Article Text

Abstract
Objectives The aim of this study is to determine whether the ‘programmed’ infliximab (IFX) treatment strategy (for which the dose of IFX was adjusted based on the baseline serum tumour necrosis factor α (TNF-α)) is beneficial to induction of clinical remission after 54 weeks and sustained discontinuation of IFX for 1 year.
Methods In this multicentre randomised trial, patients with IFX-naïve rheumatoid arthritis with inadequate response to methotrexate were randomised to two groups; patients in programmed treatment group received 3 mg/kg IFX until week 6 and after 14 weeks the dose of IFX was adjusted based on the baseline levels of serum TNF-α until week 54; patients in the standard treatment group received 3 mg/kg of IFX. Patients who achieved a simplified disease activity index (SDAI) ≤3.3 at week 54 discontinued IFX. The primary endpoint was the proportion of patients who sustained discontinuation of IFX at week 106.
Results A total of 337 patients were randomised. At week 54, 39.4% (67/170) in the programmed group and 32.3% (54/167) in the standard group attained remission (SDAI ≤3.3). At week 106, the 1-year sustained discontinuation rate was not significantly different between two groups; the programmed group 23.5% (40/170) and the standard group 21.6% (36/167), respectively (2.2% difference, 95% CI −6.6% to 11.0%; p=0.631). Baseline SDAI <26.0 was a statistically significant predictor of the successfully sustained discontinuation of IFX at week 106.
Conclusion Programmed treatment strategy did not statistically increase the sustained remission rate after 1 year discontinuation of IFX treatment.
- rheumatoid arthritis
- infliximab
- TNF-α
- randomized controlled trials
- remission
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
The goal of rheumatoid arthritis treatment has expanded to sustained remission without biological disease-modifying antirheumatic drugs, particularly in patients with infliximab (IFX) in sustained remission by the Remission induction by Remicade in RA patients (RRR) study and others. We also reported dose-escalation of IFX showed a significant interaction between baseline tumour necrosis factor (TNF) and the dose of IFX in the clinical response in the RISING study.
What does this study add?
A total of 337 patients were randomised to the ‘programmed’ IFX arm, in which the dose of IFX was adjusted based on the baseline serum TNF and the ‘standard’ arm treated with 3 mg/kg of IFX and 39.4% in the programmed arm and 32.3% in the standard arm attained simplified disease activity index (SDAI)≤3.3 at week 54. However, programmed treatment did not statistically increase the sustained remission rate after 1-year discontinuation of IFX: the programmed group 23.5% and the standard group 21.6%.
How might this impact on clinical practice or future developments?
Baseline SDAI<26.0 was a statistically significant predictor of the successfully sustained discontinuation of IFX at week 106, indicating that sufficient disease control by adequate dose of methotrexate is necessary before IFX is administered.
Introduction
Rheumatoid arthritis (RA) is a progressive systemic inflammatory disease characterised by joint destruction and functional disability.1 2 It is well known that proinflammatory cytokines such as tumour necrosis factor α (TNF-α) play central roles in the occurrence and progression of RA.3 Infliximab (IFX), an inhibitor of TNF-α, is one of the biological disease-modifying antirheumatic drugs (DMARDs); combined use of IFX and methotrexate (MTX) yields clinical and radiographic benefits in patients with RA with inadequate response to MTX (MTX-IR).4 Because the therapeutic effects of IFX (plus MTX) have been demonstrated in several clinical studies,5–9 the goal of RA treatment has expanded from the achievement of clinical remission to sustained remission without biological DMARDs, particularly in patients with RA in sustained remission.10–15
The first study reporting the possibility of biological-free treatment in patients with RA was the TNF20 study.8 The Behandelstrategieёn (BeSt) study also evaluated biological-free treatment in a much larger cohort.6 16 However, this study did not look at discontinuation of IFX after achieving sustained remission but rather low disease activity (LDA) by DAS44. The Remission induction by Remicade in RA patients (RRR) study was the first study that its endpoints were biological-free remission or LDA in established patients with RA with MTX-IR.17 Patients enrolled in that study had reached and maintained a disease activity score 28 (DAS28) of less than 3.2 for more than 24 weeks with IFX treatment and then agreed to discontinue the treatment. Among the 102 evaluable patients who completed the study, 56 (55%) maintained LDA after 1 year and exhibited no progression in terms of radiological damage or functional disturbance; 44 (43%) remained in clinical remission (DAS28 <2.6). In this context, subanalysis of the dose-escalation study of IFX with MTX (RISING study) showed a significant interaction between baseline TNF-α and the dose of IFX in the clinical response. Additionally, the clinical response and disease activity were significantly better when the treatment was used at 10 mg/kg than at 3 and 6 mg/kg, with high baseline TNF-α (baseline TNF-α values: 1.65 pg/mL or greater).18
Based on studies of ours and others, we assumed that serum levels of TNF-α could be a key indicator for optimal dosing of IFX to achieve a clinical remission and a sustained discontinuation of IFX for the treatment of RA. However, this clinical hypothesis has not been confirmed in a randomised controlled trial. Therefore, in this study, we aimed to determine whether the ‘programmed’ IFX treatment strategy, in which the dose of IFX was adjusted based on the baseline serum TNF, is beneficial to induction of clinical remission after 54 weeks and subsequent sustained discontinuation of IFX for 1 year. Hence, the study is called ‘Remission induction by Raising the dose of Remicade in RA’ (RRRR).
Methods
Study design and participants
The RRRR study was conducted as an open-label, parallel group, multicentre randomised controlled trial from April 2011 to September 2013.19 Patients were enrolled in 50 Japanese hospitals. Eligible patients were randomly assigned in a 1:1 ratio to receive either a standard IFX treatment or a ‘programmed’ IFX treatment with the dose of IFX based on the three categories of baseline TNF-α (low,<0.55 pg/mL; intermediate, ≥0.55 pg/mL and <1.65 pg/mL and high, ≥1.65 pg/mL). The standard treatment arm received 3 mg/kg IFX at 0, 2 and 6 weeks after enrolment. The same dose was taken every 8 weeks until 54 weeks. If the patients showed an simplified disease activity index (SDAI) of ≤3.3 at 54 weeks, they discontinued IFX. The programmed treatment arm received 3 mg/kg IFX at 0, 2 and 6 weeks, but the dose of IFX was selected based on baseline serum TNF-α after 14 weeks. If serum TNF-α was <0.55 pg/mL, IFX was kept at 3 mg/kg every 8 weeks after 14 weeks. If serum TNF-α was between 0.55 pg/mL and 1.65 pg/mL, IFX was increased to 6 mg/kg at 14 weeks and maintained at 6 mg/kg every 8 weeks after 22 weeks. If serum TNF-α was ≥1.65 pg/mL, IFX was increased to 6 mg/kg at 14 weeks and to 10 mg/kg at 22 weeks; a dose of 10 mg/kg was then administered every 8 weeks after 30 weeks. If the patients exhibited an SDAI ≤3.3 at 54 weeks, they discontinued IFX as in the standard treatment arm. In both treatment arms, discontinuation of IFX was maintained throughout follow-up until 158 weeks after enrolment unless patients exhibited clinical or radiological progression. Other details of the treatment plan, including concomitant drugs, are described elsewhere.19
Patients with RA were eligible for enrolment if they had active disease despite equal to or greater than 6 mg MTX weekly, were 18 years of age or older and had not previously used IFX. Exclusion criteria were: corticosteroid use >10 mg prednisolone equivalents/day; SDAI≤11.0; severe infections; active tuberculosis or evidence of latent tuberculosis; diagnosis of systemic lupus erythematosus or any other form of concomitant arthritis and congestive heart failure; we also excluded women who were pregnant or lactating during or 6 months after treatment. All patients gave written informed consent in accordance with the Declaration of Helsinki, and the trial was approved by the institutional review board at each participating institution. This trial was registered with University Hospital Medical Information Network (UMIN; number UMIN000005113).
Randomisation and masking
To ensure a balanced group design, the Clinical Research and Medical Innovation Center at Hokkaido University Hospital performed the randomisation at week 10 using a computerised random number generator. Patients were randomly assigned in a 1:1 ratio to the standard or programmed treatment arm using permuted blocks within each stratum; block size was selected as four or six at random. Sixteen strata for randomisation consisted of disease duration (less than 3 years or not), baseline SDAI (less than 26 or not) and baseline TNF-α (<0.55 pg/mL, 0.55–1.65 pg/mL or >1.65 pg/mL). Treatment allocation was blinded for the reviewer of the patients’ disease but open to both patients and physicians.
Outcome measures
The primary endpoint was the proportion of patients who sustained discontinuation of IFX 1 year after discontinuation at 54 weeks after the first administration. The secondary endpoints were the proportion of patients achieving the following: clinical remission at the time of 54 weeks after the first administration of IFX; sustained discontinuation of IFX at 2 years after discontinuation of IFX; clinical remission based on SDAI and changes in SDAI from baseline at each time point; clinical remission based on DAS28-ESR, DAS28-CRP and Boolean-based definitions, and change in each value at each time point; as well as radiographs of the hands, wrists and feet, which were centrally assessed and assigned a score according to the van der Heijde modifications of the total Sharp score (modified total Sharp score); rheumatoid factor and matrix metalloproteinase-3 levels; health assessment questionnaire (HAQ) and EQ-5D score; serum IFX concentration at 54 weeks after the first administration of IFX and adverse events.
Statistical analysis
Sample size was determined by assuming that the proportions of clinical remission (SDAI ≤3.3) were 21% and 34% for the standard and programmed treatment arms, respectively.18 After discontinuation of IFX, we also assumed that the proportion of patients who sustained discontinuation was 55% in the standard treatment arm and 65% in the programmed treatment arm.17 Therefore, the proportions of patients who sustained discontinuation of IFX at 1 year after discontinuation of IFX at 54 weeks after first administration in the standard and programmed treatment arms were calculated as 11.6% and 22.1%, respectively. Based on these values, approximately 200 randomised patients were needed for each treatment arm in order to achieve 80% power at a two-sided 5% level of significance (400 patients in total).
The analysis population included all patients enrolled and randomised in the trial (intention-to-treat population). For primary analysis, the proportion of sustained discontinuation at 1 year after discontinuation of IFX at 54 weeks was compared using the Cochrane–Mantel–Haenszel test with stratification factors (disease duration and baseline SDAI). The risk difference of the proportion of sustained discontinuation at 1 year after discontinuation of IFX and its 95% CI were calculated. To confirm the robustness of the primary results, the same analyses were conducted in a population restricted to patients who completed the planned IFX and entered the IFX-free period (secondary analysis population). Subgroup analysis based on disease duration, baseline SDAI and baseline TNF-α concentration was conducted.
For the secondary endpoints, we compared the proportion of patients with clinical remission at 54 weeks and the proportion of patients who sustained discontinuation of IFX at 2 years after discontinuation between arms. The proportions of clinical remission according to DAS28-ESR were also analysed. Longitudinal data in SDAI, DAS28-ESR, HAQ and total Sharp score were analysed using a mixed model for repeated measures.20 Means and SD were calculated for all time points and displayed as a transition diagram. Time to discontinuation of IFX and time until the loss of efficacy was plotted using the Kaplan–Meier method. As an exploratory analysis, logistic regression analysis was performed to identify the baseline predictors of sustained remission after 1 year.
Safety analysis was conducted based on the safety population, which included all patients who enrolled in the study and received IFX at least once. Combined results from both treatment arms are shown before randomisation, and separate results for each treatment arm are shown separately for each randomisation. The numbers and proportions of adverse events were calculated.
All p values calculated in the analysis were two-sided and were not adjusted for multiple testing because no interim analysis was planned. P values less than 0.05 were considered to indicate statistical significance. SAS V.9.4 (SAS Institute, Cary, North Carolina, USA) was used for all the analyses.
Results
Study population
Between April 2011 and September 2013, 415 patients were assessed for eligibility and 405 patients were enrolled in the RRRR study (figure 1). After the induction phase, 337 patients were randomised into the standard treatment arm (167 patients) and programmed treatment arm (170). Reasons of ineligibility before the randomisation are shown in online supplementary table 1. Patient demographics and disease activity were balanced among treatment groups at baseline (table 1). The percentage of patients with baseline serum TNF-α≥1.65 pg/mL was higher in the RRRR Study than in the RISING study.18
Supplemental material
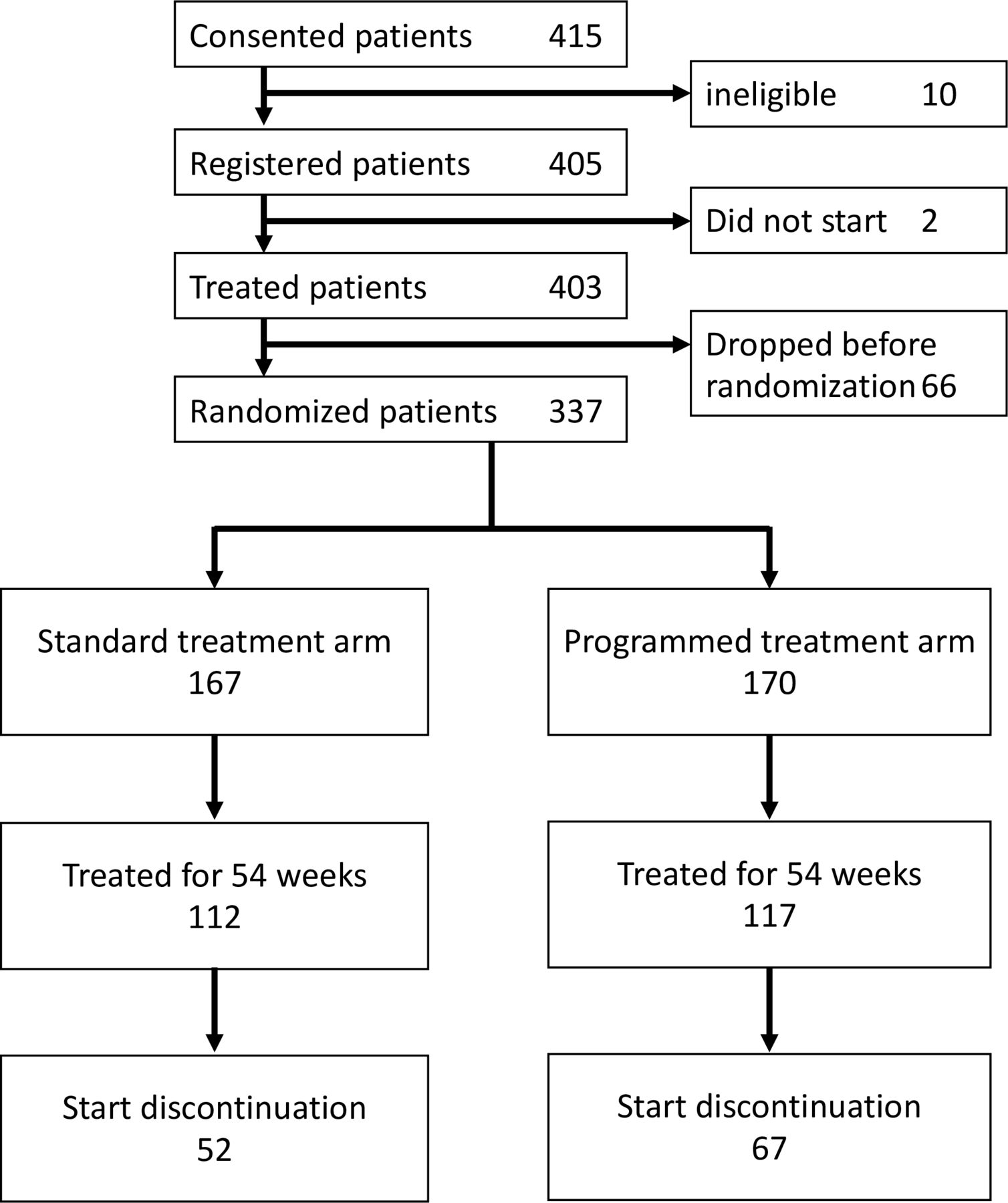
Consort flow diagram.
Baseline characteristics
In the programmed treatment arm, 51 patients were allocated into the TNF-low group (received 3 mg/kg IFX), 68 into the TNF-int group (6 mg/kg after 22 weeks) and 51 into the TNF-high group (10 mg/kg after 22 weeks). One-hundred and twenty patients in the standard treatment arm and 117 patients in the programmed treatment arm completed IFX treatment for 54 weeks after enrolment. Reasons of study withdrawal before 54 are shown in newly made online supplementary table 2. The median number of injections was 9 (range, 4–10) in both arms.
Disease activity during IFX treatment
At the last IFX treatment after 54 weeks, the difference in the least-square means in SDAI and DAS28-ESR was not statistically significant (p=0.091 and p=0.120, respectively) (figure 2A–B). However, we observed statistically significant differences in SDAI and DAS28-ESR in cases for which the missing value was imputed using the last observation carried forward (LOCF) method at the last IFX treatment after 54 weeks. After 54 weeks, the proportion of clinical remission in SDAI (SDAI ≤3.3) was 32.3% (54/167) in the standard treatment arm and 39.4% (67/170) in the programmed treatment arm (figure 2C). Based on DAS28-ESR, the proportion of clinical remission was 31.1% (52/167) in the standard treatment arm and 40.0% (68/170) in the programmed treatment arm after 54 weeks (figures 2D and 3). Ultimately, 52 patients in the standard treatment arm and 67 patients in the programmed treatment arm started discontinuation of IFX treatment (figure 1).
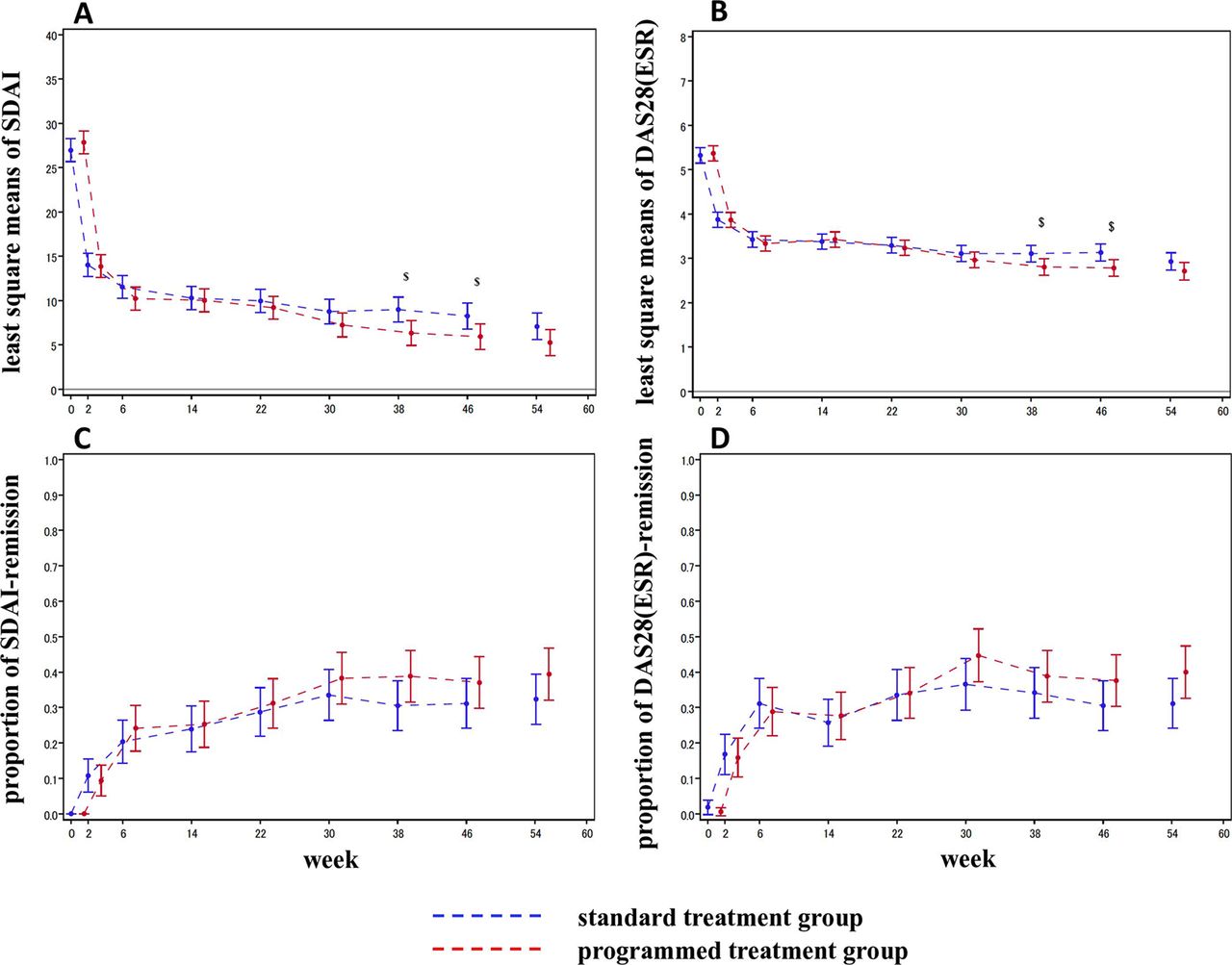
Change from baseline in SDAI (A) and DAS28-ESR, and proportion of remission based on SDAI (C) and DAS28-ESR (D). Least square means and 95% CIs were estimated plotted for the standard treatment group and programmed treatment group. $ shows p<0.05. DAS28-ESR, disease activity score in 28 joints using erythrocyte sedimentation rate; SDAI, simplified disease activity index.

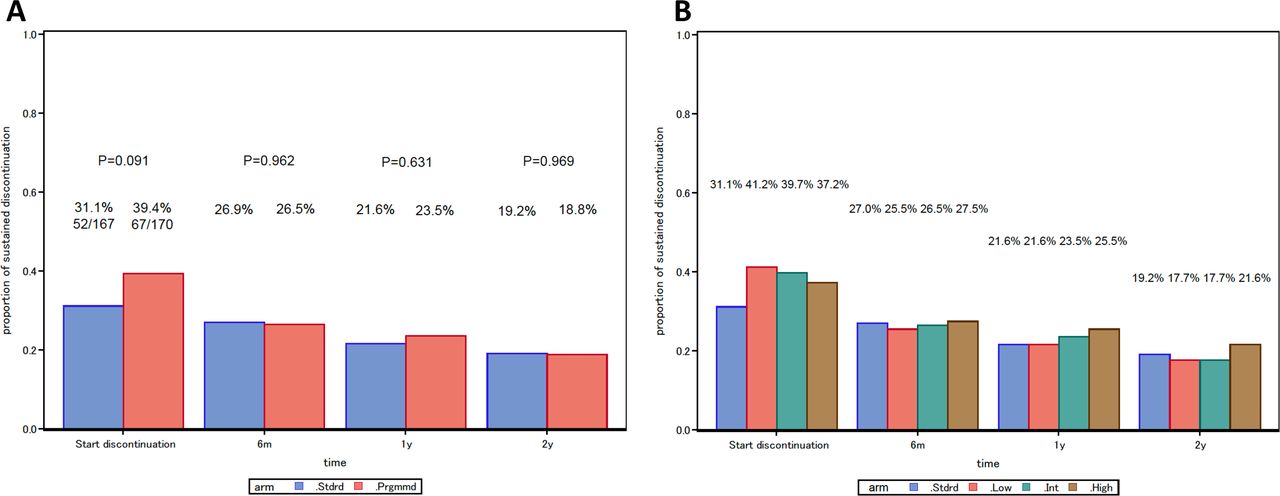
Proportions of sustained discontinuation by the standard and programmed treatment group (A) and by the dose of infliximab (B) in patients randomised in RRRR study. The standard treatment group and TNF-low group received 3 mg/kg of infliximab, TNF-int group received 6 mg/kg after 22 weeks and TNF-high group received 10 mg/kg after 22 weeks. RRRR, Remission induction by Raising the dose of Remicade in Rheumatoid arthritis; TNF, tumour necrosis factor.
Sustained discontinuation after IFX discontinuation
The proportion of sustained discontinuation of IFX 1 year after discontinuation at 54 weeks was not significantly different between two groups; the programmed treatment arm 23.5% (40/170) and the standard treatment arm 21.6% (36/167), respectively (2.2% difference, 95% CI −6.6% to 11.0%; p=0.631) (figure 3). At other time points, the proportion of sustained discontinuation was similar in both arms, as shown in figure 2A. In the programmed treatment arm, the proportions of sustained discontinuation at 1 year were 21.6% in TNF-low group, 23.5% in the TNF-int group and 25.5% in the TNF-high group. There was no statistically clear trend in the dose of IFX (p=0.642). The main reasons for stopping discontinuation was re-introduction of IFX (5/52 (9.6%) in the standard treatment arm and 16/67 (23.9%) in the programmed treatment arm), introduction of other biological antirheumatic drugs (6/52 (11.5%) in the standard treatment arm and 6/67 (9.0%) in the programmed treatment arm) and clinical judgement (5/52 (9.6%) in the standard treatment arm and 10/67 (14.9%) in the programmed treatment arm). Least-square means of trajectories in total Sharp score and HAQ during the study period were also were similar in both arms (data not shown).
Factors associated with sustained discontinuation at 1 year
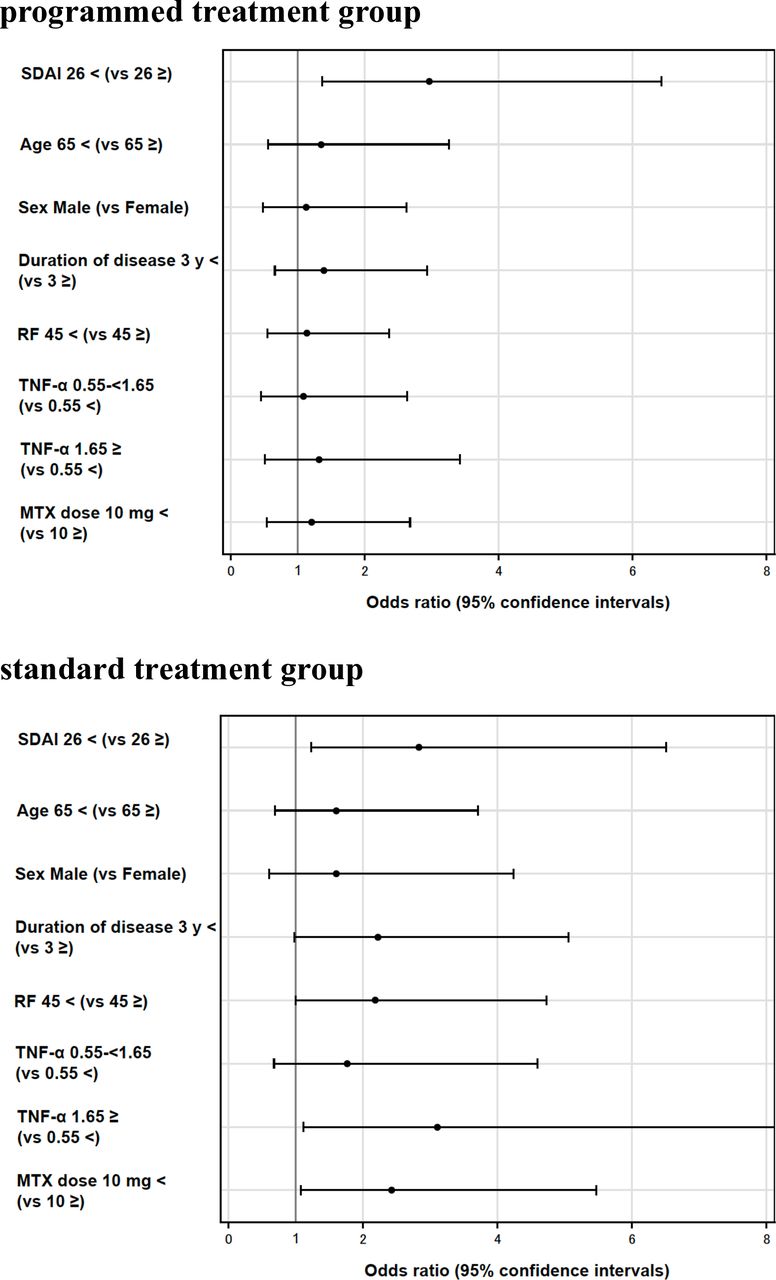
As an exploratory analysis, we used a logistic regression model to evaluate the association between baseline characteristics and sustained remission after 1 year by arms. In both arms, baseline SDAI <26.0 was a statistically significant predictor of sustained discontinuation at 1 year (OR=2.97% and 95% CI 1.37 to 6.43 in the programmed treatment arm; OR=2.83% and 95% CI 1.24 to 6.50 in the standard treatment arm) (figure 4). RF less than 45 (OR=2.18; 95% CI 1.01 to 4.73), baseline TNF-α higher than 1.65 (OR=3.11; 95% CI 1.12 to 8.67) and baseline MTX dose lower than 10 mg/kg (OR=2.43; 95% CI 1.08 to 5.47) were statistically significant predictors in the standard treatment arm, but not in the programmed treatment arm (online supplementary table S3).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between clinical background factors and the sustained discontinuation at 1 year in the multiple logistic regression analysis. MTX, methotrexate; RF, rheumatoid factor; SDAI, simplified disease activity index; TNF-α, tumour necrosis factor α.
Safety analysis
Twenty infection events (0.24 per 100 weeks) were observed in the standard treatment arm, and 22 events (0.26 per 100 weeks) in the programmed treatment arm (table 2). The incidence rates were comparable between the two arms. In addition, there was no trend in the incidence of any adverse events against the IFX dose in the programmed treatment arm.
Adverse events in each arm
Discussion
After achieving remission through combined use of MTX and TNF-inhibitors, dose reduction or withdrawal of TNF inhibitors may be considered out of concern for adverse events or treatment cost.10–15 However, several studies have suggested that few patients with established RA can discontinue bDMARDs without losing remission and that patients in sustained deep remission are more likely to be able to discontinue bDMARDs.21 We have also reported that withdrawal of TNF inhibitors in established RA was possible in the presence or maintenance of deep remission, according to a lower cut-off value than 2.6: the significant DAS28 cut-off point was determined to be <2.2 in the RRR trial and <2.0 in the HONOR trial.17 22 Therefore, we hypothesised that deep remission can be achieved by intensive and finely tuned treatments with the appropriate dose of TNF inhibitors. Meanwhile, the RISING study revealed that IFX dose, adjusted based on serum levels of TNF at baseline, was associated with the clinical response to IFX in patients with RA: a higher dose of IFX was necessary in patients with a high baseline TNF, whereas lower doses of IFX were sufficient for those with low baseline TNF.18 Thus, the RRRR study was designed to evaluate the clinical remission after 54 weeks of ‘programmed’ treatment, in which the dose of IFX for each patient was determined by baseline serum TNF-α, and subsequent sustained discontinuation of IFX for 1 year, compared with the ‘standard’ treatment.
The proportion of remission at week 54 was 32.3% and 31.1% in the standard treatment arm and 39.4% and 40.0% in the programmed treatment strategy, measured by SDAI and DAS28-ESR, respectively. There was no statistically significant difference in least-square means in SDAI and DAS28-ESR. Serum levels in IFX at the last administration were significantly higher in the programmed group than in the standard group, indicating that the study could theoretically be successful. Thus, the obtained results partly failed to support the results in the RISING study, which might depend on differences in patient characteristics at baseline, including much lower disease activity and use of higher doses of MTX in the RRRR study. Alternatively, statistical methods differed between the two studies, and significant differences in SDAI and DAS28-ESR were observed, if the missing value was imputed using the LOCF method at the last IFX treatment after 54 weeks, as was done in the RRR and RISING studies.17 18
In terms of the primary endpoint, there was no statistically significant difference in the proportion of sustained discontinuation at 1 year after withdrawal of IFX between the standard treatment arm (21.6%) and the programmed treatment arm (23.5%). In addition, there was no statistically clear trend in dose of IFX in the programmed group. At other time points, the proportion of sustained discontinuation was similar in both groups. The proportion of sustained remission after the withdrawal of IFX was also comparable for 1 year between two groups. In both arms, baseline SDAI <26 was a statistically significant predictor of sustained discontinuation at 1 year (OR=2.97 in the programmed arm and 2.83 in the standard arm) by logistic regression model. This exploratory analysis implies that the success of sustained discontinuation of IFX depends on disease activity at baseline, and that sufficient disease control by adequate dose of MTX is required before IFX is administered. Furthermore, the results did not support our initial hypothesis that deep remission and subsequent sustained discontinuation of IFX can be achieved by intensive and finely tuned treatments with appropriate doses of TNF inhibitors. There was no statistically significant difference in the proportion of deep remission, defined as DAS28 <2.2, at the last administration of IFX between the standard treatment arm (22.8%) and the programmed treatment arm (26.5%), which could result in failure of sustained discontinuation of IFX. On the other hand, the incidence rates of infections and other safety signals were comparable between the two arms, suggesting that dose escalation was tolerated in the study. Thus, the fine tuning of IFX-dose based on serum levels of TNF represents a key factor for achievement of remission defined by SDAI and DAS28-ESR, but may not be related to deep remission. If serum levels of RF are less than 45, serum levels of TNF-α are higher than 1.65, or disease activity is controlled with less than 10 mg/kg of MTX, standard treatment may be intense enough to achieve successful discontinuation of IFX.
This study had several limitations. Initially, the RRRR study was not a double-blinded study. In addition to ethical issues and budgetary reasons, there were technical problems: specifically, different numbers of vials of IFX had to be prepared when patients were treated with 3, 6 and 10 mg/kg. The study was undertaken with coverage by health insurance. Second, patients were treated with different doses of IFX only for 40 weeks, and five doses were administered to each patient. This regimen might not be intense enough to achieve differences in disease control between the two groups. Indeed, as shown in figure 2A and B, the differences in SDAI and DAS28-ESR gradually increased according to the number of doses. Third, this trial adopted the escalation dose for the 6 mg and 10 mg of IFX in the programmed treatment arm according to the approved usage by the government. However, it might reduce the efficacy of the programmed treatment strategy since the very start time may be the most important period for determining outcome. Finally, the obtained results pertain to IFX and probably to other TNF inhibitors, but not to IL-6 inhibitors or JAK inhibitors that directly affect the acute-phase response and lead to very low DAS28 values.
Taken together, the findings of the RRRR study reveal that the programmed treatment strategy using different doses of IFX based on the baseline levels of serum TNF-α did not increase the sustained remission rate 1 year after withdrawal of IFX treatment at week 106. However, in order to facilitate decision-making by patients and rheumatologists, more efforts are needed to determine the patient profile most likely to benefit from discontinuation of biological DMARDs.
References
Supplementary materials
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2020 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
Handling editor Josef S Smolen
Contributors All authors made essential and valuable contributions to the patient assessment, data collection and manuscript. In addition to the above, YT contributed to study design, study conduct, data analysis, KO, NH and NS did data management and data analysis and TaKo, NM, TM and TsTa did the study design and study conduct.
Funding This is an investigator-initiated trial sponsored by a Research Grant-In-Aid for Scientific Research from the Ministry of Health, Labor and Welfare of Japan. A radiological evaluation was funded by Mitsubishi Tanabe Pharma Co, Ltd.
Competing interests YT has received consulting fees, speaking fees and/or honoraria from AbbVie GK; Chugai Pharmaceutical Co Ltd; Daiichi-Sankyo Co Ltd; Bristol-Myers, Mitsubishi Tanabe Pharma Co; Astellas Pharma Inc; Takeda Pharmaceutical Co Ltd; Pfizer Japan Inc; Teijin Pharma; Asahikasei Pharma Corp; YL Biologics; Sanofi KK: Janssen Pharmaceutical KK; Eli Lilly Japan KK and GlaxoSmithKline KK and has received research grants from Mitsubishi Tanabe Pharma Co; Takeda Pharmaceutical Co, Ltd; Daiichi Sankyo Co Ltd; Chugai Pharmaceutical Co Ltd; Bristol-Myers KK; MSD KK; Astellas Pharma Inc; AbbVie GK; Eisai Co Ltd K Oba has received honoraria from Takeda Pharmaceutical Co Ltd; Ono Pharmaceutical Co Ltd; Eisai Co Ltd; Chugai Pharmaceutical Co Ltd; Daiichi- Sankyo Co Ltd. TT has received grants from Astellas Pharma Inc and Pfizer Japan, Inc; Chugai Pharmaceutical Co Ltd; Daiichi Sankyo Co Ltd; Takeda Pharmaceutical Co Ltd; AbbVie GK; Asahikasei Pharma Corp; Mitsubishi Tanabe Pharma Co; Pfizer Japan Inc; Eisai Co Ltd; AYUMI Pharmaceutical Co; Nipponkayaku Co Ltd; Novartis Pharma KK; Shionogi AbbVie GK; AYUMI Pharmaceutical Co; Eisai Co Ltd; Gilead Sciences, Inc; GlaxoSmithKline KK; Sanofi KK; Taiho Pharmaceutical Co Ltd; Mitsubishi Tanabe Pharma Co; Diaichi Sankyo Co Ltd; Chugai Pharmaceutical Co Ltd; Taisho Pharmaceutical Co Ltd; Eli Lilly Japan KK; Novartis Pharma KK; Boehringer-ingelheim Co Ltd; Nipponkayaku Co Ltd; Pfizer Japan Inc; Bristol–Myers KK; Janssen Pharmaceutical KK; UCB Japan Co Ltd. TM received research grants and/or speaking fees from Asahikasei Pharma Corp; Astellas Pharma Inc; AYUMI Pharmaceutical Corporation; Bristol-Myers Squibb; Chugai Pharmaceutical Co Ltd; Diaichi-Sankyo Co Ltd; Eisai Co Ltd; Eli Lilly Japan KK; Mitsubishi-Tanabe Pharma Co; MSD KK; Nippon Kayaku Co Ltd; Pfizer Japan Inc; Sanofi KK; Takeda Pharmaceutical Co Ltd. TK has received speaking fees from AbbVie GK; ASKA Pharmaceutical Co Ltd; Astellas Pharma Inc; Bristol-Myers KK; Chugai Pharmaceutical Co Ltd; Diaichi-Sankyo Co Ltd; Eisai Co Ltd; Mitsubishi Tanabe Pharma Co; Pfizer Japan Inc; Teijin Pharma; UCB Pharma and consulting fees from Bristol-Myers KK; Eli Lilly Japan KK; Pfizer Japan Inc; Diaichi-Sankyo Co Ltd; Sanofi KK. SH has received research grants from Eli Lilly Japan KK; UCB Pharma; consultancy fee from Bristol-Myers Squibb; Celgene KK; Janssen Pharmaceutical KK; Novartis Pharma KK and speaker’s fees from AbbVie GK; Asahikasei Pharma Corp; Astellas Pharma Inc; AYUMI Pharmaceutical Co; Bristol-Myers Squibb; Chugai Pharmaceutical Co Ltd; Eisai Co Ltd; Eli Lilly Japan KK; Janssen Pharmaceutical KK; Kissei Pharmaceutical Co Ltd; Pfizer Japan Inc; Sanofi KK; Takeda Pharmaceutical Co Ltd; Mitsubishi Tanabe Pharma Co; UCB Pharma. ET has received lecture fees or consulting fees from Asahi Kasei pharma co; Bristol Myers Squibb; Chugai Pharmaceutical Co Ltd; Diaichi Sankyo Co Ltd; Eisai Co Ltd; Janssen Pharmaceutical KK; Nippon Kayaku Co Ltd; Pfizer Japan Inc; Takeda Pharmaceutical Co Ltd; Taisho Toyama Pharmaceutical Co Ltd; UCB Pharma. YK has received grants or speaking fees from AbbVie GK; Astellas Pharma Inc; AYUMI Pharmaceutical Co; Bristol-Myers Squibb; Chugai Pharmaceutical Co Ltd; Eisai Co Ltd; Eli Lilly Japan KK; Hisamitsu Pharmaceutical Co Inc; Janssen Pharmaceutical KK; Novartis Pharma KK; Pfizer Japan Inc; Sanofi KK; Takeda Pharmaceutical Co Ltd; Mitsubishi Tanabe Pharma Co; UCB Pharma. KN has received speaking fees from UCB Pharma; Astellas Pharma Inc; Mitsubishi Tanabe Pharma Co and research grants from Mitsubishi Tanabe Pharma Co; Eisai Co Ltd. KA has received research grants from Asahi Kasei Pharma Co; Chugai Pharmaceutical Co Ltd and honoraria from Astellas Pharma Inc; Eli Lilly Japan KK; Pfizer Japan Inc; Mitsubishi Tanabe Pharma Co Ltd.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.