Article Text

Statistics from Altmetric.com
We read with interest the letter by Simpson et al reporting the use of dupilumab in a patient with IgG4-related disease (IgG4-RD).1 Indeed blocking the IL-4/IL-13 pathway is tempting, considering the roles of these cytokines and the physiopathological changes observed during IgG4-RD.2 3
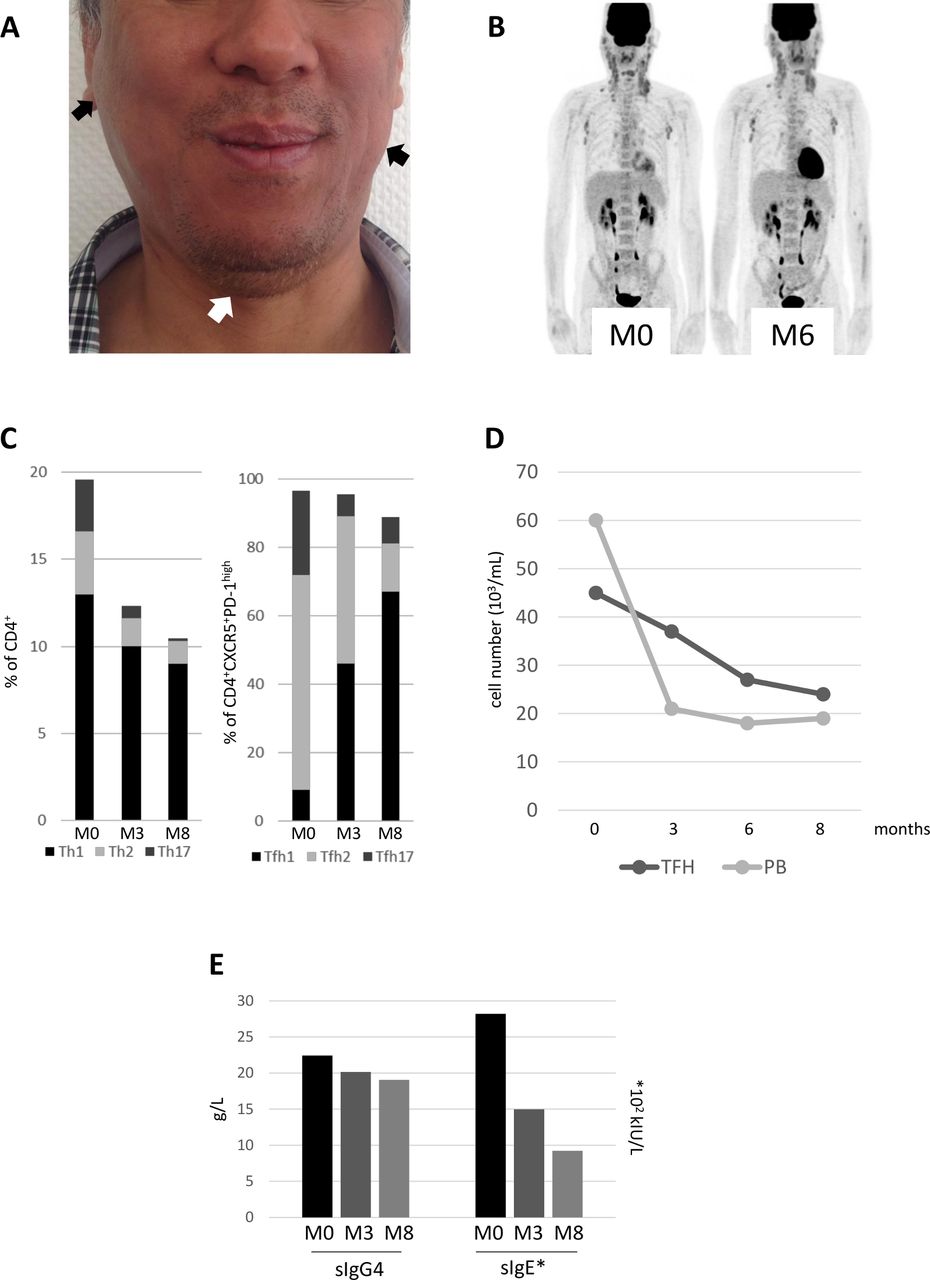
We have also treated with dupilumab a 51-year-old man with IgG4-related dacryoadenitis and sialadenitis (bilateral lacrimal, parotid, sublingual and submandibular involvement, pattern of Mikulicz syndrome). Left submandibular salivary gland and two cervical lymph nodes biopsies concluded, respectively, to lymphoplasmacytic polyclonal infiltration and reactive hyperplasia. Immunohistochemistry was only available on lymph nodes, showing an IgG4 +/CD138+ plasma cells ratio over 40% with 40 IgG4 + plasma cells/high power field. Serum IgG4 and IgE levels were found to be 17.7 g/L (normal range <0.8 g/L) and 3499 kIU/L (normal range <100 kIU/L), respectively, with normal complete blood count, liver and renal function tests. According to the 2019 American College of Rheumatology/European League Against Rheumatism classification criteria for IgG4-RD, entry criteria were met, no exclusion criteria were present, and the total points score was 29 (≥20).4 Clinical and radiological evaluation revealed no other IgG4-related involvement, except for cervical and axillary lymph nodes (figure 1A,B). The patient had cervical marked discomfort without sicca syndrome. Salivary glands and lymph nodes involvement improved after a 3 months steroid course but relapsed. A second course of steroids was associated with rituximab (two infusions of 1000 mg, 15 days apart) with clinical, biological (serum IgG4 level reduced to 7.59 g/L) and radiological response, but a new relapse occurred 1 year later. Because the patient also presented chronic rhinosinusitis with nasal polyps, a medical history of asthma and urticarial manifestations, a treatment with dupilumab was introduced without any other treatment, with an initial 600 mg subcutaneous injection, followed by a 300 mg subcutaneous injection every other week for 8 months. Rapidly the patient reported improvement of allergic rhinitis manifestations, but after an 8 months treatment course with dupilumab, salivary gland and lymph nodes involvements remained unchanged on clinical and radiological evaluation (figure 1B). Blood evaluation showed under dupilumab a decrease of total T helper 2 cells, T follicular helper (Tfh) cells, Tfh2 cells and plasmablasts after 3 and 8 months of treatment (figure 1C,D). Serum IgE significantly declined, but serum IgG4 only slightly decreased during the treatment (figure 1E).
{kind=link}
(A) Patient’s initial clinical findings before dupilumab treatment showed bilateral parotid (black arrows), sublingual (white arrow), submandibular glands and cervical lymph nodes involvements. (B) 18FDG-PET/CT scan before and 6 months after dupilumab treatment alone showed no improvement of salivary glands and lymph nodes involvements. (C) Proportion over time under dupilumab of T helper (Th)1 (IFNg+), Th2 (IL4+) and Th17 (IL17+) cells among T CD3+CD4+ cells; and proportion over time under dupilumab of T follicular helper (Tfh)1 (CD4+CXCR5+PD-1high CXCR3+CCR6-), Tfh2 (CD4+CXCR5+PD-1high CXCR3-CCR6-) and Tfh17 (CD4+CXCR5+PD-1highCXCR3-CCR6+) cells among Tfh (CD4+CXCR5+PD-1high) cells. (D) Absolute plasmablast (PB) (CD19+CD27highCD38high) and Tfh (CD4+CXCR5+PD-1high) count (103/mL) at baseline (month 0) and under dupilumab (months 3, 6 and 8). (E) Serum IgG4 (g/L) and IgE (102 kIU/L) levels at baseline (month 0) and under dupilumab (months 3 and 8). IFNg, interferon gamma; IL4, interleukin-4.
Glucocorticoids are the first line agent for remission induction in patients with IgG4-RD, with a high rate of response but frequent relapse during tapering or after discontinuation.5 Different maintenance therapy has been proposed, such as low-dose steroids, conventional steroid-sparing medications (azathioprine, mycophenolate mofetil, methotrexate) or rituximab, with different profiles of efficacy and side effects. In the case reported by Simpson et al, prednisone was administered initially during 2 months. We think that the initial clinical and biological response reported by Simpson et al could be attributable to steroids rather than to dupilumab, and that the radiological response presented at 12 months (and not assessed at 3 months) should be analysed cautiously. Indeed, in our patient, we observed no clinical nor radiological improvement after an 8-month course of dupilumab alone without steroids. However, we observed significant and interesting immunological improvements, with a marked decrease of Tfh2 cells and plasmablasts, which have been both correlated with disease activity,2 3 6 despite the fact that serum IgG4 remained fairly stable. We think that these observations taken together suggest that dupilumab could be an interesting and well tolerated therapeutic approach in IgG4-RD, but rather as relapse-free maintenance therapy after induction treatment. This strategy should be further evaluated in a dedicated clinical trial.
Ethics statements
Patient consent for publication
Footnotes
Contributors ME and NS: conceived the hypothesis, analysed data and drafted the manuscript. BDS-M, RM, AG and FV: analysed data, critically revised the manuscript and gave the final approval. CP: acquisition of data, critically revised the manuscript and gave the final approval.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.