 24 months, no prior DMARD use and indication for DMARD treatment at inclusion.12
Participant involvement
Two participants recruited from the ARCTIC trial were involved in the planning and interpretation of the analyses presented in this article.
Fatigue
Fatigue was measured at all visits on a Visual Analogue Scale (VAS) ranging from 0 mm (fatigue is not a problem) to 100 mm (fatigue is a major problem).14–16 The question was articulated, ‘Have you had problems with fatigue during the last week’? Fatigue is recommended as a core outcome measure in clinical trials by the Outcome Measures in Rheumatology, ACR and the EULAR.17 18
As there are no standardised cut-offs for clinically relevant fatigue, we dichotomised fatigue in accordance with previous studies: <20 mm (no fatigue) and ≥20 mm (clinically relevant fatigue).19–21 For the predictor analyses, the outcome was fatigue of ≥20 mm at 24 months. Additionally, we divided the fatigue VAS in <20, 20–39 and ≥40 mm corresponding to low or no fatigue, clinically relevant fatigue and high level of fatigue, respectively.22–24 Fatigue was also assessed on a continuous scale. The percentage of participants who achieved a minimal clinically important improvement in fatigue VAS of ≥10 mm was assessed at 24 months.25
Clinical assessments
Disease activity was measured at all visits by DAS (range 0–10),26 which incorporates assessment of tender joints (Ritchie Articular Index range 0–78), number of swollen joints (0–44), the patient global assessment (PGA) of disease activity on a VAS (VAS 0–100 mm) and erythrocyte sedimentation rate (ESR, mm/hour). DAS of <1.6 corresponds to remission; DAS of <2.4 corresponds to low disease activity; DAS of >2.4–3.7 corresponds to moderate disease activity; and DAS of >3.7 corresponds to high disease activity27. In addition, the Boolean-based ACR/EULAR remission,28 Simplified Disease Activity Index remission29 and Clinical Disease Activity Index remission30 were assessed. Treatment response was evaluated by EULAR good/moderate response.31
The clinical evaluation also included C reactive protein (CRP, mg/L) and ultrasound examination of 32 joints at baseline and yearly in all patients (0–3 semiquantitative scoring of grey scale and power Doppler using an atlas for reference).32 33
Patient-reported outcomes and demographic measures
Sleep difficulty was assessed by a component of the Rheumatoid Arthritis Impact of Disease (RAID) on a Numerical Rating Scale (range 0–10, higher scores representing poorer outcome). Mental health was assessed by the 36-Item Short Form Survey Mental Component Summary Score consisting of the components mental health, vitality, role–emotional and social functioning (range 0–100, with lower scores indicating poorer outcome).34 Physical function was assessed by Patient-Reported Outcome Information System (PROMIS) on a range of 20–100, translated to a T score with a mean of 50 and an SD of 10, where lower scores implied poorer outcome.35 Patient-reported outcomes were acquired electronically at 0, 3, 6, 12, 16 and 24 months during study visits.12 In addition, PGA was measured at all 13 visits. Baseline characteristics included age, gender, anti-CCP positivity, rheumatoid factor, body mass index (BMI) of ≥25 kg/m2 and a comorbidity score measured by the Self-administered Comorbidity Questionnaire (score 0–45).36 Education was dichotomised below/above 12 years.
Statistics
Data from the two study groups in ARCTIC were pooled for the current analyses as there were no statistically significant differences in primary or secondary endpoints between the two study groups.12 Patients with complete fatigue data at baseline and 24 months were included. Missing fatigue data as well as other continuous variables between baseline and 24 months were imputed with last observation carried forward. Categorical variables missing at 24 months were imputed with worst outcome, and missing data before 24 months with last observation carried forward.12 Continuous variables are described in means (SD), or medians (25th, 75th percentiles) as appropriate. Categorical variables are presented as frequencies (%).
We explored changes in median fatigue from baseline to 24 months and calculated the proportions of patients in the three fatigue categories at baseline and at 6 and 24 months. The correspondence between changes in fatigue VAS and changes in DAS according to categories was assessed.
Potential baseline predictors of fatigue of ≥20 mm at 24 months of follow-up were explored by univariable logistic regression, and a p value of less than 0.10 was required for the variable to be included in the subsequent multivariable analysis. Continuous variables were tested for linearity. A multivariable prediction model was built using backward stepwise selection requiring a p value of <0.05 to keep the covariate in the model. All models were adjusted for age and gender. Variables excluded from the final model were re-entered one by one and kept in the model if they changed the coefficient of any other variable by more than 20%. Potential interactions between variables in the final model were analysed by including interaction terms one by one. Joint pain VAS, PROMIS physical function and RAID sleep were excluded from analyses due to high correlation with PGA (r=0.83, r=−0.67 and r=0.58, p<0.001, respectively) at baseline, but separate analyses of a model including these variables were also performed. DAS was not included as a composite measure, but the components were included separately. As CRP and ESR are closely related, we included CRP in the analyses in favour of ESR. ORs were calculated to explore the associations between early treatment response or remission and fatigue after 24 months of treatment. Robustness analyses were performed using only complete case data, and sensitivity analyses were performed for patients with fatigue of ≥20 mm at all time points from baseline to 24 months.
All analyses were performed using Stata/IC V.14.0 and 16.0.
Results
Baseline characteristics
Of the 230 patients analysed for the primary outcome in the ARCTIC trial, 205 had complete fatigue data at baseline and 24 months and were included in the current analyses. There were no statistically significant differences in baseline variables between the subset of 205 and the full set of 230 patients. Less than 5/205 (2.4%) of the observations for any variables were imputed at any time point during the 24 months of follow-up. Baseline demographics and disease characteristics are presented in table 1. Fatigue was highly prevalent at baseline with 142/205 (69%) reporting fatigue of ≥20 mm, and median fatigue was 37.0 mm (25th, 75th percentiles 13.0, 62.0). Mean DAS of 3.4 (SD 1.1) corresponded to moderate disease activity level at baseline.
Baseline demographics and disease characteristics
Changes in fatigue from baseline to 24 months
There was a rapid and sustained reduction in fatigue with the largest reduction observed within the first 3 months (figure 1 and online supplemental figure 1). Median fatigue was 37 mm (25th, 75th percentiles 13.0, 62.0) at baseline and 9 mm (25th, 75th percentiles 2.0, 34.0) at 24 months, and mean fatigue was 39 mm (SD 27.9) and 21 mm (SD 24.5) at baseline and 24 months, respectively.
Supplemental material

Change in median fatigue VAS (0–100 mm) over 24 months. Percentiles (25th and 75th) illustrated by the shaded area. VAS, Visual Analogue Scale.
At baseline, 142/205 (69%) reported a fatigue score of ≥20 mm, compared with 77/205 (38%) at 24 months (p<0.001) (figure 2). A total of 57% of the patients had a minimal clinically important improvement in fatigue (≥10 mm) at 24 months, and the proportion of patients reaching minimal clinically important improvement according to baseline fatigue of <20, 20–40 and >40 mm were 11%, 64% and 84%, respectively, displaying that a majority of patients with moderate and high fatigue achieved an improvement corresponding to minimal clinically important improvement.

{kind=link}
{kind=link}
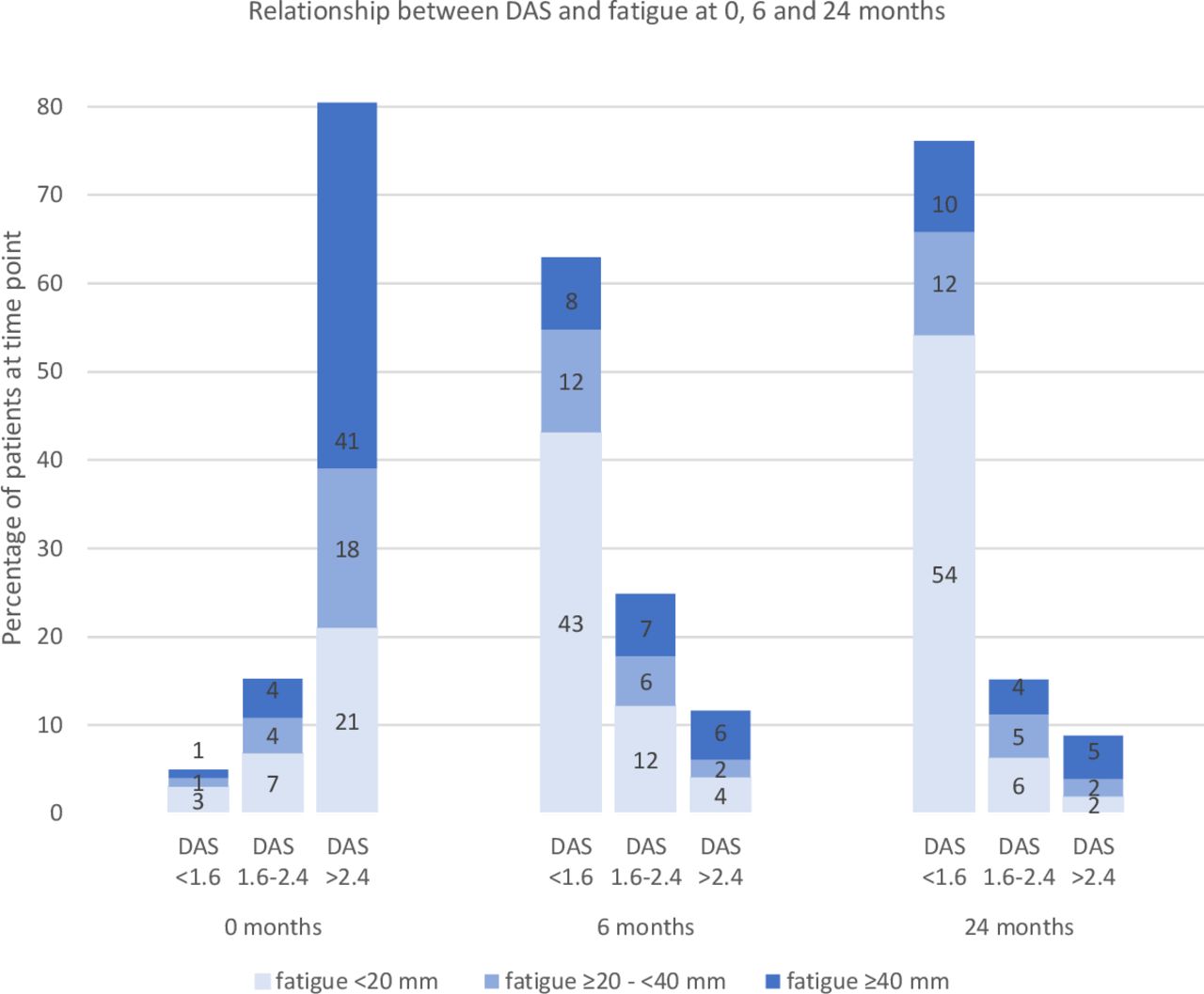
Percentage of patients in fatigue categories <20, ≥20–<40 and ≥40 mm according to DAS categories <1.6, 1.6–2.4 and >2.4 at 0, 6 and 24 months. DAS, Disease Activity Score.
Changes in fatigue and disease activity
There was a parallel reduction in fatigue and disease activity as 80% of the patients had moderate or high disease activity according to DAS (>2.4) at baseline and 9% at 24 months, while 69% of patients reported clinically relevant fatigue (≥20 mm) at baseline and 38% at 24 months (figure 2). At baseline, 95/205 (46%) had a fatigue score of 40 mm or higher, and this proportion was reduced to 39/205 (19%) at 24 months (figure 2). There was a corresponding increase in patients with low or no fatigue from baseline to 24 months; 63/205 (31%) of the patients scored <20 mm on the fatigue scale at baseline, compared with 128/205 (62%) at 24 months. In concurrence, 10/205 (5%) were in DAS remission at baseline vs 156/205 (76%) at 24 months (figure 2).
The proportion of patients with fatigue was highest among the patients with moderate to high disease activity both at baseline with 122/165 (74%) and 24 months with 14/18 (78%).
A fraction of the patients in DAS remission reported fatigue: 4/10 (40%) at baseline and 45/156 (29%) at 24 months, while some patients with moderate or high DAS (>2.4) did not report fatigue: 43/165 (26%) at baseline and 4/18 (22%) at 24 months (figure 2).
Baseline predictors of fatigue
Sleep disturbances, Mental Component Summary Score, physical function and PGA at baseline were predictors of fatigue at 24 months, in addition to low number of swollen joints and low ultrasound power Doppler score (table 2). In the multivariable analyses, number of swollen joints (OR=0.92, 95% CI 0.87 to 0.98, p value of 0.006), ultrasound power Doppler score (OR=0.95, 95% CI 0.90 to 0.99, p value of 0.027) and PGA (OR per mm=1.03, 95% CI 1.01 to 1.04, p<0.001) were significant predictors of reporting fatigue at 24 months, when controlling for the other factors in the model, as described in table 2.
Baseline predictors of clinically relevant fatigue (≥20 mm) at 24 months
Similar results were observed in robustness analyses in complete case data and sensitivity analyses for patients with sustained, clinically relevant fatigue from baseline to 24 months (data not shown).
Moreover, neither BMI, depression as a comorbidity (online supplemental table 1), methotrexate dosage (online supplemental table 2) nor the extent of adverse events (online supplemental table 3) were associated with fatigue in our data.
Associations between fatigue and early treatment response or remission at 6 months
There was no significantly decreased risk of reporting fatigue of ≥20 mm at 24 months for patients who achieved EULAR good/moderate response at 3 months (OR=0.62, 95% CI 0.28, 1.34, p value of 0.277) (table 3). However, there was a significantly decreased risk of reporting fatigue of ≥20 mm at 24 months for patients who achieved remission at 6 months by all listed remission criteria (table 3).
ORs of fatigue ≥20 mm at 24 months according to EULAR response at 3 months, DAS remission, ACR/EULAR Boolean remission, SDAI remission and CDAI remission at 6 months
Discussion
In this inception cohort of patients with early RA, clinically relevant fatigue of ≥20 mm was highly prevalent at treatment onset. There was an overall rapid and sustained reduction in fatigue corresponding to the reduction in disease activity, and the majority of patients were in remission or low disease activity with no clinically relevant fatigue at 24 months. Prediction analyses demonstrated that few swollen joints, low power Doppler ultrasound score and high PGA at baseline increased the risk of reporting fatigue at 24 months. In addition, not reaching remission at 6 months increased the risk of reporting fatigue at 24 months.
Differences in fatigue measures, cut-offs and study designs create some challenges in the comparison of fatigue across studies. We saw a lower baseline level of fatigue in the present analyses than in comparable studies by Rat et al,20 Scott et al37 and Gossec et al,38 where patients with early RA reported mean fatigue level of 47.8 (SD 28.2) and mean fatigue of >50 and >60 mm, respectively. Furthermore, the reduction in fatigue during the 24 months of follow-up was greater in the ARCTIC cohort than in a longitudinal register study by Druce et al,21 where mean fatigue VAS was above 50 mm at baseline and at 1 and 4 years of follow-up, and smaller reductions in fatigue were observed in studies on patients with early RA as well as in patients with established RA.19 23 24 Mean fatigue at 24 months in the ARCTIC cohort was similar to the level of fatigue (mean 20.5 mm (SD 0.02)) in Norwegian healthy controls reported by Slatkowsky-Christensen et al, supporting that the overall level of fatigue in the ARCTIC cohort at 24 months was at the same level as a normal population.39 In agreement with previous research, our findings suggest that fatigue is prevalent in patients with early RA in about two of three patients, and that the prevalence is similar to what has been observed in established RA.19 20 24 40
We found that the improvement in fatigue over time corresponded to the reduction in disease activity, indicating a treatment response. There was a higher proportion of patients with high fatigue among patients with the highest disease activity at all assessed time points, which implies a positive relationship between the two factors. At the same time, our analyses showed that some patients in DAS remission reported fatigue and that some patients with high disease activity experienced low or no fatigue. Proinflammatory cytokines involved in the inflammatory responses in RA have been suggested to trigger fatigue,6 41 42 and some trials have indicated an association between disease activity and fatigue.24 43–45 However, other studies show that in some cases, fatigue persists even though inflammation and disease activity are low.22 46 47
The predictor analyses support that fatigue is a multidimensional phenomenon.2 The multivariable analyses indicated that low inflammatory disease activity represented by few swollen joints and low ultrasound power Doppler score, and high scores of PGA at baseline were associated with a higher risk of fatigue at 24 months of follow-up. It could seem contradictory that we observed a positive association between fatigue and disease activity as well as between early remission and unresolved fatigue at 24 months, and at the same time found little inflammation at baseline to predict fatigue at 24 months. One explanation could be that there were two subsets of fatigue: patients where high inflammatory disease activity was the cause of fatigue and for whom early, intensive treatment improved fatigue, and patients with fatigue at baseline for whom fatigue could have been triggered by different factors that were not affected by DMARD treatment.23 48 These factors might be captured by PGA, and further research is warranted on the relationship between fatigue and PGA. In the 38% of the patients who reported clinically relevant fatigue at 24 months, the source of fatigue might not have been adequately addressed. Associations between comorbidities such as depression and fibromyalgia and fatigue have been documented in prior studies8 49 but were not confirmed in our data. Non-pharmacological interventions to relieve fatigue are tailored physical activity, behavioural modification, treatment of pain or depression, and improving sleep.8
Our results indicate that achievement of treatment target at 6 months reduced the risk of fatigue at 24 months, and similar results were observed by Scott et al, who found that fatigue was significantly lower in patients with RA in an intensive treat-to-target strategy compared with patients who received standard treatment.24 37
This study has limitations. There is a lack of standardised fatigue measures and definitions in RA, and we used global, unidimensional fatigue VAS in the present analyses. Fatigue VAS does not yield detailed information; however, fatigue VAS is validated as more sensitive to change than some multidimensional measures and has high reliability, construct, content and face validity.14–16 50 Furthermore, it is one of the most frequently applied measures of fatigue in RA.16 The lack of standardised cut-offs for fatigue VAS generates uncertainties regarding the prevalence and severity of fatigue, including the extent of residual fatigue, and complicates comparison of results across studies.
A strength of this study is the longitudinal, prospective and multivariable analyses which have been recommended.7 In addition, data from the ARCTIC trial provided a unique opportunity to explore fatigue in patients with early RA followed by modern treat-to-target strategies, and to our knowledge, this is the first study that have explored associations in patients with early RA between fatigue and ultrasound, biochemical and clinical assessments, in addition to a comprehensive assessment of patient-reported outcome measures.
In conclusion, this study showed that the majority of patients with early RA treated according to current EULAR treatment recommendations experienced a rapid and sustained reduction of fatigue. However, patients who did not reach remission at 6 months were at risk of experiencing fatigue at the 2-year follow-up, which could be of importance to clinicians in identifying patients at risk of long-term fatigue. In addition, there was a higher risk of fatigue in patients with RA with low objective disease activity measures and high patient reported global assessment of disease at baseline, and a non-pharmacological approach to fatigue in these patients might be considered.
Data availability statement
Data are available upon reasonable request. The authors commit to making the relevant anonymised patient level data available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The Aiming for Remission in Rheumatoid Arthritis: a Randomised Trial Examining the Benefit of Ultrasound in a Clinical Tight Control Regime trial was approved by an independent ethics committee (the Regional Committee for Medical and Health Research Ethics South-East; reference number 2010/744) and appropriate institutional review boards, and followed the guidelines outlined in 'Guidelines for Good Clinical Practice' developed by the International Conference of Harmonization.
Acknowledgments
The authors thank the patients for participating in this study and the Aiming for Remission in Rheumatoid Arthritis: a Randomised Trial Examining the Benefit of Ultrasound in a Clinical Tight Control Regime and investigators: Hallvard Fremstad, Tor Magne Madland, Åse Stavland Lexberg, Hilde Haukeland, Erik Rødevand, Christian Høili, Hilde Stray, Anne Lindter Noraas, Dag Magnar Soldal and Gunnstein Bakland.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
EAH and A-BA are joint senior authors.
Handling editor Josef S Smolen
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content, approved the final manuscript to be submitted and agreed to be accountable for all aspects of the work. Conception and design of the study: KH, NPS, SL, EAH and A-BA. Acquisition of data: NPS, HBH, EM, TU, EAH and A-BA. Analysis and interpretation of data: KH, NPS, SL, JS, LBN, EM, HBH, TU, TKK, EAH and A-BA.
Funding This work was supported by the DAM Foundation, research grants committee. The Aiming for Remission in Rheumatoid Arthritis: a Randomised Trial Examining the Benefit of Ultrasound in a Clinical Tight Control Regime study has received grants from the Norwegian Research Council, Norwegian South-Eastern Health Region, the Norwegian Rheumatism Association and investigator-initiated research grants from AbbVie, Union Chimique Belge Pharma, Pfizer Inc, Merck Sharp & Dohme Norway and Roche Norway. The funders of the study had no role in study design, data collection, data analysis, data interpretation or writing the report.
Competing interests All authors have completed the International Committee of Medical Journal Editors uniform disclosure form at www.icmje.org/disclosure-of-interest/ (available on request from the corresponding author). KH, JS, NPS, SL and LBN declare no conflict of interest. EM received personal fees as leader for the national rheumatology nurses in the Norwegian Nurses Organisation. HBH received personal honoraria from Abbvie, Lilly, Pfizer and Novartis, and participated in a data safety monitoring board or advisory board for Novartis and Lilly. TU received consultancy honorarium from Lilly and Pfizer. TKK received consultancy honorariums from AbbVie, Amgen, Biogen, Celltrion, Eli Lilly, Gilead, Mylan, Novartis, Pfizer, Sandoz, Sanofi, Egis, Evapharma, Ewopharma, Hikma and Oktal. EAH received consulting fees from Abbvie, Novartis, Pfizer, Gilead, Eli Lilly, Galapagos and Janssen. A-BA received consultancy honorariums from AbbVie, Eli Lilly, Novartis, Pfizer and UCB.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.