Article Text

Statistics from Altmetric.com
Several autoimmune diseases, most notably systemic lupus erythematosus (SLE), show an overexpression of type I interferon (IFN)-inducible genes, termed the IFN signature.1 The IFN signature is associated with endothelial progenitor cells (EPC) dysfunction in SLE2 and the recent report by Grenn et al3 provides evidence for this link in antiphospholipid syndrome (APS) as well.
The authors show that patients with primary APS (PAPS) have a reduced number of circulating EPC that differentiate into endothelial cell like cells. This is supported by a similar reduction in EPC differentiation when EPC from healthy controls (HC) are cultured with serum from patients with PAPS. Whereas depletion of antiphospholipid antibodies (aPL) has no effect, blockade of the receptor for type I IFN restores EPC differentiation. Hence, targeting type I IFN might mitigate vascular disease in patients with APS by restoring EPC differentiation. In support of this assumption, the authors demonstrate the presence of an IFN signature in peripheral blood mononuclear cells (PBMC) of patients with PAPS.
Previous hints in the literature further confirm the presence of an IFN signature in PBMC of patients with PAPS.4 ,5 Interestingly, a microarray study on isolated monocytes of patients with SLE, SLE+APS and PAPS reported the presence of an IFN signature only in monocytes of patients with SLE and SLE+APS, not in PAPS.6 Monocytes are considered key players in the pathogenesis of APS4 among others due to an overexpression of tissue factor (TF), the main initiator of humoral coagulation, while shifts in monocyte subsets are linked to vascular disease in rheumatic diseases.7 ,8
Here we report the prevalence of the IFN signature in monocytes from patients with PAPS, SLE+APS and SLE in relation to TF expression and increases in proinflammatory monocyte subsets and show that patients with PAPS treated with hydroxychloroquine and statins have reduced IFN signatures.
Prevalence of a type I IFN signature in monocytes of patients with APS
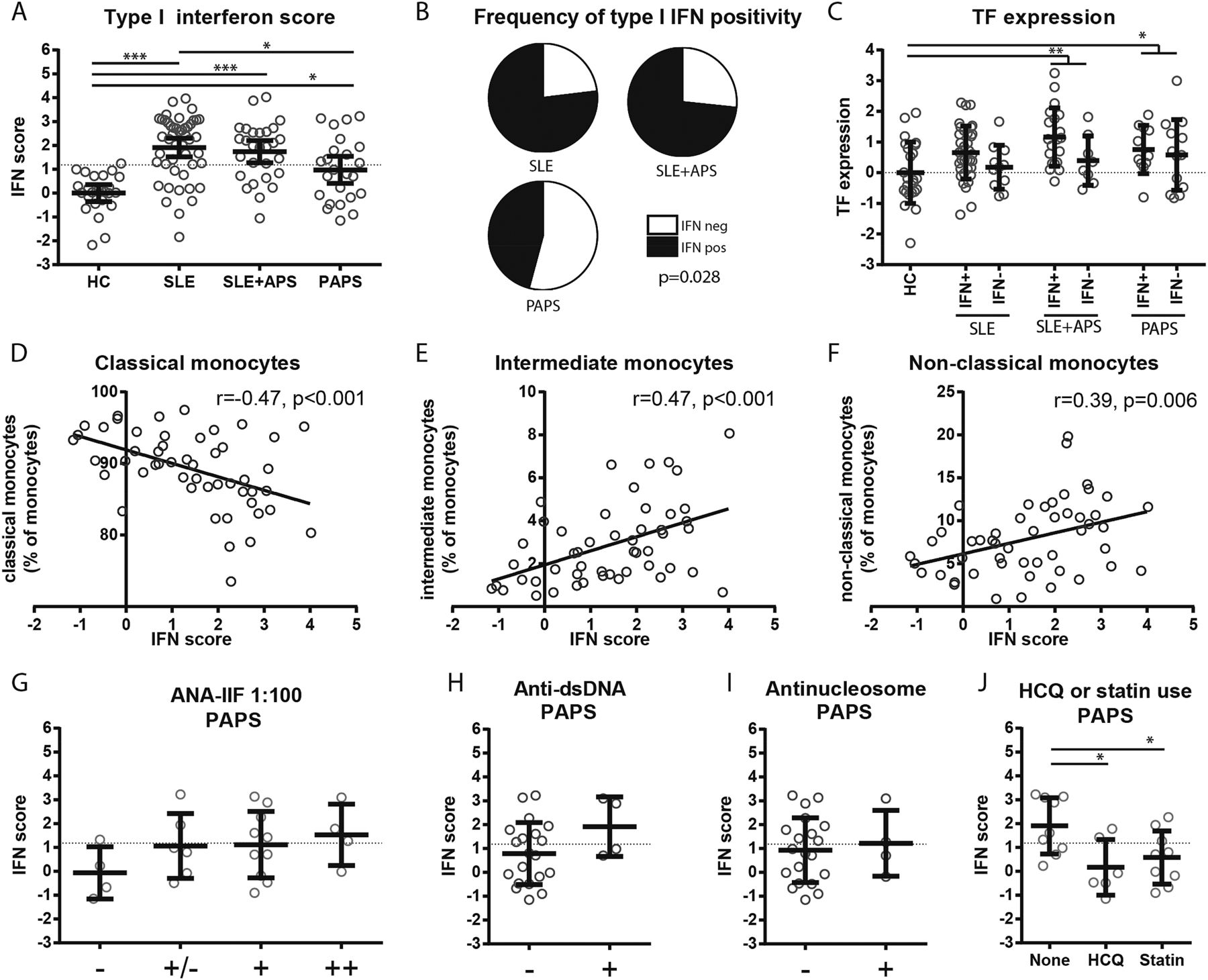
Significantly increased IFN scores were observed in patients with SLE, SLE+APS and PAPS as compared with HC. Interestingly, patients with SLE had higher IFN scores than those with PAPS (figure 1A). Using a cut-off set at the 95th percentile of HC, an IFN signature (IFN+) was observed in 77%, 71% and 46% of patients with SLE, SLE+APS and PAPS, respectively (figure 1B). The previously mentioned microarray study in monocytes of patients with SLE, SLE+APS and PAPS6 used only genes differentially expressed by at least twofold for further pathway analysis. This threshold explains why the IFN signature was not detected in PAPS. A reanalysis of the publicly available dataset (GEO dataset ID 200050395) is in line with our data, showing increased expression of type I IFN inducible genes in monocytes of PAPS patients as compared with HC, with higher expressions in patients with SLE and SLE+APS.

{kind=link}
Prevalence of a type I interferon (IFN) signature in monocytes of patients with systemic lupus erythematosus (SLE), SLE+APS (antiphospholipid syndrome) and primary APS (PAPS) in relation to tissue factor expression, monocyte subsets, lupus-like serology, hydroxychloroquine and statin use. (A) Distribution of type I IFN scores among patients with SLE, SLE+APS and PAPS (means±95% CI). IFN scores were determined as previously described.12 Statistics: Analysis of variance (ANOVA) with post hoc Tukey's HSD. (B) Proportion of patients with or without a type I IFN signature by setting a threshold at the 95th percentile of healthy controls (HC). Statistics: χ2. (C) Tissue factor (TF) expression z-scores in patients when stratified by the presence (IFN+) or absence (IFN−) of a type I IFN signature (means±SD). Statistics: ANOVA with post hoc Dunnett's and Student's t-test (comparison of IFN+ with IFN− subgroups). (D–F) Correlations of the type I IFN score with the proportion of classical, intermediate and non-classical monocytes in patients with APS (SLE+APS and PAPS) as determined by flow cytometry on isolated monocytes. Statistics: Pearson correlation coefficients. (G) Type I IFN scores of patients with PAPS stratified by result of antinuclear antibody (ANA) IIF test (at 1:100 serum dilution). Only ++ samples also tested positive at 1:1000 serum dilution, (H) the presence or absence of anti-dsDNA antibodies (ELiA) or (I) anti-nucleosome antibodies (line blot) (means±SD). Statistics polynominal ANOVA (G) or Student's t-test (H and I). (J) Patients with PAPS stratified by their use of hydroxychloroquine (HCQ) or statins (means±SD). Statistics: ANOVA with post hoc Dunnett's. Each dot represents one subject. *p<0.05, **p<0.01, ***p<0.001. The dotted horizontal line in G–J indicates the 95th percentile of IFN scores in HC as in A. IIF, indirect immunofluorescence; MMF, mycophenolate mofetil.
In our cohort, the IFN score was neither associated with the presence or absence of lupus anticoagulant, anti-cardiolipin, anti-β2 glycoprotein I antibodies or triple positivity nor with the type of thrombosis (arterial or venous), both in patients with PAPS and in SLE+APS (data not shown). Monocytes of patients with SLE+APS and PAPS had increased expression of TF, with a similar trend in patients with SLE. Although TF expression was on average higher in patients with a type I IFN signature (IFN+) as compared with patients without (IFN−), this did not reach statistical significance in any of the patient groups (IFN+ vs IFN− in patients with SLE, SLE+APS and PAPS p=0.10, p=0.055 and p=0.67, respectively) (figure 1C).
Type I IFN signature associates with increases in proinflammatory monocyte subsets in APS
Monocytes can be subdivided into three different subsets based on the expression of CD14 and CD16. The majority of monocytes are CD14++CD16− and termed classical monocytes, whereas CD14++CD16+ and CD14+CD16+ are termed intermediate and non-classical monocytes, respectively. No differences were observed in the proportion of monocyte subsets between patients with SLE+APS and PAPS (data not shown). However, the IFN scores correlated positively with the proportions of intermediate and non-classical monocytes (r=0.47, p<0.001 and r=0.39, p=0.006, respectively) and negatively with the proportion of classical monocytes (r=−0.47, p<0.001) in APS (figure 1D–F). As increases in intermediate and non-classical monocytes are associated with preclinical cardiovascular disease (CVD) in SLE and rheumatoid arthritis7 ,8 this observation further substantiates the link between type I IFN and vascular disease in APS, as was proposed by Grenn et al.
Type I IFN signature in relation to lupus-like serology, hydroxychloroquine and statin use in PAPS
As IFN scores are higher in patients with SLE, it might be speculated that the presence of an IFN signature predisposes patients with PAPS to develop SLE. None of the patients with PAPS studied had clinical evidence of SLE, fulfilled the American College of Rheumatology criteria for SLE or was treated with immunosuppressants (table 1). The presence of lupus-like serology such as antinuclear antibodies (ANA), anti-double stranded DNA (anti-dsDNA) or anti-nucleosome antibodies is associated with the progression of PAPS towards SLE.9 ,10 Insignificant trends towards higher IFN scores were observed in patients with PAPS with higher level of ANA (figure 1G, p=0.12) and with elevated anti-dsDNA antibodies (figure 1H, p=0.12). No relation between anti-nucleosome antibodies and the IFN signature was observed in PAPS (figure 1I p=0.70). Importantly, 45% of the patients with PAPS without anti-dsDNA antibodies had an IFN signature defined as above the 95th percentile of HC (figure 1H). There is a growing interest in the use of hydroxychloroquine and statins as immunomodulators in PAPS.11 Interestingly, patients with PAPS treated with hydroxychloroquine and statins had lower IFN scores as compared with patients not using these drugs (figure 1J).
Patient characteristics
In support of the data by Grenn et al, we conclude that monocytes of patients with PAPS display an IFN signature. However, based on our data we conclude that the IFN signature is more outspoken in patients with SLE. Besides its association with EPC dysfunction, we report that the IFN signature is associated with increases in CVD-associated monocyte subsets and is not restricted to patients with PAPS with lupus-like serology. Finally, hydroxychloroquine and statin treatment might serve to control type I IFN-related immune activation in PAPS.
References
Footnotes
JAGvR and TRDJR shared last co-authorship.
Contributors All authors were involved in study design, interpretation of data, drafting of the work and gave final approval of the version published. LLvdH was involved in data collection and performed the analysis.
Competing interests None declared.
Ethics approval Medisch Ethische Toetsingscommissie Utrecht.
Provenance and peer review Not commissioned; internally peer reviewed.