Article Text

Abstract
Objective To compare event and incidence rates of herpes zoster (HZ), also known as shingles, in patients with rheumatoid arthritis under treatment with conventional synthetic (cs), targeted synthetic (ts) or biologic (b) disease-modifying antirheumatic drugs (DMARDs).
Methods Patients were prospectively enrolled from 2007 until October 2020. Reported HZ events were assigned to ongoing treatments or those terminated within 1 month prior to the HZ event. Exposure-adjusted event rates (EAERs) of HZ were calculated per 1000 patient years (py) and adjusted HRs with 95% CIs computed. Inverse probability weights (IPW) were used to adjust for confounding by indication.
Results Data of 13 991 patients (62 958 py) were analysed, with 559 HZ events reported in 533 patients. The EAER of HZ was highest for tsDMARDs (21.5, 95% CI 16.4 to 27.9), followed by B cell targeted therapy (10.3, 95% CI 8.0 to 13.0), monoclonal antitumour necrosis factor (anti-TNF) antibodies (9.3, 95% CI 7.7 to 11.2), interleukin 6 inhibitors (8.8, 95% CI 6.9 to 11.0), soluble TNF receptor fusion protein (8.6, 95% CI 6.8 to 10.8), T cell costimulation modulator (8.4, 95% CI 5.9 to 11.8) and csDMARDs (7.1, 95% CI 6.0 to 8.3). Adjusted for age, sex and glucocorticoids and weighted with IPW, tsDMARDs (HR 3.66, 95% CI 2.38 to 5.63), monoclonal anti-TNF antibodies (HR 1.63, 95% CI 1.17 to 2.28) and B cell targeted therapy (HR 1.57, 95% CI 1.03 to 2.40) showed a significantly higher risk compared with csDMARDs.
Conclusion Our results provide evidence for a 3.6-fold increased risk of HZ associated with tsDMARDs and an increased risk of HZ under bDMARDs compared with csDMARDs.
- arthritis
- rheumatoid
- biological therapy
- tumour necrosis factor inhibitors
- DMARDs
Data availability statement
No data are available. RABBIT data are not approved to be shared.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Patients with rheumatoid arthritis have an increased risk of developing herpes zoster (HZ).
Increased incidence rates have been reported under tumour necrosis factor and Janus kinase (JAK) inhibitors.
What does this study add?
Comparative data on all disease-modifying antirheumatic drugs (DMARDs) provide evidence for an increased risk of HZ under JAK inhibitors.
Treatment with biologic DMARDs showed a significantly higher risk compared with conventional synthetic DMARDs.
Higher age and glucocorticoids were also associated with an increased risk of HZ.
How might this impact on clinical practice or future developments?
An increased risk of HZ should be considered especially under JAK inhibitors, in elderly patients, and under glucocorticoid therapy.
Introduction
Herpes zoster (HZ), also known as shingles, remains a clinically relevant infectious event for patients with rheumatoid arthritis (RA). In addition to the generally increased risk with RA and older age,1 2 current research focuses on the question to what extent the specific disease-modifying antirheumatic drug (DMARD) treatment of RA influences the risk of HZ. A comparison of all available biologic (b) DMARDs, including tumour necrosis factor (TNF) inhibitors, abatacept, rituximab and tocilizumab, in the US Medicare data of 2015 showed a similar risk of HZ across all biologic agents.3 The newer targeted synthetic (ts) DMARDs, the Janus kinase (JAK) inhibitors, however, reportedly have an at least twofold risk of HZ, which was further increased by the addition of glucocorticoids.4–7 Another meta-analysis using pooled data of 40 eligible randomised clinical trials and 19 observational studies until 2016 indicated an increased risk of HZ in immunocompromised patients receiving bDMARDs, especially of non-TNF blocking agents, mainly because studies comparing TNF inhibitors with controls were under-represented.8 No European data on the risk of HZ under JAK inhibitors in real-world settings have been available to date.9 The European Alliance of Associations for Rheumatology recommends considering HZ vaccination in high-risk patients with autoimmune rheumatic disease.10 Data to date show that only a small percentage of patients have been vaccinated against HZ so far.3 11
To further investigate the risk of HZ when exposed to different antirheumatic therapies, we compared event and incidence rates of HZ in patients with RA under treatment with conventional synthetic (cs) DMARDs, tsDMARDs or bDMARDs and evaluated in addition the contribution of concomitant glucocorticoid therapy.
Patients and methods
Data source
The German Rheumatoid Arthritis: Observation of biologic therapy register RABBIT is a prospective longitudinally followed cohort of patients with RA that are included with a new start of a bDMARD/tsDMARD, or with a csDMARD treatment after at least one prior DMARD therapy. At the time of enrolment, at months 3 and 6, and then every 6 months during the time of observation, information is collected from rheumatologists and patients on demographics, clinical status including joint counts, treatment details (eg, start/stop dates of DMARDs, dosages of glucocorticoids), laboratory tests, patient-reported outcomes and adverse events. Rheumatologists are requested to classify reported events according to the International Conference on Harmonisation E2A guideline on serious and non-serious events and to provide additional information on serious adverse events, for example, providing hospital discharge letters if available. Patients are observed for up to 10 years, irrespective of treatment changes. For this analysis, patients enrolled from 2007 onwards with at least one follow-up were included.
Outcome and treatment exposure
All HZ events reported until 31 October 2020 were selected. Medical Dictionary for Regulatory Activities Terminology (MedDRA) terms used in this study included ‘herpes zoster’ (MedDRA code 10019974), ‘herpes zoster infection neurological’ (MedDRA code 10061208), ‘herpes ophthalmic’ (MedDRA code 10062004), ‘herpes zoster oticus’ (MedDRA code 10063491), ‘herpes zoster disseminated’ (MedDRA code 10065038), ‘herpes zoster meningitis’ (MedDRA code 10074259) and ‘herpes zoster cutaneous disseminated’ (MedDRA code 10074297).
Treatment with DMARDs was categorised into monoclonal anti-TNF antibodies (adalimumab, certolizumab, golimumab, infliximab), soluble TNF receptor fusion protein (etanercept), T cell costimulation modulator (abatacept), B cell targeted therapy (rituximab), interleukin (IL) 6 inhibitors (tocilizumab, sarilumab), JAK inhibitors (tofacitinib, baricitinib, upadacitinib) and csDMARDs as the reference group. Patients were considered receiving bDMARD/tsDMARD treatment at the time of an event if the respective treatment was ongoing or terminated within 1 month prior to the event. In a sensitivity analysis, this 1-month risk window was extended to 3 months.
Age, sex, disease duration, disease activity assessed by the Disease Activity Score of 28 joints (DAS28) using erythrocyte sedimentation rate and the Clinical Disease Activity Index (CDAI), physical capacity assessed by the Hannover Functional Status Questionnaire (FFbH, 0–100, with 100 representing full capacity), presence of rheumatoid factor and anticitrullinated protein antibodies (ACPA), level of C reactive protein (CRP), number of previous DMARDs, glucocorticoid therapy and doses, comorbidities (osteoporosis, hypertension, coronary heart disease, diabetes, chronic obstructive respiratory disease, chronic kidney disease, malignant neoplasia, lymphoma/leukaemia, mental illness/depression), and number of comorbidities (recorded by the rheumatologist as present or not) were used to characterise patients at baseline.
Statistical analysis
Differences at baseline between treatment groups were examined using descriptive statistics (mean, SD, median, IQR and percentage). Exposure-adjusted event rates of HZ (EAERs; defined as the number of HZ events divided by the total exposure time among patients in the respective treatment group) and exposure-adjusted incidence rates (EAIRs; defined as the number of HZ events divided by the total exposure time among patients in the respective treatment group and at risk of an initial occurrence of HZ) with 95% CIs were calculated per 1000 patient years (py).
The Andersen-Gill model, an extension of the standard Cox proportional hazard model used to include recurrent events by taking the complete follow-up time into account, was applied and adjusted HRs with 95% CIs were calculated to investigate risk factors for the development of HZ. Patient characteristics at baseline (age, sex) and characteristics varying with time during follow-up (treatment with bDMARDs/tsDMARDs and treatment with glucocorticoids) were considered as possible risk factors. The CIs of the HRs were calculated by means of robust sandwich estimates. Adjustment with inverse probability weights (IPW) was used to deal with confounding by indication. These weights were estimated by means of logistic regression with the covariates age, sex, disease duration, disease activity (DAS28), functional status (FFbH), previous treatment with bDMARDs/tsDMARDs and osteoporosis (yes/no). In a sensitivity analysis, IPW was calculated using CDAI instead of DAS28 as a measure of disease activity. Osteoporosis was used as an indirect indicator of long-standing disease activity in RA.
A secondary analysis was performed in a subsample of patients to evaluate the potential impact of unmeasured confounding. This subsample included only those patients who were (1) either enrolled with a certain bDMARD/tsDMARD treatment, had at least one interruption of this bDMARD/tsDMARD treatment during follow-up, and received only csDMARD treatment during this interruption time; or (2) patients who were enrolled with a csDMARD treatment and started a bDMARD/tsDMARD treatment during follow-up. Each patient in the subsample serves as her/his own control, observed under treatment exposure with a certain bDMARD/tsDMARD, but as well exposed to csDMARD alone, while carrying her/his own risk factors.
Missing values on DAS28 (CDAI) at the start of treatment were imputed by fitting regression models. Strongly skewed distributions, like the CRP, were logarithmised to prevent undesired effects and reverse-transformed for the calculation of regression coefficients.
Data analyses were performed with SAS V.9.4, and p values <0.05 were considered statistically significant.
Results
Patient characteristics at baseline
A total of 13 991 patients (62 958 py of observation) were included. At baseline (ie, the time at enrolment in RABBIT with a new start of a DMARD therapy), 3242 patients started treatment with monoclonal anti-TNF antibodies, 2513 with soluble TNF receptor fusion protein, 817 with T cell costimulation modulator, 1431 with B cell targeted therapy, 1424 with IL-6 inhibitors, 713 with JAK inhibitors and 3851 with csDMARDs after at least one prior csDMARD therapy.
The mean age of all patients was 57.7 years, whereby patients receiving monoclonal anti-TNF antibodies were younger (55.1 years) and those receiving JAK inhibitors were older (59.5 years) than patients in the other treatment groups. Patients under B cell targeted therapy were most often RF or ACPA positive (84% and 76%, respectively) and received most often glucocorticoid therapies (68%) compared with all other treatment groups. (The latter may be influenced by use of glucocorticoids as premedication of B cell targeted therapies to reduce possible infusion-related symptoms.) Meanwhile, patients under T cell costimulation modulator received most often concomitant methotrexate (68%). Patients in these two treatment groups tended to have the longest disease duration (12 and 10 years, respectively), the lowest functional capacity (FFbH score 56 and 59, respectively), the highest disease activity (DAS28 5.3 and 5.2, respectively), more often had osteoporosis (28% and 25%, respectively), and the highest number of previous therapies with csDMARDs (2.7 and 2.5, respectively) and bDMARDs/tsDMARDs (1.7 and 1.3, respectively). The presence of comorbidities other than osteoporosis was comparable between the treatment groups (table 1). All baseline characteristics are reported in table 1.
Patient characteristics at baseline (N=13 991)
EAER of HZ
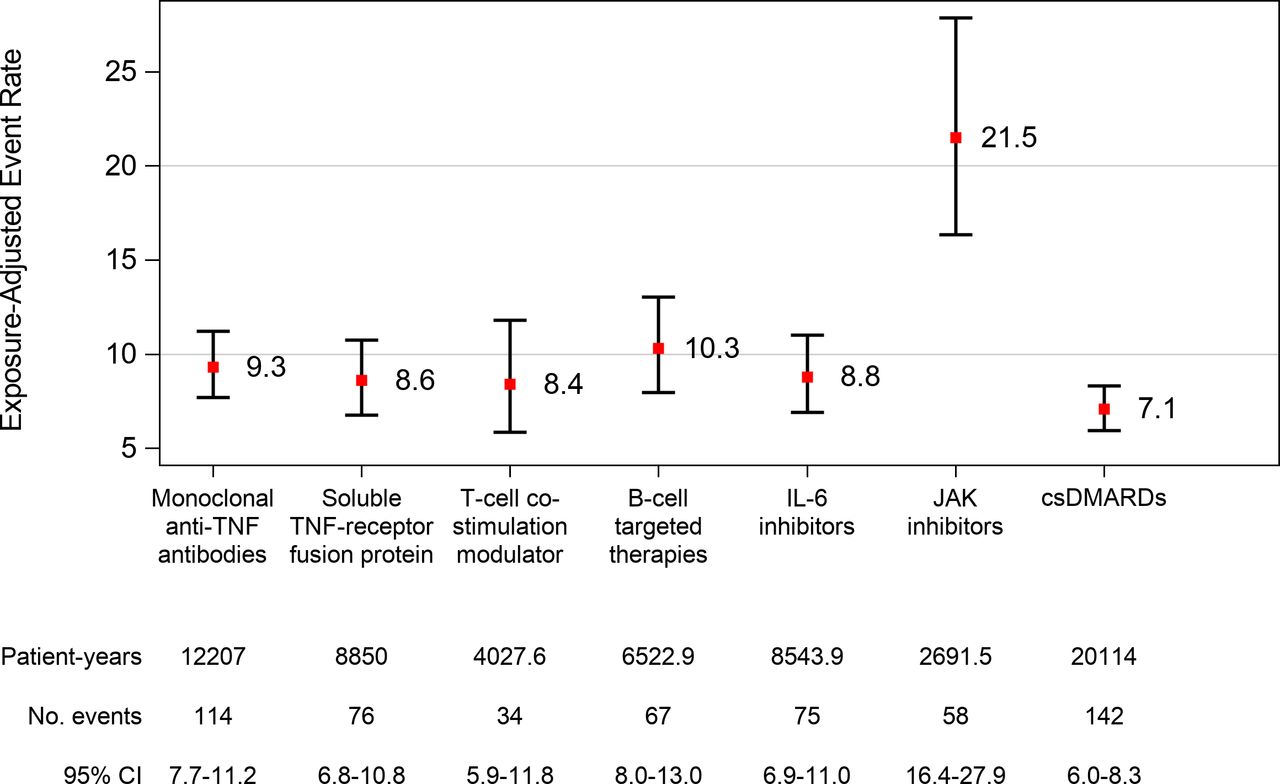
A total of 559 HZ cases in 533 patients were reported. The event rate per 1000 py was 8.9 (95% CI 8.2 to 9.6) over all treatments. The EAER of HZ was 9.3 (95% CI 7.7 to 11.2) for monoclonal anti-TNF antibodies, 8.6 (95% CI 6.8 to 10.7) for soluble TNF receptor fusion protein, 8.4 (95% CI 5.9 to 11.8) for T cell costimulation modulator, 10.3 (95% CI 8.0 to 13.0) for B cell targeted therapy, 8.8 (95% CI 6.9 to 11.0) for IL-6 inhibitors, 21.5 (95% CI 16.4 to 27.9) for JAK inhibitors and 7.1 (95% CI 6.0 to 8.3) for csDMARDs (figure 1). The event rate of HZ under JAK inhibitors with concomitant use of glucocorticoids was comparable with the event rate of HZ under JAK inhibitors without concomitant use of glucocorticoids (online supplemental figure S1). The EAER per 1000 py for each separate MedDRA term is presented in online supplemental table S1. Similar EAERs were observed when using a 3-month risk window (data not shown).
Supplemental material

Exposure-adjusted event rates of all herpes zoster per 1000 patient years. csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; IL-6, interleukin 6; JAK, Janus kinase; TNF, tumour necrosis factor.
A total of 61 serious HZ events were reported in 61 patients. The event rate of serious HZ over all treatments per 1000 py was 1.0 (95% CI 0.7 to 1.2). The event rates between treatments did not differ considerably, except for higher event rates of serious HZ under B cell targeted therapy and JAK inhibitors (figure 2). The EAIRs of all HZ and of serious HZ are comparable with the respective EAERs and are provided in online supplemental figures S2 and S3, respectively.

{kind=link}
{kind=link}
Exposure-adjusted event rates of serious herpes zoster per 1000 patient years. csDMARDs, conventional synthetic disease-modifying antirheumatic drugs; IL-6, interleukin 6; JAK, Janus kinase; TNF, tumour necrosis factor.
Recurrent HZ events occurred in 22 patients. Patient characteristics at baseline and EAERs of HZ among patients with recurrent events are provided in online supplemental tables S2 and S3, respectively.
Risk of HZ
Adjusted for age, sex and glucocorticoid use, a significantly increased risk was observed for treatment with monoclonal anti-TNF antibodies (HR 1.73, 95% CI 1.34 to 2.24), soluble TNF receptor fusion protein (HR 1.45, 95% CI 1.09 to 1.94), B cell targeted therapy (HR 1.62, 95% CI 1.21 to 2.18), IL-6 inhibitors (HR 1.41, 95% CI 1.06 to 1.89) and JAK inhibitors (HR 3.23, 95% CI 2.32 to 4.48) compared with treatment with csDMARDs. Treatment with T cell costimulation modulator showed no significantly higher risk compared with csDMARDs. Furthermore, older age, female sex and glucocorticoid use in a dose-dependent manner were associated with an increased risk of HZ (table 2). Using IPW adjustment, a significantly higher risk of HZ remained under monoclonal anti-TNF antibodies, B cell targeted therapy and JAK inhibitors compared with treatment with csDMARDs (table 2). A sensitivity analysis, where IPW was estimated including CDAI instead of DAS28 as a measure of disease activity, showed similar results, except for B cell targeted therapy being no longer significant in comparison with csDMARDs (online supplemental table S4).
Risk of herpes zoster: Andersen-Gill model with and without IPW
Subsample analysis of patients with different treatment episodes
A total of 5974 patients were observed under treatment with a certain bDMARD/tsDMARD and with csDMARD alone, and thus included in the subsample analysis (a schematic representation of the design of the subsample is provided in online supplemental figure S4). These patients’ first three treatment switches or (transient) interruptions are illustrated in online supplemental figure S5. It shows, for instance, that among the patients who started treatment with monoclonal anti-TNF antibodies at baseline, the majority experienced only (transient) interruption before receiving another bDMARD/tsDMARD, while ‘treatment switch’ in patients enrolled with csDMARDs mainly meant that they started TNF inhibitor treatment.
The mean duration of treatment with bDMARDs/tsDMARDs and csDMARDs is reported in table 3, together with the baseline characteristics of patients in the subsample, which were comparable with those in the entire study sample. A patient from this subsample who started treatment with monoclonal anti-TNF antibodies at baseline was treated, on average, for 12.9 months with this treatment and for 10.1 months with csDMARDs alone, whereas a patient who started treatment with JAK inhibitors at baseline was treated, on average, for 7.3 months with this treatment and for 6.7 months with csDMARDs alone (table 3).
Characteristics of patients who were either enrolled with bDMARD/tsDMARD treatment and had interruption(s) during follow-up in the course of which they received csDMARDs alone or who were enrolled with csDMARD treatment and started bDMARD/tsDMARD treatment during follow-up (n=5974)
Adjusted for age, sex and glucocorticoid use, a significantly increased risk in this subsample analysis was observed for treatment with monoclonal anti-TNF antibodies (HR 1.87, 95% CI 1.31 to 2.69), B cell targeted therapy (HR 1.71, 95% CI 1.22 to 2.39) and JAK inhibitors (HR 3.51, 95% CI 2.24 to 5.52) compared with treatment with csDMARDs, whereas treatment with soluble TNF receptor fusion protein, T cell costimulation modulator and IL-6 inhibitors showed no significantly higher risk compared with csDMARDs (table 4). Furthermore, older age, female sex and glucocorticoid use were associated with an increased risk of HZ (table 4).
Risk of herpes zoster for patients who were either enrolled with bDMARD/tsDMARD treatment and had interruption(s) during follow-up in the course of which they received csDMARDs alone or who were enrolled with csDMARD treatment and started bDMARD/tsDMARD treatment during follow-up
Discussion
This is the first analysis in a European prospective cohort study comparing the event and incidence rates and risk of HZ in patients with RA under treatment with six different DMARDs of variable modes of action with csDMARD treatment in one large national cohort. A significant association between HZ and treatment with tsDMARDs was found. The association between HZ and monoclonal anti-TNF antibodies as well as B cell targeted therapy was less influential and varied depending on the methodology used. A significantly higher risk of HZ was found for patients of older age and for treatment with glucocorticoids, with the latter being dose-dependent.
Previous data from the USA showed an increased risk of HZ in patients treated with tsDMARDs, but no clear association was found between HZ and use of bDMARDs.2 Earlier data from the RABBIT register have already shown an increased risk of patients treated with a monoclonal anti-TNF antibody.12 However, it remained unclear whether this was due to inflammatory activity of RA or due to the specific mode of action of the treatment administered, as patients treated with soluble TNF receptor fusion protein did not show an increased risk. In contrast, data from the British Society for Rheumatology Biologics Register provided evidence for an increased risk associated with all TNF inhibitors, while in other reports no increased incidence rates were found.13–15 Furthermore, differences in the use of concomitant glucocorticoids and methotrexate were discussed as possible causes of these different results because, uniformly in all studies, glucocorticoids were associated with an increased risk of HZ. In a meta-analysis of 2014, a 61% significantly increased risk of HZ was calculated for patients receiving TNF inhibitors.16
The results of the analysis presented here comparing data on all DMARDs support our former findings of an increased incidence of HZ under bDMARDs compared with csDMARDs. Of note, this analysis was based on an independent data set with data collected between 2007 and end of October 2020, while the former analysis was performed on a data set of the same cohort with earlier data collected between 2001 and end of December 2006.12 In agreement with our previous report, we showed a higher risk of HZ in patients receiving monoclonal anti-TNF antibodies but not in those receiving the soluble TNF receptor fusion protein. This difference may be explained by different mechanisms of action related to the induced cytotoxicity in TNF-expressing monocytes and T cells, yielding the expression of different leucocyte genes.17 18 Due to the approval of additional therapies since the previous analysis, this time we were also able to investigate the risk of HZ for other mechanisms of action. This enabled us to investigate the risk of HZ also under B cell targeted therapy, T cell costimulation modulator, IL-6 inhibitors and tsDMARDs, of which the first and the latter were significantly associated with an increased risk of HZ compared with csDMARDs.
The possible mechanism leading to reactivation of the virus may differ with regard to the specific mechanisms of action. While monoclonal anti-TNF antibodies conjoin transmembrane TNF and induce apoptosis of T cells, the soluble TNF receptor does not. Etanercept lacks a specific domain for the docking of one of the complement components so that interaction proceeds differently.19 From the reactivation of latent tuberculosis it is known that insufficient interferon-gamma (IFN-γ) production may also play a role, as TNF inhibitors but not B cell targeted therapy, T cell costimulation modulator and IL-6 inhibitors inhibit the IFN-γ production induced by tuberculosis antigens.19 JAK inhibitors modulate the immune response by blocking intracellular signals on the cytokine level. The downregulation of interleukin 12, IFN-γ and other relevant cytokines is discussed to enable the reactivation of latent viral infections.20 21 A possible explanation for the specific attenuated immune response to tofacitinib may be found in a recent basic science work when keratinocytes and synovial cells were exposed to tofacitinib and the immune response was measured after stimulation with bacterial lipopolysaccharides or viral varicella-zoster virus (VZV).22 The results confirm what we also see in our data, namely that antiviral immunity is downregulated after exposure to JAK inhibitors.
The more unstable influence of the other bDMARDs remains to be further investigated. EAERs and EAIRs were very comparable and adjusted HRs were significant for all modes of actions except for abatacept. The numbers were not very dissimilar for this drug particularly with IPW. After IPW adjustment, only monoclonal TNF and B cell depletion remained significant, but in the sensitivity analysis B cell depletion was no longer significant. A clear difference in terms of the underlying mechanisms of action cannot be derived from this.
Age and glucocorticoids have previously been described as risk factors for HZ4–6 and were confirmed in our data. The clear dose dependence with a 3.5-fold higher risk at doses above 10 mg should be emphasised here.
Although only 11% of the HZ events reported in our cohort were considered as being serious by the local investigator, the impact of HZ on patients’ burden of disease and on healthcare in general is considerable.23 Healthcare utilisation and costs are about doubled in patients with RA and HZ compared with persons with HZ without immunosuppression.24
In terms of a risk assessment with regard to vaccination, this suggests that especially elderly patients with higher glucocorticoid doses and patients for whom tsDMARD therapy is planned should be considered for vaccination. Preliminary data from tofacitinib-treated patients with RA indicate the possibility of reducing the risk of HZ by vaccination.4
Limitations and strengths
The query of the vaccination status has only recently been added to the questionnaire used in the RABBIT register and could not be taken into account in this analysis. Since we do not know the proportion of patients who may have been vaccinated, there is a possibility of unequal distribution in the groups. Future analyses, however, will allow adjusting for vaccination status. Concomitant methotrexate was not adjusted for as its use differs among the bDMARDs included in this analysis. Moreover, a clear association between HZ events and use of methotrexate in patients with RA has not been confirmed.25
The strength of our study is the large prospective register that includes all available DMARD therapies in RA, enabling direct risk comparison of different treatments within one cohort. Furthermore, we conducted a secondary analysis among a subsample of patients who were either enrolled with a certain bDMARD/tsDMARD treatment, had at least one interruption of this treatment during follow-up, and received csDMARD treatment during this interruption period or patients who were enrolled with csDMARD treatment and started a bDMARD/tsDMARD treatment during follow-up. The strength of this analysis was that each patient had been observed under different treatment episodes (bDMARD/tsDMARD vs csDMARD alone), while carrying her/his own risk factors. Thus, patients serve as their own controls in this design. The results of this secondary analysis support the findings of the main analysis.
To conclude, the risk of HZ infection in patients with RA is multiplied by age and the need for immunosuppressive therapy especially when glucocorticoids and JAK inhibitors are applied.
Data availability statement
No data are available. RABBIT data are not approved to be shared.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by the ethics committee of the Charité University Medicine Berlin.
Acknowledgments
The authors acknowledge the invaluable contributions of all participating consultant rheumatologists and their patients. In particular, the authors would like to thank the rheumatologists who enrolled the highest numbers of patients: J Kaufmann, T Klopsch, C Eisterhues, J Braun, I Schwarze, A Liebhaber, A Krause, K Rockwitz, S Zinke, C Kneitz, C Möbius, E Ständer, H Tony, S Berger, A Gräßler, C Kühne, S Remstedt, W Ochs, E Wilden, M Bohl-Bühler, S Wassenberg, H Kellner, G Burmester, F Haas, C Richter, M Röser, A Bruckner, S Balzer, H Fricke-Wagner, H Bergerhausen, W Harmuth, G Wiesmüller, S Lebender, A Bussmann, F Hamann, C Stille, M Feuchtenberger, E Edelmann, H Tremel, B Krummel-Lorenz, H Körber, K Krüger, L Meier, A Kapelle, L Müller, A Thiele, M Schmitt-Haendle, U Prothmann, D Pick, K Karberg, H Brandt, K Weiß, J Kekow, A Seifert, U Müller-Ladner, K Manger, C Baumann, D Krause, M Aringer, M Worsch, A Roßbach, M Zänker, H Streibl, M Backhaus, C Richter, H Schulze-Koops, C Herzberg, M Grünke, N Heel, P Herzer, N Heel, A Reck, F Wiesent, G Dahmen, N Blank, R Max, T Eidner, R Dockhorn, G Zeh, K Winkler, H Menne, U von Hinüber, W Demary, H Sörensen, M Schneider, A Gause, A Bruns, C Bielecke, T Marycz, B Häckel, K Alliger, H Euler, A Gause, F Moosig, C Iking-Konert, J Häntsch, R Boldemann. The authors also acknowledge the significant contributions of Peter Herzer, Munich, Bernhard Manger, Erlangen, and Matthias Schneider, Düsseldorf, as members of the advisory board.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Contributors IR, MS and AS had full access to all data of this study and take responsibility for data integrity and accuracy of the analysis. Study concept and design: IR, MS, AZ and AS. Acquisition of data: JK, G-RRB and JB. Analysis and interpretation of data: IR, KA, MS, AZ and AS. Drafting the manuscript: IR, KA and AS. Critical revision of the manuscript for important intellectual content: IR, MS, KA, G-RRB, JB, JK, AZ and AS. Obtaining funding: AZ and AS. All authors read and approved the manuscript.
Funding RABBIT is supported by a joint, unconditional grant from AbbVie, Amgen, BMS, Celltrion, Fresenius Kabi, Hexal, Lilly, MSD, Viatris, Pfizer, Roche, Samsung Bioepis, Sanofi-Aventis and UCB.
Competing interests AS has received speaking fees from Bristol-Myers Squibb, Celltrion, MSD, Pfizer and Roche. AZ has received speaking fees from AbbVie, Janssen, Pfizer, Roche and Sanofi-Aventis. G-RRB has received honoraria for lectures and consulting from AbbVie, BMS, Galapagos, Lilly, MSD, Pfizer, Roche and Sanofi. JB has received honoraria for talks, advisory boards, paid consultancies and grants for studies from AbbVie (Abbott), Amgen, Baxter, Biogen, BMS, Boehringer, Celgene, Celltrion, Centocor, Chugai, Fresenius, GlaxoSmithKline, Gilead, Hexal, Janssen, Lilly, Medac, MSD (Schering-Plough), Mylan, Mundipharma, Novartis, Pfizer (Wyeth, Hospira), Roche, Sanofi-Aventis and UCB.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.