Article Text

Statistics from Altmetric.com
We read with interest the recent work in Annals of the Rheumatic Diseases by Bacon and colleagues regarding the relationship between cartilage loss and pain in patients with knee osteoarthritis (OA).1 The authors included 600 participants within the Osteoarthritis Initiative and found that cartilage loss was significantly associated with a small degree of worsening in pain over 24 months. The relation between cartilage thickness loss and pain was partially mediated by synovitis change, rather than by changes in bone marrow lesions. This finding prompted us to reconsider the relation between cartilage loss and pain, and the clinical efficacy of the chondroprotective application in the treatment of knee OA. Their excellent and important work adds to our knowledge base, but we do have two minor points that may help to contextualise findings from this study and contribute to further investigations.
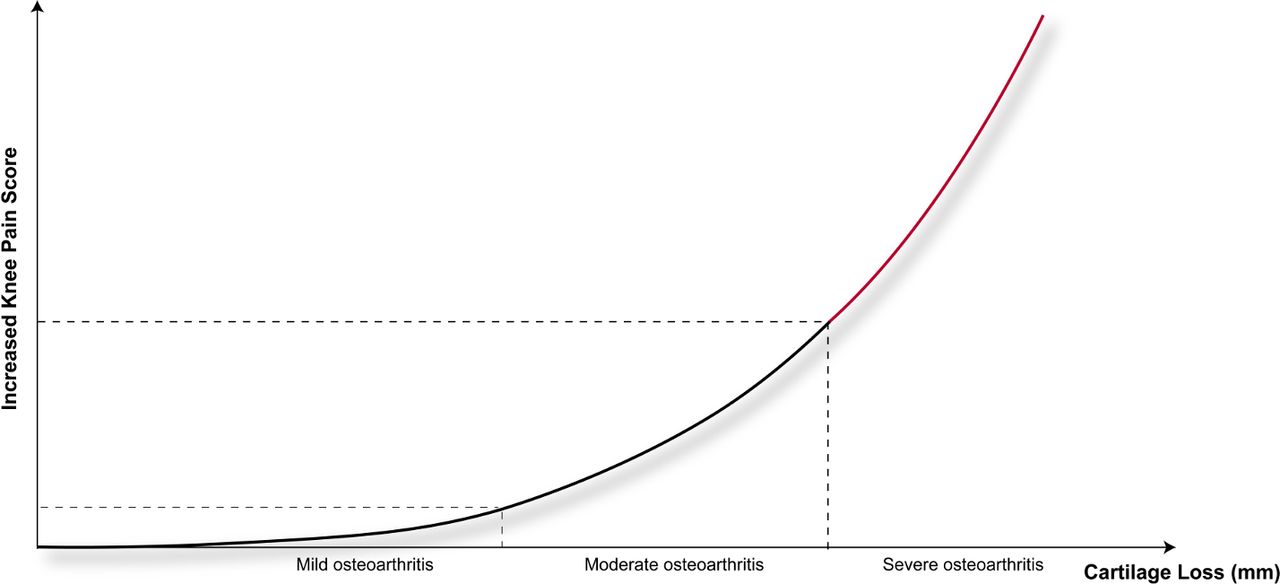
First, the predominant patient population included in this study was mild to moderate OA by Kellgren-Lawrence (K&L) grade, which is the typical population in whom chondroprotective agents are indicated.2 However, in this study, neither patients with severe OA (K&L grade 4) were included,3 nor subanalysis based on the K&L grade was performed. As OA-related knee pain usually becomes more severe over time,4 it is conceivable that there might exist a cumulative effect that the weak association of cartilage loss with pain could be stronger along the degenerative process of the knee (figure 1). Therefore, it remains unclear whether there exists a dose–response relationship between cartilage loss and pain worsening, and further studies are warranted to investigate if there was a dynamic association between cartilage loss and knee pain during the degenerative process.
{kind=link}
The possible dose–response relationship between cartilage loss and knee pain in osteoarthritis. Compared with patients with mild to moderate knee osteoarthritis, a loss of 0.1 mm of cartilage thickness in patients with severe knee osteoarthritis may associated with a higher increased knee pain score.
Second, the robustness of the results and the conclusion is severely biased by using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain score as the outcome. Although the WOMAC pain scale is a well-established, validated instrument to measure the pain level during specific activities that likely to cause OA pain,1 it only provides a summary of temporal or short-term pain severity, while the duration of pain is ignored. Considering the knee pain in OA is chronic, intermittent, activity related and varies over time,4 the WOMAC pain scale is not an ideal assessment tool to analyse the relationship between cartilage loss and knee pain, even if WOMAC pain scale has been widely used in similar studies.5–7 Thus, the findings should be interpreted with caution, and chronic pain assessment tools8–10 should be adopted to accurately and continuously measure the pain intensity and pain duration. If the continuous knee pain was cumulatively calculated, we could understand exactly how or to what extent the loss of cartilage thickness is associated with knee pain in OA.
Ethics statements
Patient consent for publication
Footnotes
X-DW and DW contributed equally.
Contributors XDW, DW, WH and GXQ contributed substantially to conception and design; drafted the article; gave final approval of the version to be published; and agreed to act as guarantors of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; internally peer reviewed.