Article Text

Abstract
Background/purpose Early diagnosis of inflammatory rheumatic diseases is important in order to improve long-term outcome. We studied whether delay in diagnosis (time between onset of symptoms and establishment of diagnosis) in patients with rheumatoid arthritis (RA), psoriatic arthritis (PSA) and ankylosing spondylitis (AS) changed from year 2000 to 2011.
Methods Month and year of initial symptoms and diagnosis, gender, hospital, year of birth and date of first data entry were obtained for 13 721 patients with RA, PSA or AS who had been registered in the DANBIO registry. Time between symptom onset and diagnosis was modelled using generalised linear regression to predict the average duration for each calendar year of initial symptoms with adjustments for gender, year of birth and date of DANBIO entry.
Results Patients with valid data (RA: 10 416 (73%); PSA: 1970 (68%); AS: 1335 (65%)) did not differ significantly from the whole DANBIO population, except more missing data in early years. The regression model showed that the mean duration from initial symptoms to diagnosis for RA, PSA and AS declined steadily from 30, 53 and 66 months (year 2000), respectively, to 3–4 months (year 2011). Sensitivity analyses including patients who were included after 2005, patients who had received biological treatment or had symptom onset less than 2 and 5 years prior to first entry into DANBIO showed similar results.
Conclusion Since the year 2000, a significant reduction in diagnostic delay was observed in this large cohort of patients with RA, PSA or AS, probably reflecting a stronger awareness of the importance of early diagnosis.
- Ankylosing Spondylitis
- Psoriatic Arthritis
- Rheumatoid Arthritis
- Epidemiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA), psoriatic arthritis (PSA) and ankylosing spondylitis (AS) are the most prevalent chronic inflammatory arthritides, causing severe pain, joint destructions, loss of function and comorbidities.1–4 Since the 1990s, scientific evidence has shown that the prognosis for patients with RA improved when they are diagnosed early after symptom onset.5–8 Early diagnosis and aggressive treatment with anti-inflammatory disease-modifying drugs such as methotrexate resulted in reduced progression of joint damage.5–8 The goal of early treatment has so far been difficult to achieve with reports of lag time between symptom onset and diagnosis of 9–17 months.9 ,10 A ‘window of opportunity’ for initiation of treatment of about 3 months after symptom onset in RA has been identified as the optimum time to achieve remission.11 This knowledge is reflected in clinical referral and treatment guidelines across Europe and in the USA, and initiatives have been taken to reduce diagnostic delay, for example, by establishing early arthritis clinics and referral guidelines.12 The principle of early referral has spread to other inflammatory rheumatic diseases, for example, PSA and AS.3 ,13 ,14 Current recommendations for the management of PSA state that early treatment should be given priority.3 In AS, the challenges are even bigger since diagnosing patients has often been delayed by many years.13 ,15–17 Thus, considerable and continuous concern has been expressed by rheumatologists regarding the problem of diagnostic delay in inflammatory arthritis.9 ,12 ,18–20
Despite this, little is known about whether the recommendations of early referral have been transformed into more rapid establishment of diagnosis in routine care. Early referral is difficult to study on a larger scale because in contrast to the date of diagnosis, the date of symptom onset is not registered routinely in patient registration systems.
Based on the nationwide, Danish DANBIO registry, the aim of the present study was to study whether diagnostic delay defined as the time between onset of symptoms and the time of diagnosis has changed since the year 2000 in patients with RA, PSA or AS. We hypothesised that a reduction in diagnostic delay had occurred in this period for all three diagnoses.
Methods
Study design
This was an observational study of patients with RA, PSA or AS who had been registered prospectively in DANBIO between 2000 and 2011. The main variable of interest was the delay in establishing the diagnosis, that is, the time span between onset of symptoms and establishment of diagnosis. We studied changes in delay during the 12-year period.
Data sources and variables
The DANBIO registry was established in 2000 with the primary aim to study drug efficacy and safety.21–25 Rheumatologists from all Danish departments of rheumatology register adult patients (age ≥18 years) with rheumatic disease (ie, RA, AS and PSA) who start any antirheumatic treatment in routine care. Patients are followed prospectively with regular registrations of treatment and disease status.23 From 2000 to 2005, the registration included mainly patients starting treatment with biological disease-modifying antirheumatic drugs (bDMARDs). Coverage is >90% for patients who are treated with bDMARDs.23 Since 2005 patients have been registered in DANBIO regardless of treatment. At the time of inclusion, the treating rheumatologist enters details of the disease history (including month and year of symptom onset and of diagnosis), disease activity and antirheumatic treatment. At the time of the first registration in DANBIO, some patients would have recent-onset arthritis and others established disease.
We obtained information of diagnosis (ICD-10), month/year of initial symptoms, month/year of diagnosis. gender, birth year, hospital, geographical region and date of first entry into the DANBIO registry, disease activity at first entry (assessed by patient's global score on a visual analogue scale ranging from 0 mm (none) to 100 mm (worst possible)), disease severity (assessed by functional status by the Health Assessment Questionnaire (HAQ)) and ever/never treatment with bDMARD.
Study population
The study population included all patients aged ≥18 years at the time of symptom onset who during the period from January 2000 to December 2011 had been registered in the DANBIO registry with a diagnosis of RA, PSA or AS and had valid data on dates of symptom onset and diagnosis.
Potential confounders
As potential confounders were considered demographic variables (birth year, gender, geographical region) and year of first entry into DANBIO. In patients with available data, analyses were repeated with addition of the following variables: disease activity at entry into DANBIO (patient global score), disease severity (estimated by the HAQ at entry into DANBIO) and prescription of bDMARD (ever/never). Since the results of the two analyses were similar, we only present the former in the paper.
Permissions and ethics
The DANBIO database has been approved by the Danish Board of Health and the Danish Data Registry. The registration of data does not require patient consent. Publication of data does not require approval by the ethics committee.
Statistical analyses
Valid dates on symptom onset and diagnosis were available for 13 721 of 19 127 patients (72%). We used t test to ascertain association with invalid dates and gender, birth year, symptom onset, diagnosis, date of data entry and regional health authority. A total of 120 patients with RA, 58 patients with AS and 126 patients with AS who had delay in diagnosis exceeding 240 months were truncated at 240 months in order to reduce variance. For the statistical analysis, birth year was categorised into 10-year age groups (prior to 1929, 1930–1939, …,1980–1989) and one 5-year group from 1990 to 1995. The years of first symptoms and diagnosis were categorised into 3-year periods (prior to 2000, 2000–2002, 2003–2005, 2006–2008, 2009–2011). The majority of data on time of first symptoms and first diagnosis were entered into DANBIO after 2005. Date of first entry into the DANBIO registry was therefore categorised into 3-year periods (prior to 2006, 2006–2008, 2009–2011). Up to 2006 the health service in Denmark was organised in 15 counties. From 2007 they were amalgamated into five health regions, which were used for the present analyses. The study population was compared with the group of other DANBIO patients who were excluded from the analysis due to missing data on onset of symptoms and/or date of diagnosis.
Bivariate analyses were conducted with ordinary least-squares regressions of the delay as the dependent variable and gender, year of birth, initial symptoms and calendar year of DANBIO entry as the explanatory variables. Descriptive analysis of the average duration of the delay in relation to year of birth and initial symptoms and year of birth and hospital region was provided. Kaplan–Meier plots were used to illustrate time from symptom onset to diagnosis by calendar year of initial symptoms.
To analyse the association between average delay of diagnosis and gender, year of birth, year of initial symptoms and year of entry, three different general linear regression models were estimated: one assuming a Poisson distribution, one negative binominal regression model (which is less restrictive than the Poisson model) and finally a model that assumed a γ distribution. The model assuming a γ distribution was chosen as the preferred model because it provided the best fit. This model was then used to predict the average duration for each year of initial symptoms with adjustments for gender, year of birth and DANBIO entry.
Sensitivity analyses were performed including (1) only patients starting biological treatment, (2) only patients included in DANBIO after 2005 regardless of treatment, (3) only patients with recent-onset symptoms defined as maximum 2 years before first registration in DANBIO and (4) only patients with recent or intermediate duration of symptoms, that is, maximum 5 years before first registration.
Statistical analyses were conducted with Stata V.13.0. Statistical significance was assumed for p<0.05.
Results
A total of 10 416 patients with a diagnosis of RA, 1970 patients with PSA and 1335 with AS were registered in DANBIO before 31 December 2011 and had valid dates of symptom onset and diagnosis. Thus, 13 721 patients were included in the present study (table 1). Patients who were included had similar distribution of gender and age as had those who were not included (table 1). Significantly more patients had missing data in the early years of DANBIO registration, especially prior to 2005 (figure 1). When compared with the included patients, the HAQ score and the patient's global score on a visual analogue scale from 0 to 100 mm were higher in the excluded RA and PSA patients, and the fraction who had ever received biological treatment was higher in all three groups (table 1). Characteristics of patients with RA, PSA and AS according to distribution of gender, birth year, year of first symptoms, year of first diagnosis, year of data entry into DANBIO and geographical region are presented in online supplementary table S1.
Clinical characteristics of the study population according to diagnosis and compared with the patients who were not included due to missing date for symptom onset and/or diagnosis
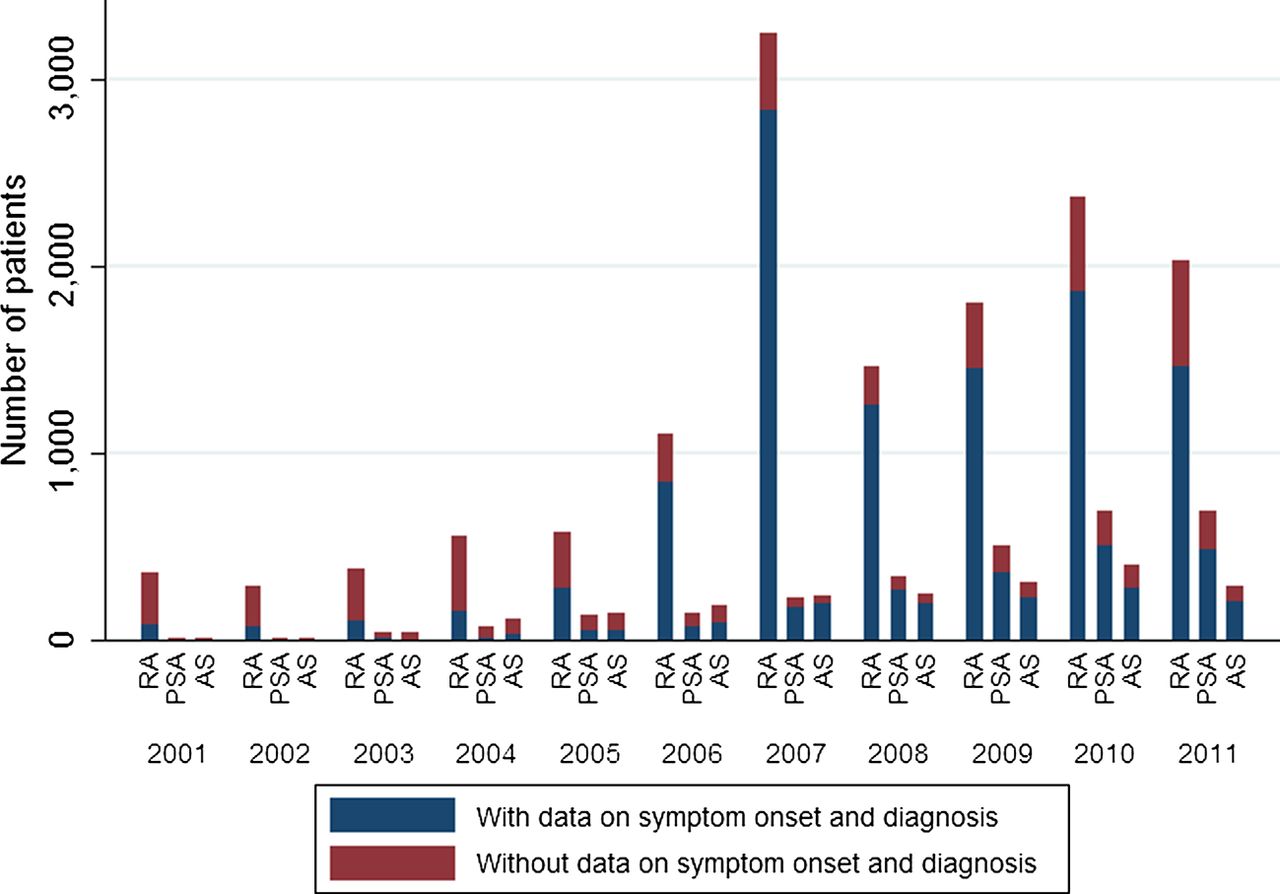
Number of patients with and without data on years for symptom onset and diagnosis shown by year of entry into DANBIO for patients with rheumatoid arthritis, psoriatic arthritis and ankylosing spondylitis.
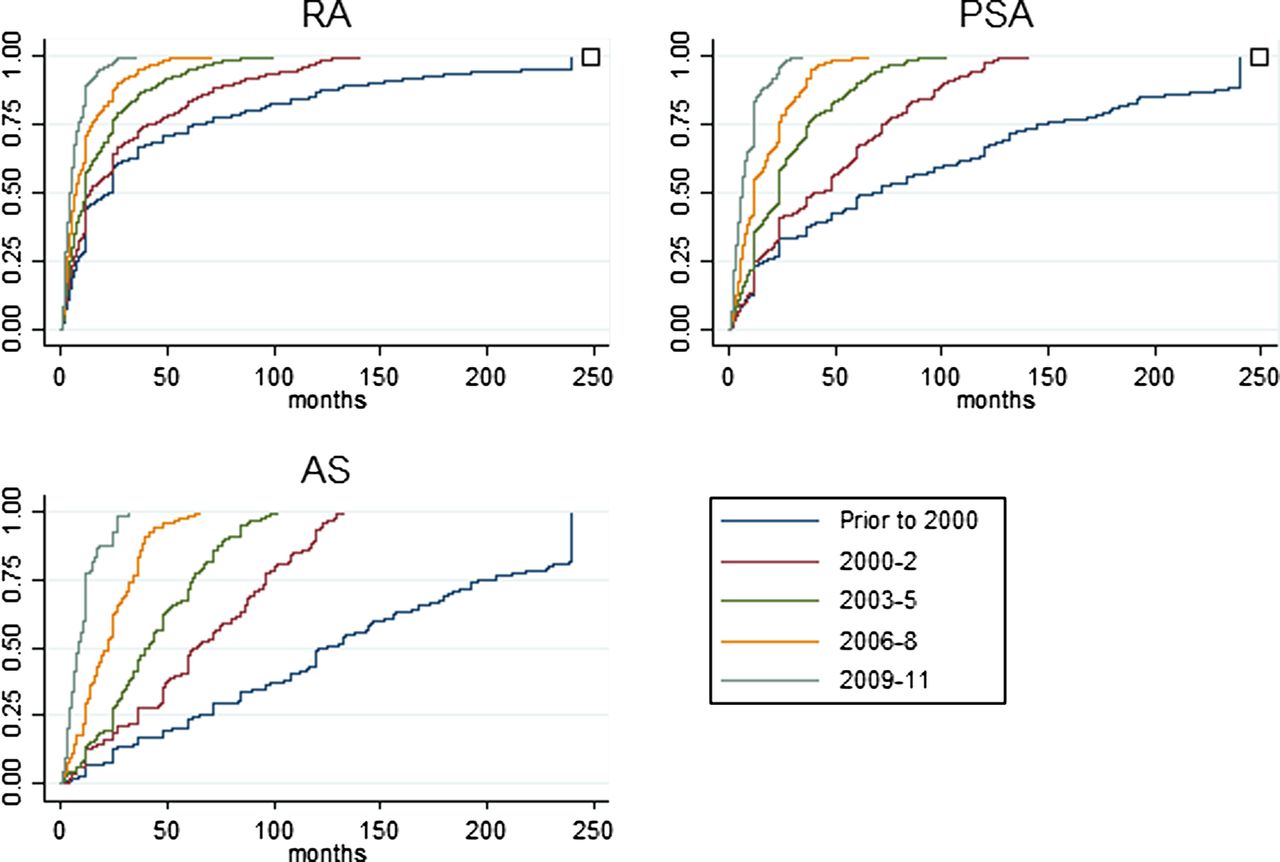
During the study period, the average time from initial symptoms to diagnosis was 23 months (SD=41) for patients with RA, 41 (SD=57) for patients with PSA and 88 (SD=79) for patients with AS. A total of 34% of the RA population, 21% of the PSA and 9% of the AS patients, respectively, had the diagnosis established within 3 months. Figure 2 shows the time from symptom onset to diagnosis by calendar year of initial symptoms. In patients with RA who experienced initial symptoms in 2000–2002, the mean duration until diagnosis was 24 months (median 12) while for those who experienced initial symptoms in 2009–2011 the mean was 6 months (median 4). For patients with PSA, it was 42 (32) and 7 (5), and for patients with AS 64 (61) and 10 (8), respectively.

Time from symptom onset to diagnosis by calendar year of initial symptoms: (A) rheumatoid arthritis, (B) psoriatic arthritis and (C) ankylosing spondylitis.
Figure 3 illustrates the association between year of symptom onset (x-axis), year of birth (z-axis) and duration of diagnostic delay (y-axis) for each disease. Although younger patients had longer diagnostic delay, the calendar year of symptom onset contributed more to delay, that is, patients with more recent symptom onset had shorter diagnostic delay.

Impact of year of symptom onset and birth cohort on time from symptom onset to diagnosis: (A) rheumatoid arthritis, (B) psoriatic arthritis and (C) ankylosing spondylitis
For all three diagnoses, the regression model showed that the calendar year of symptom onset contributed highly significantly and independent of year of birth, year of entry into DANBIO, gender or geographical region to the duration of the diagnostic delay. Year of birth also contributed independently, but only in patients with RA. Gender was only statistically significant in patients with PSA. The year of entry into DANBIO contributed to a lesser extent. Figure 4 shows the modelled duration of diagnostic delay for different years of symptom onset (after adjustment for gender, birth year and year of data entry). The adjusted duration for individuals who had initial symptoms of RA in 2000 was more than 29 months, and the adjusted duration declined each year until the lowest of about 3 months in 2011. For patients with symptoms of PSA and AS, the corresponding delays were 53 and 66 months in 2000 and 3 and 4 months in 2011.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time from symptom onset to diagnosis from the year 2000 to the year 2011 in 10 416 patients with rheumatoid arthritis, psoriatic arthritis and ankylosing spondylitis adjusted for gender, birth year and year of entry into DANBIO.
In four sensitivity analyses, calculations were repeated on subsets of patients, including only patients who had (1) received biological treatment, (2) been registered in DANBIO after 2005 regardless of treatment and (3) less than 2 years and (4) less than 5 years of symptom duration before entry into DANBIO, and the results were similar to those on the whole data set (not shown).
Discussion
Based on the Danish nationwide DANBIO registry, we studied changes in diagnostic delay in the new millennium in more than 13 000 patients with inflammatory rheumatic diseases. A significant and consistent decrease in the time between onset of symptoms and the time of diagnosis was observed between the years 2000 and 2011. For RA, the delay was 29 months in the year 2000, and for PSA and AS it was 53 and 66, respectively. By 2011, the delay was reduced to 3–4 months for all three diseases.
The sample size in this study was an important strength, with data collected prospectively during a 12-years period. Data were captured as part of a prespecified DANBIO protocol.23 The initiative to conduct the investigation came from the Danish Rheumatism Association, who expressed worry about long diagnostic delays in Danish arthritis patients. Data were collected routinely during patients’ visits at the outpatient clinic, but had not been inspected for the present purpose, before analyses began. We consider the internal and external validity and generalisability to be high. However, with an observational design, potential biases must be considered. In the present study, patients with very mild and very severe disease would be less likely to be registered in DANBIO, for example, because specialised treatment was not necessary, or the patient was too ill to register or even died (channelling bias). DANBIO was established in 2000, and patients diagnosed before this time would experience a waiting period before registration was possible and would not be registered unless they survived long enough (immortal time bias or survivor selection bias). Left and right censorship, channelling (leading to selective reporting) and immortal time bias may have resulted in relatively more patients with milder disease being registered during the early years, and more patients with more severe disease during the later years. Other reasons for channelling, with the opposite effect on patient recruitment, may also have been at play: in the early years of DANBIO, registration was restricted to patients who were eligible to biological drugs (ie, the most severely ill patients), whereas after 2005, also patients on non-biological treatments were included. Various sensitivity analyses supported the robustness of the results. In a subanalysis including only patients who had received biological drugs, our key findings were confirmed. This is reassuring since coverage of this group of patients has consistently been >90%, thereby almost eliminating channelling bias.23 Recall bias is another potential source of error: patients with longer disease duration may have difficulties remembering the correct dates for symptom onset. In two sensitivity analyses, we only included patients with symptom onset less than 2 or 5 years prior to first entry into DANBIO, respectively, and found a similar pattern of changes over time in diagnostic delay, indicating that recall bias was not a major issue. This is supported by a previous study that concluded that the majority of patients who were diagnosed with AS remembered the age of first symptoms with an accuracy of less than 1 year.26 As expected in this kind of registration, which takes place in a busy clinical setting, missing data were a weakness with approximately 28% of the patients in the DANBIO registry excluded from the study population. Reassuringly, comparison of the included and excluded patients showed only minor (insignificant) differences in patient characteristics. The number of patients and the completeness of data improved after 2006, when DANBIO switched from paper-based to electronic capture of data. It is likely that the temporal changes observed in this Danish cohort have also resulted in earlier treatment, which is important for the long-term outcome of the diseases, but we do not have data to support this since the date of first disease-modifying treatment is not registered on a routine basis in DANBIO.
Although RA, PSA and AS are the most prevalent chronic inflammatory joint diseases, little is known about the magnitude of diagnostic delay in patients followed in routine care and whether it has changed over the years. Recommendations and guidelines reflect that delay of diagnosis is a major challenge, which needs to be addressed, and strategies promoting early referral and reducing delays in the diagnosis and management of inflammatory arthritis have been launched.3 ,12 ,27 ,28 There is ample evidence in RA that early diagnosis and treatment initiation are associated with improved clinical and radiographic outcomes including the probability of inducing remission.5 ,6 Remission is now the treatment goal in RA, leading to better long-term outcomes, and delays in diagnosis beyond a window of opportunity of 3 months are associated with poorer outcome.5 ,19 ,29 ,30 Significant differences in referral time across Europe have been reported.20 In one study, the median lag time between symptom onset and referral was 17 months,10 and in a cohort of 1674 patients with early RA included between 1993 and 2006, the majority of patients were not seen by a rheumatologist within the 3 months’ window of opportunity.31 Other smaller studies have reported average lag times between 4 and 40 months.9 ,32–34 PSA was previously considered a mild disease, but recent evidence shows that, like RA, PSA causes joint damage, leading to reduced quality of life, impaired function and also increased mortality.18 ,35 The disease develops more severely in patients who present later than 2 years after symptom onset compared with those who present earlier, which suggests that also patients with PSA will benefit from early diagnosis and treatment, although a ‘window of opportunity’ has not been defined.18 ,36 ,37 Current recommendations state that despite relative paucity of randomised controlled trials (RCTs), early treatment should be given priority.3 Most patients with AS have onset of symptoms in their mid-20s, which is the most productive time of life. In the year 2000, the average diagnostic delay in ≈3000 patients with AS was almost 10 years.26 In another study, the average delay was 8 years, but decreasing from 27 years in 1960 to 2 years in 2000.17 In AS, early treatment has not been demonstrated to influence radiographic outcome, but if AS is left undiagnosed, continuous pain, stiffness and fatigue are the consequences alongside a potential progressive loss of spinal mobility and function.13 Early diagnosis is important because patients with AS early in the disease course have at least the same level of disease activity and pain as patients in the later stages. Early diagnosis facilitates early treatment with non-steroidal anti-inflammatory drugs, and if necessary, with tumour necrosis factor blockers, which have the best treatment response in early AS.14 The present study demonstrates how observational registries reflecting clinical practice can contribute with new knowledge about disease course in “real-life” patients because the registries provide data that are neither collected in RCTs nor in administrative health systems. Although clinical practice, resources, etc., vary between countries, it is likely that a reduction in diagnostic delay has been achieved in other countries. Several factors associated with patient behaviour and referral systems contribute to delay of diagnosis. A categorisation of delays has been proposed.38 ,39 where delays are identified at several stages: patients may take time to approach their general practitioner (GP) after they have experienced a swollen joint (patient delay), GPs may attribute the swollen joint to other conditions, for example, overuse, degenerative diseases or gout, causing a further delay (GP delay), and finally the waiting time to specialists in rheumatology may be long (system delay). Strategies for identification and referral of patients with inflammatory arthritis have been launched, including community case finding strategies, public awareness programmes, internet and website information in an attempt to reduce the patient delay, education programmes, self-administered questionnaires and referral guidelines to reduce GP delay, and triage of referrals, rapid access services and early arthritis clinics to reduce system delay.12 Female patients of older age have been reported to suffer more diagnostic delay, and other demographic and socioeconomic factors also have a major impact on patients’ referral to specialist treatment.10 ,31 ,34 In the present study, these factors were also of some significance, but compared with the impact of calendar time, their role was modest. The rheumatologic resources have been fairly constant during the study period. More magnetic resonance scanners have become available. This has improved the access to early diagnosis in patients with axial arthritis and may have contributed to earlier referral in patients with inflammatory back pain. Since it takes years to develop the radiographic changes, which are mandatory in AS according to the modified New York criteria, not all patients have fulfilled those criteria at the time of diagnosis, but rather have been included based on a clinical/MRI-based diagnosis.
In conclusion, in a large cohort of patients with inflammatory arthritis, the delay between symptom onset and establishment of diagnosis decreased significantly from the year 2000 to the year 2011, probably reflecting a stronger awareness of the importance of early diagnosis.
Acknowledgments
All departments of rheumatology in Denmark (Esbjerg, Fredericia, Frederiksberg, Gentofte, Glostrup, Gråsten, Nordsjællands Hospital—Hillerød, Hjørring, Holbæk, Holstebro, Horsens, Kolding, Køge, Odense, Randers, Rigshospitalet, Rønne, Silkeborg, Slagelse, Svendborg, Vejle, Viborg, Aalborg, Aarhus) are acknowledged for conscientiously reporting data to the DANBIO registry.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Handling editor Tore K Kvien
-
Contributors MLH was responsible for collection of data in DANBIO. JS did the statistical analyses of the present study. JS and MLH wrote the manuscript together and both have approved the final version.
-
Funding The study was partly funded by The Danish Rheumatism Association by an unrestricted grant.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.