Article Text

Abstract
Introduction Antibodies against double-stranded DNA (anti-dsDNA) are a specific biomarker for systemic lupus erythematosus (SLE). The first WHO International Standard (IS) for anti-dsDNA (established in 1985), which was used to assign units to diagnostic tests, was exhausted over a decade ago.
Methods Plasma from a patient with SLE was first evaluated in 42 European laboratories. The plasma was thereafter used by the National Institute for Biological Standards and Control to prepare a candidate WHO reference preparation for lupus (anti-dsDNA) antibodies. That preparation, coded 15/174, was subjected to an international collaborative study, including 36 laboratories from 17 countries.
Results The plasma mainly contained anti-dsDNA, other anti-chromatin antibodies and anti-Ku. The international collaborative study showed that the field would benefit from 15/174 as a common reference reagent improving differences in performance between different assays. However, no statistically meaningful overall potency or assay parallelism and commutability could be shown.
Conclusion 15/174 cannot be considered equivalent to the first IS for anti-dsDNA (Wo/80) and was established as a WHO Reference Reagent for lupus (oligo-specific) anti-dsDNA antibodies with a nominal value of 100 units/ampoule. This preparation is intended to be used to align test methods quantifying levels of anti-dsDNA antibodies.
- systemic lupus erythematosus
- autoantibodies
- autoimmune diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Autoantibody reference reagents improve comparability between laboratories using different assays.
The First International Standard for anti-double-stranded DNA (dsDNA) is no longer available.
What does this study add?
This report describes the validation of 15/174, a new WHO Reference Reagent for anti-dsDNA.
How might this impact on clinical practice or future developments?
15/174 can be used to align test methods quantifying anti-dsDNA.
INTRODUCTION
Antibodies against double-stranded DNA (anti-dsDNA) are biomarkers for systemic lupus erythematosus (SLE).1 2 As a result, measurement of anti-dsDNA is widely used as a diagnostic and prognostic test for SLE, and there are a range of kits and tests available.3
The first WHO International Standard (IS) for anti-dsDNA denoted Wo/80 was established in 1985 to assign International Units (IU) to diagnostic tests.4 Wo/80 was exhausted over a decade ago and requires replacement.
MATERIALS AND METHODS
Raw material characterisation by 42 European laboratories
Plasmapheresis plasma from a female patient with SLE diagnosed according to the 1997 classification criteria5 6 was evaluated blindly by 42 European laboratories in the European Consensus Finding Study Group on autoantibodies, a.k.a. the EULAR Autoantibody Study Group (https://www.eular.org/investigative_rheumatology_study_groups.cfm). Sampling was approved by the local Institutional Review Board, and the patient had given written informed consent.
Treatment of the candidate standard (15/174) and commutability samples (S1–S3)
2.4 L of plasma, evaluated above, and three patient samples with SLE coded 15/174, S1, S2 and S3, respectively, were thrombin-treated,7 clarified, 0.5 mL filled into glass ampoules and lyophilised at the National Institute for Biological Standards and Control (NIBSC).7 8 Accelerated stability studies on 15/174 showed a reduction in activity of 0.09%/year at −20°C (online supplementary table S1).9
Supplemental material
Participants and assays used in the international collaborative study
In an international collaborative study (36 laboratories from 17 countries; online supplementary table S2), 15/174 was compared with local standards and S1–S3 to evaluate commutability. Each laboratory is referred to by an arbitrarily assigned number (1–36). For a laboratory performing more than one method, each method is treated as if performed by separate laboratories. A total of 26 different methods were used (table 1). Participants were requested to contribute full dilution comparisons and content estimates of 15/174 with local standards, and assay replicate dilution series in duplicate. Three independent assays were requested, on separate days, with dilutions from freshly reconstituted ampoules.
Supplemental material
Laboratory methods
Study participants were recruited separately to the European and international studies and both were run independently of each other.
Statistical analyses
At NIBSC, estimates in IU/mL at each sample dilution as reported by participants were used directly in the analysis to calculate the potency of 15/174 and S1–S3. A geometric mean (GM) of results corrected for dilution was calculated for each sample in each assay run, excluding dilutions not on a linear section. Parallelism10 ,11 with standards supplied with commercial assay kits was concluded if a linear relationship with a fitted slope between 0.80 and 1.25 was observed for log estimated concentration against log dilution. Outside this range, no calculated estimate relative to kit standard was reported. Where fewer than half of the assays performed by a laboratory gave valid results for a sample, no laboratory mean result is reported for that sample. GM was used to combine results from individual assays of 15/174 and S1–S3 for each laboratory.
Relative potencies for S1–S3 to 15/174 were calculated using a parallel-line model10 with log estimated concentration as assay response. Where the ratio of fitted slopes for the samples was outside 0.80 to 1.25, no relative potency was reported.
Results from all valid assay runs were combined to generate unweighted GMs for each laboratory and used to calculate overall unweighted GM potency estimates. Variability between laboratories has been expressed using geometric coefficients of variation (GCV = {10 s−1}×100% where s is the SD of the log10 transformed estimates). Outliers were defined as results more than (1.5 × IQR) higher than the upper quartile or (1.5 × IQR) lower than the lower quartile.
Patient involvement
There was no patient involvement in this study.
RESULTS
Characterisation of the raw material by 42 European laboratories
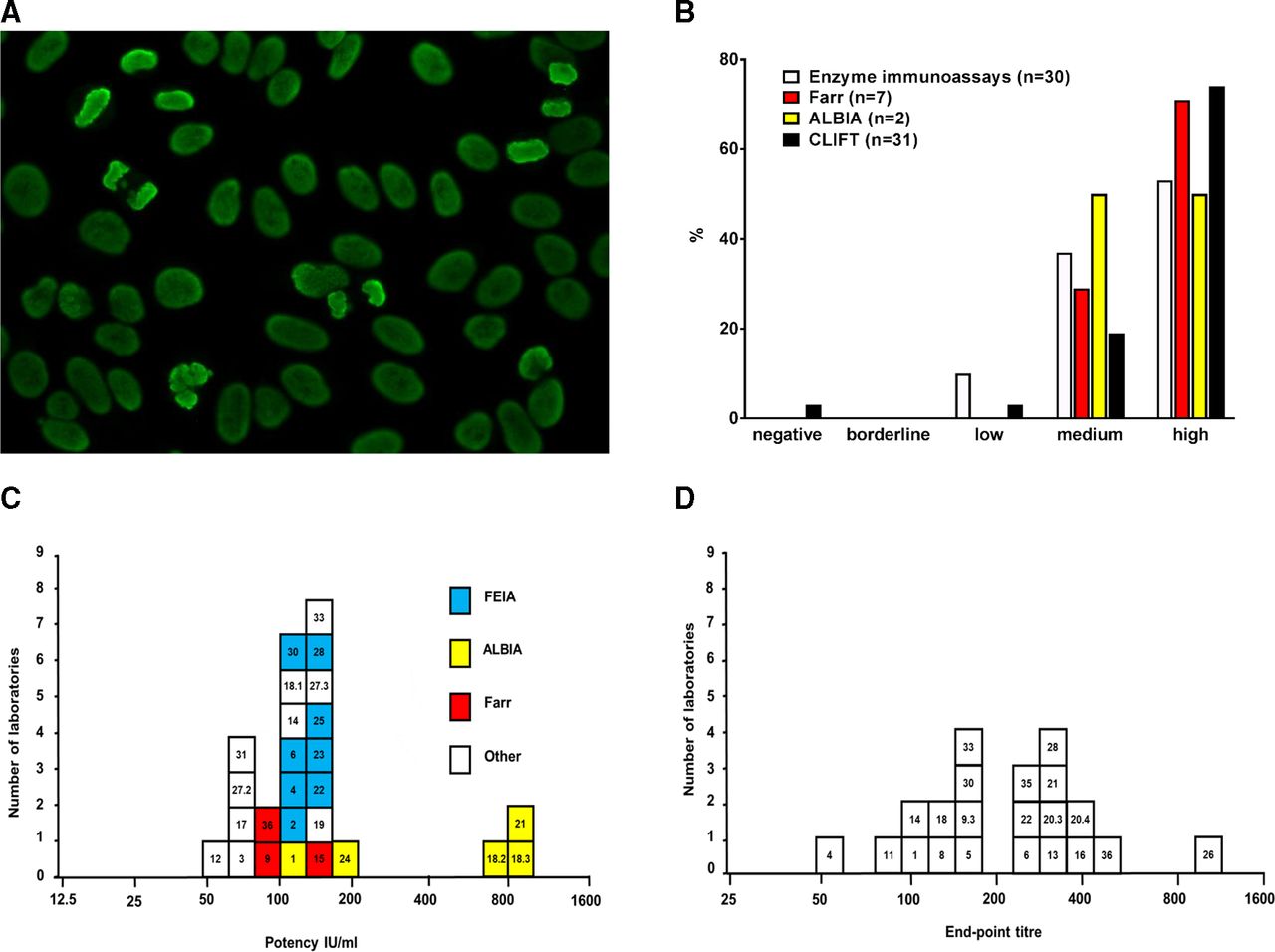
Homogeneous antinuclear antibody or AC-1 pattern was detected in all laboratories (figure 1A).5 All laboratories reported anti-dsDNA (figure 1B). Anti-histone antibodies were reported from 24/25, anti-nucleosome in 18/19 and anti-Ku by 18/18 laboratories. Other autoantibodies were rarely reported (online supplementary table S3).
Supplemental material
{kind=link}
Evaluation of SLE plasma subjected to a European study and anti-dsDNA levels for 15/174 from an international collaborative study. (A) Indirect immune fluorescence staining on HEp-2 cells using the raw material used to prepare 15/174. Photo Dr Stephan Regenass. (B) Distribution of test results for anti-dsDNA levels among the 42 European laboratories in relation to laboratory techniques used. Some laboratories performed more than one type of analysis. Levels were evaluated as negative, borderline, low, medium or high by the laboratories performing the analysis. (C) GM potency estimates (IU/mL) of 15/174 from the international collaborative study for statistically valid immunoassay results. (D) GM endpoint titres of 15/174 from the international collaborative study for the CLIFT. The numbers in the squares denote the laboratory codes. Each square represents the unweighted GM from the laboratory. ALBIA, addressable laser bead immunoassay; CLIFT, Crithidia luciliae immunofluorescent test; dsDNA, double-stranded DNA; ELISA, enzyme-linked immunosorbent assay; FEIA, fluoroenzyme immunoassay; GM, geometric mean; SLE, systemic lupus erythematosus.
Assay validity for the international collaborative study
Individual assay estimates and instances of non-parallelism (with commercial kit standards or 15/174) are shown in online supplementary table S4 (calculated from reported results) and online supplementary table S5 (calculated relative to 15/174 by parallel line analysis). A summary of the extent of non-parallelism is shown in table 2.
Supplemental material
Supplemental material
Overall results for the international collaborative study
Statistically valid estimates for 15/174 in terms of commercial kit standards or for S1–S3 in terms of kit standards or relative to 15/174 tended to be highly variable. Estimates of 15/174 against kit standards, for example, ranged from 56 IU/mL to a high of 847 IU/mL, although most estimates fell in the 100–200 IU/mL range (figure 1C). Similar variability for S1–S3 was also observed (online supplementary figure S1A-J). Endpoint titres for the Crithidia luciliae immunofluorescence test (CLIFT) were also highly variable, ranging from 50 to 1000 for 15/174 (figure 1D and online supplementary figure S2A-C).
Supplemental material
Supplemental material
Intra-laboratory and inter-laboratory variability for the international collaborative study
Calculation of estimates in terms of a common candidate standard invariably produced a reduction in %GCV, most noticeable for CLIFT results when comparing the estimates in terms of absolute titres with those obtained relative to 15/174 (table 2). For quantitative immunoassays, comparing estimates reported in terms of kit standards against those calculated in terms of 15/174 showed reductions in %GCV for S1&S2, but not S3, based on results after exclusion of outliers (table 2).
DISCUSSION
In all laboratories and test methods, 15/174 exhibited anti-dsDNA reactivity. In approximately half of the laboratories, the material behaved in an apparently similar way to local standards, and by inference to the first IS (Wo/80). In a similar number of laboratories, there was observable non-parallelism and no quantitative traceability to Wo/80 could be established. Moreover, across the entire study, it was not possible to establish commutability, as a consistent ranking order for the three patient samples was not obtained. In this context, it is important to mention that anti-dsDNA levels in S1 and S2 were very similar (table 2). It is also of interest to note that laboratories 18.2, 18.3 and 21 used high sensitivity addressable laser bead immunoassay kits and the higher potency results reported were probably due to detection of low affinity antibodies (figure 1C). However, as shown in table 2, alignment to 15/174 reduced variability and minimised batch-to-batch variability of a test kit, rather than obtaining an absolute value, should be considered most important in clinical diagnosis and monitoring disease progression and/or the effect of treatment over time.
The range of available anti-dsDNA assays has increased considerably during the 30 years since Wo/80 was described.4 The 36 laboratories participating in the collaborative study for 15/174 all employed the assays routinely used to quantify anti-dsDNA in their routine clinical settings.8 This setting differs appreciably from the setup employed in the evaluation of Wo/80 when eight laboratories with special expertise in anti-dsDNA testing all obtained identical centrally prepared reagents and then performed CLIFT and Farr assays according to fixed protocols.
The first IS for anti-dsDNA, Wo/80, is exhausted and has been unavailable for more than a decade. Some methods included in this study can provide a historical linkage to the unitage assigned to Wo/80 through earlier calibration exercises, although many cannot, and none can be confirmed due to the unavailability of Wo/80. Thus, the typical replacement paradigm is not applicable when introducing 15/174. Another problem in exchanging autoantibody standards based on patient’s samples is that the candidate replacement is unlikely to be identical to the original. This is particularly significant in the case of anti-dsDNA where autoantibody avidity might differ between patients. SLE sera also contain many different autoantibodies against a range of antigens, including dsDNA. Although 15/174 cannot be regarded as monospecific for anti-dsDNA, we found the raw material for 15/174 to be rather specific for anti-chromatin reactivities and antibodies against Ku, a DNA binding protein.12–14 It is known that different methods may detect different populations of anti-dsDNA3 so there are discrepancies in antibody levels depending on the type of test when applied to individual patients.
Given the presumed different binding characteristics resulting in an apparent lack of comparability of this candidate standard with the previous IS, it is considered that it would be unwise to establish this material as a replacement IS, with a defined unitage in IU. Notwithstanding this discontinuity, this study showed that the field would benefit from the availability of an international reference reagent, and that the current situation, with manifest differences in performance between different assays supposedly measuring the same thing, would be improved. The preparation 15/174 is intended to be used to align test methods quantifying levels of anti-dsDNA to a common standard.
Based on the results presented here, the WHO Expert Committee on Biological Standardisation endorsed preparation 15/174 as the WHO Reference Reagent for lupus (oligo-specific) anti-dsDNA antibodies with a nominal potency of 100 units per ampoule.15 The name intentionally emphasises the non-continuity with the first IS for anti-dsDNA. The Reference Reagent 15/174 is available from the NIBSC (https://www.nibsc.org/products/brm_product_catalogue/detail_page.aspx?catid=15/174).
Acknowledgments
We thank Drs Susan Thorpe and Adrian Bristow for their respective contributions in initiating the WHO project and drafting the WHO report. The study organisers thank Drs Charlotte Dahle and Anders Bengtsson for donating clinical samples, and Dr Stephan Regenass for the permission to use his photo of the HEp-2 staining. We thank the staff of the Centre for Biological Reference Materials, NIBSC, for lyophilising the candidate IS and clinical samples. We are extremely grateful to the study participants for contributing data. Johan Rönnelid is the chairman of the EULAR European Consensus Finding Study Group on Autoantibodies, performing the immunological characterisation of the raw material for 15/174. The preliminary results from this study were presented at the 3rd International Autoantibody Standardization (IAS) Workshop, Dresden.
Footnotes
Handling editor Josef S Smolen
Contributors PLM, JR, CD and BJF evaluated the suitability of the proposed candidate material; JH and PR carried out the statistical analysis; BJF and JR drafted the manuscript, which was critically reviewed and approved by all the authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval was granted by the Institutional Review Board of the Istituto Auxologico Italiano (date: 1-02-2000).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.