Article Text

Abstract
Objective To estimate the incidence of psoriatic arthritis (PsA) in patients with psoriasis who had received a continuous treatment with biological disease-modifying antirheumatic drugs (bDMARDs) compared with phototherapy.
Methods A retrospective non-randomised study involving patients with moderate-to-severe plaque psoriasis, who were prescribed at least 5 years of bDMARDs or at least three narrow-band ultraviolet light B (nb-UVB) phototherapy courses, and did not have a diagnosis of PsA at enrolment. Development of PsA in each patient was assessed by a rheumatologist according to the Classification for Psoriatic Arthritis criteria. The annual and cumulative incidence rate of PsA was estimated by using an event per person-years analysis. Cox proportional hazards models were undertaken to assess the hazard risk (HR) of PsA after adjustment for confounders.
Results A total of 464 psoriatic patients (bDMARDs, n=234 and nb-UVB, n=230) were followed between January 2012 and September 2020 (corresponding to 1584 and 1478 person year of follow-up for the two groups, respectively). The annual incidence rate of PsA was 1.20 cases (95% CI 0.77 to 1.89) versus 2.17 cases (95% CI 1.53 to 3.06) per 100 patients/year in the bDMARDs versus phototherapy group, respectively (HR 0.29, 0.12–0.70; p=0.006). The variables independently associated with higher risk of PsA were older age (adjusted HR 1.04, 1.02–1.07), nail psoriasis (adjusted HR 3.15, 1.63–6.06) and psoriasis duration >10 years (adjusted HR 2.02, 1.09–3.76); notably, bDMARDs treatment was associated with a lower risk of incident PsA (adjusted HR 0.27, 0.11–0.66).
Conclusions bDMARDs treatment may delay or reduce the risk of incident PsA in patients with moderate-to-severe chronic plaque psoriasis.
- arthritis
- psoriatic
- biological therapy
- tumor necrosis factor inhibitors
- arthritis
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. These are deidentified participant dataAll the data are available at paolo.gisondi@univr.it. There is no embrago for the data.
Statistics from Altmetric.com
Key messages
What is already know about this subject?
In most cases, diagnosis of plaque psoriasis may precede that of psoriatic arthritis (PsA) by an average of 5–10 years, and in only a minority of cases PsA precedes the skin disease or occurs simultaneously.
The transition from psoriasis to PsA may evolve across various phases, that is, preclinical, subclinical and prodromal phases.
What does this study add?
The major finding of this non-randomised intervention study was that the incidence of PsA was lower in patients treated with biological disease antirheumatic modifying drugs (bDMARDs) compared with narrow-band ultraviolet light B phototherapy.
How might this impact on clinical practice or future developments?
Early therapeutic intervention with bDMARDs may delay or reduce the risk of PsA development in patients with moderate-to-severe chronic plaque psoriasis.
Introduction
Chronic plaque psoriasis is associated with psoriatic arthritis (PsA) in up to nearly 20%–25% of adult cases.1 Epidemiological studies have reported that the diagnosis of psoriasis may often precede the development of PsA by several years.2 In particular, psoriatic skin lesions can emerge before the development of musculoskeletal manifestations in around 75% of patients with PsA in a time frame of about 10 years.2 3 Major unmet needs in the field of PsA include improving our understanding of the natural history of disease, defining those patients with psoriasis are at increased risk of developing arthritis and characterising the immune, environmental and molecular subclinical events that precedes PsA onset. Factors that may confer an increased risk of PsA include the genetic background, the psoriatic involvement of selected body areas (such as the scalp, nails and intergluteal areas), as well as obesity and psoriasis severity, whereas no protective factors have been identified so far.4–6 The delay between the onset of skin manifestations of psoriasis and joint disease may provide a therapeutic window of clinical opportunity for preventing the progression from psoriasis to PsA. Whether a continuous systemic treatment with biological disease-modifying antirheumatic drugs (bDMARDs) in patients with psoriasis could prevent the development of PsA has not been yet extensively investigated. Thus, the main aim of this non-randomised intervention study was to estimate the incidence of PsA in patients with moderate-to-severe chronic plaque psoriasis, who had received a continuous treatment with bDMARDs compared with those treated with narrow-band ultraviolet light B (nb-UVB) UVB phototherapy.
Methods
We have undertaken a retrospective non-randomised intervention study, involving psoriatic patients consecutively attending the Dermatology outpatient service of the University Hospital of Verona between 1 January 2012 and 30 September 2020, who were receiving either bDMARDs or nb-UVB phototherapy for the treatment of moderate-to-severe chronic plaque psoriasis.
We initially identified in our electronic database a total of 982 potentially eligible psoriatic patients. Among these, we selected patients, who met the following inclusion criteria: (1) age >18 years; (2) a clinically confirmed diagnosis of moderate-to-severe chronic plaque psoriasis; (3) a continuous treatment with a bDMARD for at least 5 years (between 2012 and 2020); patients with treatment interruptions up to 3 months between two consecutive courses were also included. In the case of a switch to another bDMARD of the same or different classes, the patient was still included in the analysis if the treatment interruption was less than 3 months; and (4) a treatment for at least three courses of nb-UVB phototherapy (each course consisting of 24–32 sessions at a frequency of 2–3 sessions/week) among those psoriatic patients, who did not receive any other synthetic agents or bDMARDs for treatment of pasoriasis (ie, these patients formed the control group).
Exclusion criteria were as follows: (1) patients with a diagnosis of PsA in the past or at the time of the inclusion in the study (n=234); (2) those who did not have a continuous treatment with a bDMARD for at least 5 years (n=187); (3) those who did not receive at least three courses of nb-UVB phototherapy (n=69); or (4) those with mild psoriasis, those using a combination therapies (eg, methotrexate associated with tumour necrosis factor alpha (TNF-α) inhibitors, or nb-UVB plus bDMARDs) (n=28). bDMARDs used in this study were TNF-α inhibitors (ie, etanercept, infliximab, adalimumab), the IL-12/23 inhibitor (ustekinumab) or the IL-17A inhibitor (secukinumab). More details about the selection procedure of the study are summarised in online supplemental figure 1, and online supplemental file 1.
Supplemental material
Supplemental material
At baseline, the presence of PsA was excluded in all included patients by a rheumatologist. All patients were initially screened for PsA by administering them the Early ARthritis for Psoriatic patients (EARP)-10 questionnaire.7 This questionnaire was routinely administered to all psoriatic patients who attended our dermatology outpatient service with a frequency of once every 6 months for our internal standard procedure. In the case of a positivity to three or more items of this questionnaire, the patient was sent to rheumatologist for a specialist visit. A rapid referral to the rheumatologist is guaranteed by the fact that we set up the joint dermatological and rheumatological clinics about 10 years ago. Each patient was classified as having PsA if he/she fulfilled the Classification Criteria for Psoriatic Arthritis criteria.8 The number of swollen and tender joints and the subset of PsA (ie, peripheral arthritis, axial involvement, enthesitis or dactylitis) were recorded. Demographics variables, smoking status, family history of PsA in the first degree relative, metabolic comorbidities (ie, obesity, diabetes, hypertension and dyslipidaemia), psoriasis duration and severity (by using the Psoriasis Area and Severity Index (PASI)), as well as involvement of nail, scalp, folds (ie, inguinal, anal, axillary or submammary) were collected in all patients at baseline. In particular, patients were diagnosed with obesity in the case of a body mass index (BMI) ≥30 kg/m2; diabetes in the case of fasting plasma glucose ≥126 mg/dL (≥7.0 mmol/L), or prior history of disease, or use of any antidiabetic medications; arterial hypertension in the case of systolic/diastolic blood pressure ≥130/85 mm Hg, or prior history of disease, or use of any antihypertensive agents; dyslipidaemia in the case of serum triglycerides ≥150 mg/dL (≥1.7 mmol/L), or total cholesterol ≥200 mg/dL (≥5.2 mmol/L), or low-density lipoprotein cholesterol ≥100 mg/dL (≥2.6 mmol/L), or use of any lipid-lowering drugs. The local ethics committee approved the study protocol. The ethics committee exempted such kind of research from the informed consent requirement because we only accessed retrospectively a deidentified database for the purpose of data analysis.
Statistical analysis
The results of continuous and categorical variables are presented as means±SD and proportions, respectively. The Pearson’s χ2 test for categorical variables and the unpaired Student’ t test for continuous variables were used to analyse the baseline differences between the groups of psoriatic patients. The number of person years at risk was calculated as the time between the date of enrolment and the last contact date. This period was used to estimate the annual incidence rate of PsA per 100 patients in the two treatment groups. The cumulative incidence of PsA over time was estimated by Kaplan-Meier method. The log-rank test was used to compare the cumulative incidence curves in the two treatment groups. The mean exposure time to phototherapy was calculated and included in the analysis. Cox proportional hazards models were used to analyse the predictors of incident PsA. Explanatory variables included smoking history, family history of PsA, metabolic comorbidities (ie, obesity, diabetes, hypertension and dyslipidaemia), psoriasis duration and severity (ie, PASI), as well as involvement of nail, scalp, folds at baseline. The effects of these included risk factors on risk of incident PsA were expressed in terms of HRs along with their 95% CI. First, an age-adjusted and sex-adjusted Cox regression model was constructed from univariate analyses and then following a directed acyclic graph only those variables presenting p<0.15 and/or biologically plausible were included in two progressive multivariable regression models (see adjusted model 1 and adjusted model 2 of table 1). A propensity score matching (PSM) procedure was also performed in all patients by fitting a logistic regression model in which the baseline PASI was used as the matching variable and the treatment received (bDMARDs or phototherapy) was the dependent variable. In logistic regression analysis, baseline PASI was included as a continuous variable. After fitting the logistic regression model, the logit transformation of PSM for all patients was stored for subsequent use in matched groups. By the PSM procedure, patients treated with bDMARDs were matched with those treated with phototherapy using a 1:1 nearest neighbour algorithm without replacement and a calliper width of 0.50 SD of the logit transform of the propensity score. The analysis was conducted using the STATA software (V.13 StataCorp, Collage Station, Texas, USA).
Multivariate Cox regression model assessing associations with psoriatic arthritis (PsA)
Results
In this retrospective, non-randomised intervention study, we enrolled a total of 464 psoriatic patients treated with either bDMARDs (n=234) or nb-UVB phototherapy (n=230), who were followed for a mean of 6.76±1.37 years per person follow-up. In the bDMARDs group, 39 (17%) patients were treated with infliximab, 17 (7%) with etanercept, 67 (29%) with adalimumab, 50 (21%) with ustekinumab and 61 (26%) with secukinumab, respectively. A total of 35 (15%) out of 234 patients on bDMARDs switched therapy. In particular, 10 patients switched from a TNF-α inhibitor to another, 8 patients from a TNF-α to IL-12/23 inhibitor and 12 patients to an IL-17A inhibitor. Five patients switched from IL-12/23 inhibitor to IL-17A inhibitor. In the nb-UVB phototherapy group, 120 (52%) patients had received three courses of phototherapy, 98 (43%) received four courses and 12 (5%) received five courses (with a mean exposure time to phototherapy of 53 weeks). The bDMARDs and phototherapy groups had a total of 1584 and 1478 person year of follow-up with a mean 6.91±1.06 and 6.60±1.62 years per person follow-up, respectively. Descriptive characteristics of the study population are reported in table 2. At baseline, patients who developed incident PsA were older, and more likely to have longer psoriasis duration, greater family history of PsA and higher psoriasis localisation at the level of scalp and nails compared with patients who did not developed PsA over the follow-up. No significant differences were found in BMI, smoking status, psoriasis localisation at folds, as well as prevalence of diabetes, dyslipidaemia or hypertension between the two patient groups.
Descriptive characteristics at baseline of participants who develop psoriatic arthritis (PsA) or not at the end of the follow-up
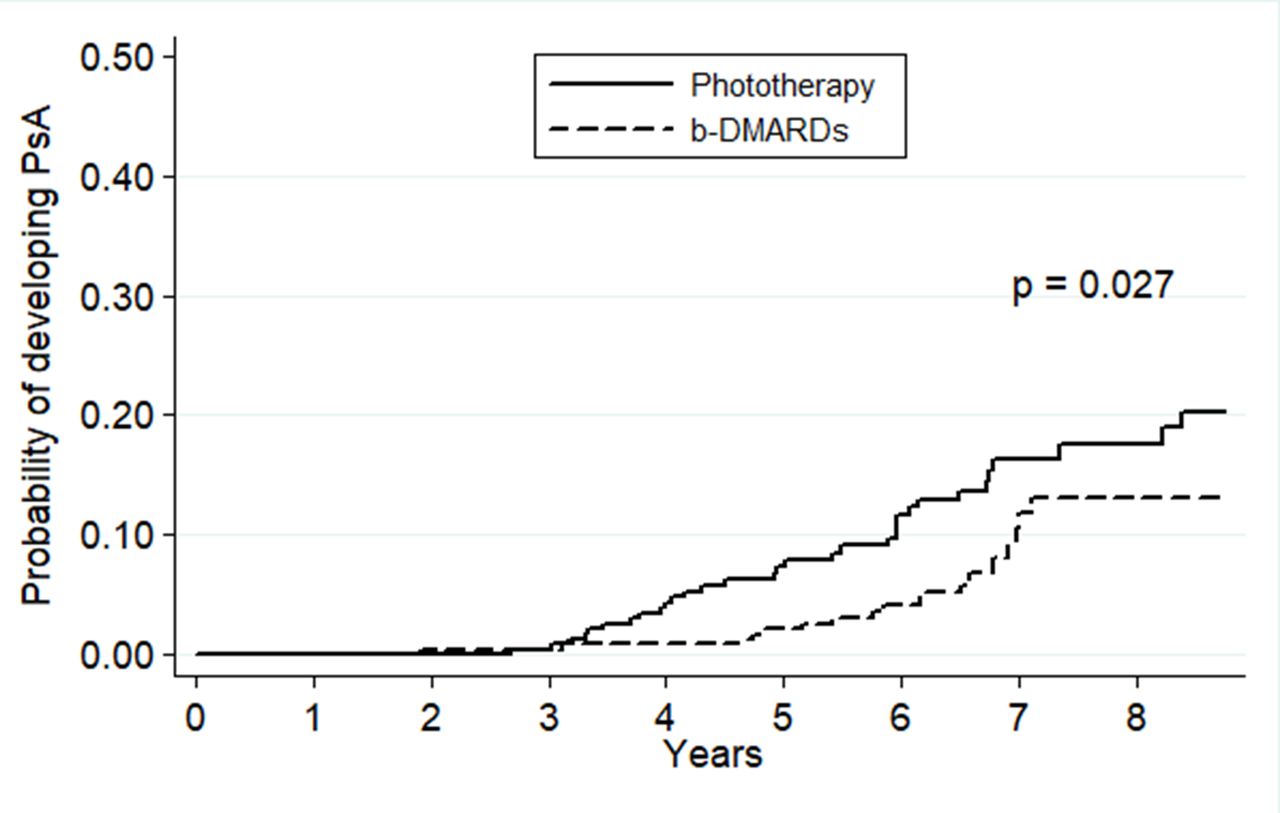
Over the follow-up, a total of 51 (11% of total) patients developed incident PsA, including 19 (8%) and 32 (14%) in the bDMARDs and nb-UVB phototherapy groups (p=0.046), respectively. In particular, the annual incidence rate of PsA was 1.20 cases (95% CI 0.77 to 1.89) versus 2.17 cases (95% CI 1.53 to 3.06) per 100 patients/year in the bDMARDs and phototherapy groups, respectively (p=0.006). The cumulative incidence curves of incident PsA in the two patient groups are shown in figure 1 (p=0.027 by log-rank test as assessed by the Kaplan-Meir survival method). The most frequent pattern of PsA was peripheral arthritis (84%), followed by dactylitis (20%), enthesitis (16%) and axial involvement (6%). More than one pattern could be observed in a single psoriatic patient. A significantly higher proportion of peripheral arthritis (p=0.003) and dactylitis (p<0.001) was observed in the phototherapy group of patients (table 3).
{kind=link}
Cumulative incidence rates of psoriatic arthritis (PsA) in the biological disease-modifying antirheumatic drugs (bDMARDs) versus narrow-band ultraviolet light B phototherapy groups, estimated by the Kaplan-Meier method (p=0.027 by the log-rank test).
Psoriatic arthritis (PsA) subsets in the two treatment patient groups
The univariable Cox regression analyses (table 1) showed that the baseline variables that were significantly associated with a higher risk of incident PsA were older age (HR 1.04, 95% CI 1.02 to 1.07), presence of nail psoriasis (HR 1.74, 95% CI 1.00 to 3.03), scalp psoriasis (HR 2.10, 95% CI 1.07 to 4.10;), family history of PsA (HR 2.30, 95% CI 1.04 to 5.12), psoriasis duration >10 years (HR 2.67 95% CI 1.48 to 4.83) and baseline PASI≥10 (HR 0.47, 95% CI 0.27 to 0.82). Notably, in univariable regression analysis, treatment with bDMARDs was significantly associated with a lower risk of incident PsA (HR 0.53, 95% CI 0.30 to 0.94) compared with nb-UVB phototherapy. The aforementioned significant variables were included in two progressive multivariable Cox regression models, as shown in table 1. Treatment with bDMARDs remained significantly associated with a lower risk of incident PsA after adjustment for age, sex, nail psoriasis and baseline PASI ≥10 (adjusted model 1), and even after additional adjustment for presence of folds psoriasis, scalp psoriasis, family history of psoriasis and psoriasis duration >10 years (adjusted model 2). Other variables that were independently associated with a higher risk of incident PsA were older age and psoriasis duration >10 years, but not baseline PASI.
Finally, given the non-randomised intervention design of the study, we also performed a PSM procedure for baseline PASI. After this statistical procedure, a total of 172 patients were identified for the analysis (n=86 in each treatment group), as shown in online supplemental table 1). After this PSM procedure, compared with nb-UVB phototherapy, treatment with bDMARDs did not show any significant association with the risk of incident PsA both in univariable regression analysis and even after adjustment for age and sex (online supplemental table 2).
Supplemental material
Discussion
The major finding of our retrospective, non-randomised intervention study was that the incidence of PsA was significantly lower in patients with moderate-to-severe chronic plaque psoriasis treated with bDMARDs compared with those treated with nb-UVB phototherapy.
It is known that the diagnosis of plaque psoriasis often precedes the development of PsA by an average of nearly 5–10 years, and in only a minority of cases PsA precedes the skin disease or occurs simultaneously.9 Genetic predisposition may dictate a different development time of the two disorders, or skin inflammation may foster the development of joint disease in genetically predisposed patients. Experimentally, it has been shown that specific epidermal alterations, such as the abrogation of JunB/activator protein 1, which is a well-known regulator of cytokine production and keratinocyte proliferation, may be sufficient to initiate both skin lesions and arthritis in mouse models of psoriasis.10 Possibly, a persistent and greater skin inflammation related to psoriasis may favour the development of PsA at both close and distant sites.11 Psoriasis and PsA share several immuno-inflammatory pathways, with a key role of TNF-α, IL-17 and IL-23 in both conditions. Different murine models of arthritis, enthesitis or psoriasiform skin lesions have documented that IL-23 administration leads to enthesis-centred inflammatory arthritis, with bone erosion and new bone formation that are mostly mediated by levels of IL-17 and TNF-α.12 The transition from psoriasis to PsA may evolve across various different phases, including preclinical, subclinical and prodromal phases.13 14 We have previously reported, and then confirmed by others, that lower limb enthesopathy is a common ultrasonographic finding among patients with psoriasis without clinical signs of arthropathy.15–19 Ultrasonographic enthesopathy may predict PsA development and it is likely related to a subclinical entheseal psoriatic inflammation.20
In the present study, we reasoned that bDMARDs targeting TNF-α or the IL-23/IL-17 axis could attenuate, delay or prevent the transition from psoriasis to PsA. In contrast, nb-UVB phototherapy dampers only skin inflammation, and it is regarded as a specific skin targeted therapy. Moreover, we admit that there is a difference in the exposure time between patients treated with either bDMARDs or phototherapy, because the latter is commonly used in intermittent courses and not continuously as bDMARDs.21 In both patient groups, there may have been some subclinical cases of incident PsA who evolved into the clinical phase more frequently in the phototherapy group than in the bDMARDs group, because these treatments are different in their mechanisms of action. Accordingly, the interception in very early PsA study showed that IL-17A inhibition led to a decline in subclinical joint inflammation, arthralgia, and skin lesions in patients with subclinical PsA.22 Conversely, oral retinoids targeting mainly keratinocytes differentiation and hyperproliferation have been associated with increased risk of PsA.23
In the present study, we found that in addition to the use of bDMARs, which had a protective effect on risk of PsA, other independent predictors of PsA development were older age, psoriasis duration >10 years and psoriasis localisation at nails. Different predictors of PsA have been identified in literature among patients with psoriasis, including genetic and environmental factors, metabolic comorbidities and psoriasis localisation.13 Genome-wide association studies and studies of human leucocyte antigen (HLA) alleles have reported that PsA has a strong genetic component.24 25 Frequencies of HLAB*08, HLAB*27, HLAB*38 and HLAB*39 alleles are higher in patients with PsA than in general population and polymorphisms of interleukin 23 receptor (IL23R) and tumour necrosis factor alpha-induced protein-3 (TNFAIP3) genes are more strongly associated with PsA than psoriasis alone.13 24 Cohort studies found that nail psoriasis, particularly pitting, was also a positive predictor for PsA development.5 23 Psoriatic patients with nail disease have a greater magnitude of underlying systemic subclinical enthesopathy than those with normal nails. Nail matrix and bed are in close proximity with the entheses of the distal interphalangeal joints.26 Among psoriasis-related metabolic comorbidities, obesity has been recognised as a strong risk factor for PsA, because of its proinflammatory load and greater biomechanical stresses on joints and entheses.9 27 In this study, we found that duration of psoriasis correlated positively with a higher risk of developing PsA. To date, few studies have examined the association between psoriasis duration and risk of PsA.28 29 Although PsA incidence remains constant following initial diagnosis of psoriasis among patients seen in European dermatology clinics, conflicting data were found with regards to an association between age of psoriasis onset and risk of PsA.30
Our study has some important limitations that should be mentioned, including its retrospective, non-randomised intervention design with consequent possible selection, observational and immortality biases. Confounding by indication is another major limitation of the study. Since the study is not randomised, the patient’s likelihood of receiving treatment with bDMARDs or nb-UVB phototherapy was different and clinically influenced by the extent and localisation of skin lesions, but also by the patient’s willingness to come to the hospital 2–3 times a week for nb-UVB phototherapy, or by some coexisting comorbidities (for example, prior history of melanoma or non-melanoma skin cancers and the use of photosensitizing drugs such as diuretics). In order to try to adjust the aforementioned confounding bias by indication due to the non-randomised intervention study design, we also performed a PSM procedure, which showed that treatment with bDMARDs failed to show any significant association with the risk of incident PsA compared with nb-UVB phototherapy. However, these latter results should be interpreted with some degree of caution, because the number of patients included in this propensity score analysis was too small to draw any firm conclusion about the long-term effect of bDMARDs on PsA development. In addition, as partly expected, we believe that the PSM for baseline PASI, which is one of most important variables to decide the type of treatment for psoriasis in clinical practice, would abolish any protective effect of bDMARDs on PsA development in this analysis.
Finally, a subgroup analysis examining the effects of different bDMARD classes on the risk of incident PsA could not be performed because of the relatively small sample size of this study. In addition, soluble markers of inflammation and genetic factors have not been investigated. Notwithstanding these limitations, the major strengths of our study are the completeness of the database, the lack of missing data and the accuracy for PsA diagnosis that was always supported by an expert rheumatologist.
In conclusion, the results of this non-randomised intervention study suggest that continue therapeutic intervention with bDMARDs may reduce the risk of incident PsA in patients with moderate-to-severe chronic plaque psoriasis. Future large prospective and intervention studies are needed to further validate these findings in independent samples.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. These are deidentified participant dataAll the data are available at paolo.gisondi@univr.it. There is no embrago for the data.
Ethics statements
Patient consent for publication
Ethics approval
The local ethics committee approved the study protocol. The ethics committee exempted such kind of research from the informed consent requirement because we only accessed retrospectively a de-identified database for the purpose of data analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2021 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
Handling editor Josef S Smolen
Contributors FB performed all statistical analyses, contributed to writing the manuscript and visited the patients of the study population. PG designed the study, contributed to writing the manuscript and visited the patients of the study population. GT contributed to perform statistical analyses, and writing the manuscript. LI visited the patients of the study population and revised the manuscript. GG visited the patients of the study population and revised the final version of the manuscript.
Funding This work was supported by the European Union’s Horizon 2020 Research andInnovation Program (Grant agreement n. 848028).
Competing interests PG has been a consultant and/or speaker for Abbvie, Almirall, Amgen, Janssen, Leo-pharma, Eli Lilly, Novartis, Pierre Fabre, Sandoz, Sanofi, and UCB. LI served as consultant and/or speaker for AbbVie, Amgen, Biogen, Merck Sharp & Dohme, Eli-Lilly, Novartis, Celgene, Sandoz. GG served as consultant and/or speaker for AbbVie, Abiogen, Almirall, Amgen, Biogen, Boehringer-Ingelheim, Bristol-Meyers Squibb, Celltrion, Eli-Lilly, Genzyme, Leo Pharma, Novartis, OM Pharma, Pfizer, Regeneron, Samsung Sanofi and UCB.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.