Article Text

Abstract
Objectives To identify demographic and clinical predictors of obstructive lung disease (OLD) and restrictive lung disease (RLD) in patients with established inflammatory polyarthritis (IP) and to compare the prevalence of respiratory symptoms in patients with IP and the general population.
Method A total of 421 patients with IP underwent a spirometry test 15 years after inclusion in the Norfolk Arthritis Register (NOAR). Logistic regression analyses were performed to assess the predictive ability of demographic and clinical characteristics obtained at inclusion in NOAR and to assess their association with OLD or RLD at 15 years (age- and gender-adjusted). In addition, the prevalence of OLD and RLD was compared with a matched population (1:4) of people participating in the European Prospective Investigation of Cancer-Norfolk, a representative sample of the general population in Norfolk, UK.
Results In this IP population, current smoking was the strongest predictor for OLD and functional disability for RLD. In the comparison study, 11.6% had OLD in the IP population and 4.9% in the general population (adjOR 2.01, 95% CI 1.26 to 3.22). The prevalence of RLD was not statistically different between the IP population and the general population (14.6% vs 17.5%; adjOR 0.76, 95% CI 0.53 to 1.10).
Conclusions OLD, but not RLD, is more prevalent in the IP population than in the general population. Functional disability is especially associated with RLD whereas smoking is associated with OLD. The latter finding, and the known association between smoking and a poor disease prognosis, underlines the importance of smoking cessation in patients with IP.
- Arthritis
- Epidemiology
- Outcomes research
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Respiratory manifestations in rheumatoid arthritis (RA) are common and include upper and lower airway disorders, pleural and interstitial disorders including RA-associated interstitial lung disease (RA-ILD) and are associated with increased mortality.1–7 Common lung disorders can be divided into obstructive lung disease (OLD), including chronic obstructive bronchitis and emphysema, and restrictive lung disease (RLD), including RA-ILD. Especially for RLD, prevalence rates vary widely ranging from 1% to 50%, depending on the diagnostic tests used (eg, pulmonary function tests, high-resolution CT (HRCT)) and the population studied.1 As there is an increased prevalence of smoking in patients with RA, it is perhaps not surprising that there should also be an increased prevalence of chronic obstructive pulmonary disease, lung cancer and respiratory infections compared with the general population. However, even after adjustment for smoking, increased rates of respiratory symptoms have been found in patients with RA compared with the general population.8 ,9
Several demographic and disease severity measures such as male gender, age, smoking, body mass index (BMI), erythrocyte sedimentation rate, rheumatoid factor (RF), anti-citrullinated protein antibody (ACPA) and human leucocyte antigen (HLA)-B40 have been identified as predictors of lung disease in patients with RA,2 ,10–13 although results differ between studies and sample sizes are relatively small. Moreover, most studies were restricted to investigating the prevalence and predictors of either OLD or RLD but not of both. Another disadvantage of previous publications is the cross-sectional study design. For some associations observed, such as between decreased functional disability and OLD or RLD, it is not possible to establish the direction of the association. Therefore, it is also important to determine the association between potential predictors measured prior to the pulmonary function test and subsequent lung function disorders.
The objectives of this study were (1) to identify potential demographic and clinical predictors measured 15 years prior to and potential variables associated with OLD and RLD at time of the spirometry test in patients with inflammatory polyarthritis (IP), and (2) to compare the prevalence of abnormal lung function in patients with IP and the general population.
Methods
Clinical assessments
Consecutive patients aged over 16 years with early IP from the Norfolk Arthritis Register (NOAR) recruited between 1990 and 1994 were included in this study. Details of NOAR have been published previously.14 Briefly, patients with swelling in two or more joints that lasted ≥4 weeks were referred to NOAR. At baseline, patients were seen by a research nurse. Clinical assessments included the evaluation of the number of swollen and tender joints (out of a total of 51). Blood was collected and stored in −80°C freezers to measure RF (positive >40 Ul), ACPA (≥5 U/ml; Axis-Shield DIASTAT Kit, Axis-Shield, Dundee, UK) and C-reactive protein (CRP, mg/l). HLA genotyping was carried out as described previously and subtyping at the HLA-DRB1 locus was performed to identify the presence of the shared epitope.15 The 28-joint Disease Activity Score, based on three components including C-reactive protein (DAS28(3) CRP)16 was calculated for each patient. In addition, patients completed the British version of the Health Assessment Questionnaire (HAQ).17 At each follow-up visit, smoking status was recorded and categorised into never smoked/past smoker/current smoker at baseline and 15-year follow-up. Clinical follow-up assessments were carried out annually for 3 years and then at 5, 7, 10, 12 and 15 years. RA was defined according to the 1987 American College of Rheumatology (ACR) criteria18 and applied cumulatively over these years. At each assessment the use of disease-modifying antirheumatic drugs (DMARDs) and other medication, including medication for respiratory diseases (see online supplemental file), were also recorded. In NOAR, all patients remain under long-term follow-up except for (1) patients who do not cumulatively satisfy the ACR criteria for RA at 5 years and have been given a consultant diagnosis other than RA, undifferentiated IP, psoriatic arthritis or post-viral arthritis to explain their symptoms; (2) patients whose disease has gone into spontaneous long-term remission (no inflamed joints at the 3rd or 5th anniversary and not on DMARDs or steroids).
Respiratory function in patients with IP
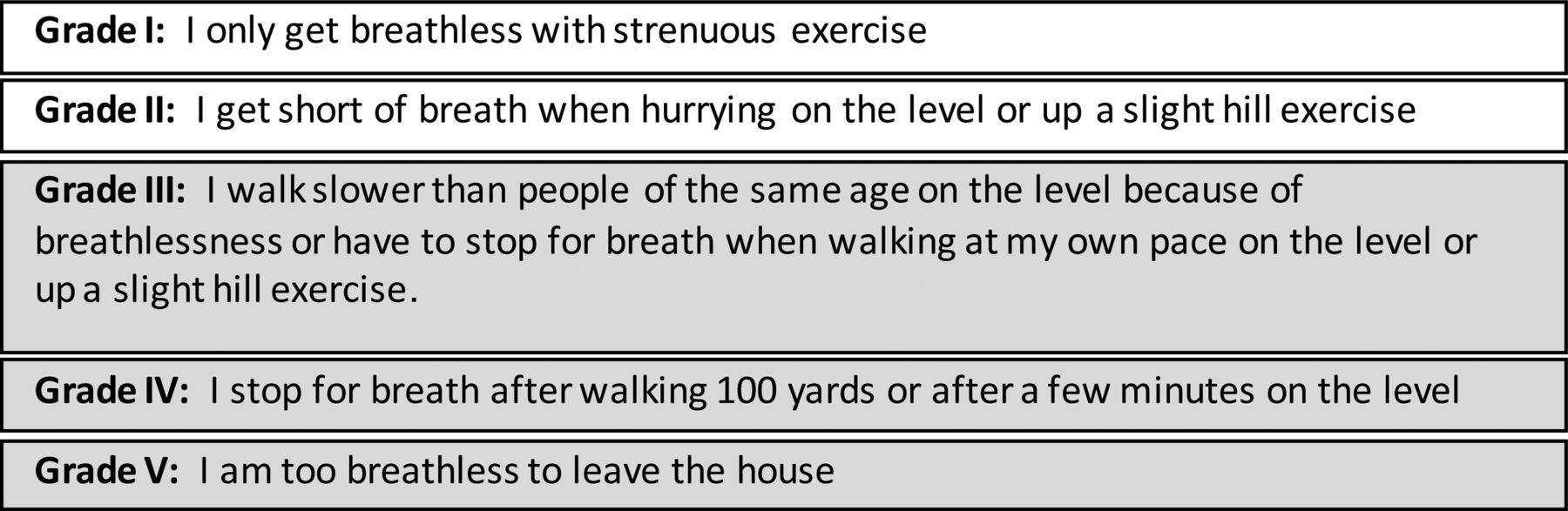
A respiratory function test was performed at the 15-year assessment by a research nurse using a portable spirometer (Micro Medical GP MS07). A standardised protocol was used. Exclusion criteria were patients with angina, undiagnosed chest pains, cardiac problems, recent abdominal or eye surgery or frailty. Forced expiratory volume in 1 s (FEV1), percentage predicted FEV1 (FEV1pred), forced vital capacity (FVC) and percentage predicted FVC (FVCpred) were recorded. OLD was defined according to British Thoracic Society criteria (ie, FEV1/FVC<0.70 and FEV1pred<80%).19 RLD was defined as FVCpred<70% and FEV1/FVC between 0.80 and 1.00. Normal lung function was defined as FVCpred≥70% and FEV1pred≥80%. Patients also completed the Medical Research Council (MRC) respiratory symptom questionnaire.20 ,21 The MRC dyspnoea scale consists of five statements about perceived breathlessness (see figure 1).

{kind=link}
Description grades of MRC respiratory symptom questionnaire.
Patients with MRC grades 3, 4 or 5 were defined as having moderate to severe breathlessness and were compared with patients with MRC grades 1 or 2.
Respiratory function in the general population
Respiratory data collected as part of the European Prospective Investigation of Cancer (EPIC-Norfolk) in Norfolk, UK were used as reference data for the general population.22 ,23 Participants in EPIC-Norfolk are men and women aged 39–79 years at inclusion into the cohort and resident in Norfolk, UK—that is, the same residential area as that of the patients in NOAR. Participants in EPIC-Norfolk were recruited between 1993 and 1997 and follow-up data have been collected at regular intervals. For the present study, data obtained during the second assessment (1998–2000) were used. Participants were asked to complete a questionnaire including questions about any medical conditions, medication use and smoking history (never, past or current). At a clinic visit, height and weight were measured and respiratory function was assessed by spirometry (Micro Medical, Rochester, UK). FEV1 and FVC were measured twice and the higher measure was recorded. Participants in EPIC-Norfolk who were also included in NOAR, were using DMARDs, had a diagnosis of RA, had incomplete respiratory data or missing data on height were excluded from the general population cohort in this study.
Comparison of respiratory function between patients with IP and the general population
Since the age range between patients with IP and the general population sample was slightly different and age is strongly associated with lung function, we included only those people aged between 42 and 81 years at the time the respiratory test was performed. Patients with IP were matched 1–4 with people from the general population by age, gender and season in which the spirometry test was performed. By season and gender, controls were matched using a greedy algorithm to select age matches by selecting the closest match first, within a 5-year age range, then the closest remaining match and so on (STATA, gmatch). FEV1pred and FVCpred were not recorded in EPIC and therefore we estimated the expected FEV1 and FVC for both cohorts to calculate the percentage of predicted value (observed/estimated expected×100%). The estimated expected value was calculated based on the equation from the Health Survey for England.24 The estimated FEV1pred and FVCpred values were strongly correlated with the actual recorded FEV1pred and FVCpred values within the NOAR cohort (FEV1pred: r=0.97, p<0.001; FVCpred: r=0.96, p<0.001).
NOAR and EPIC-Norfolk were approved by the local Norwich Research Ethics Committee and all patients and participants gave written informed consent.
Statistical analysis
In the IP population the predictive ability of baseline demographic and disease-related characteristics and the association between demographic and disease related factors measured at 15 years with OLD or RLD at the 15-year follow-up were assessed using logistic regression models. OR (95% CI) were adjusted for age and gender (adjOR). For the comparison study between patients with IP and the general population, a multinomial regression analysis was performed to test the difference in smoking rates between patients with IP and the general population. A random linear or logistic effect model, where appropriate, retaining the matched groups, was applied to test the difference in FEV1 and FVC between patients with IP and the general population and to test the likelihood for OLD and RLD adjusting for smoking status (adjβ or adjOR). All analyses were repeated in the group of patients fulfilling the 1987 ACR criteria for RA.
All analyses were carried out using STATA Release 11 (StataCorp, College Station, Texas, USA).
Results
A total of 1098 eligible patients were recruited by NOAR between 1990 and 1994; 304 died before the expected 15-year follow-up assessment date, in 12% of which the underlying cause of death was respiratory disease (ICD-10 code J*, see online supplement). In addition, 271 patients were lost to follow-up or were not followed after the 5-year assessment as indicated by the protocol. A total of 523 patients were seen for their 15-year assessment. Of these, 102 patients fulfilled the exclusion criteria or did not want to perform the spirometry test, leaving 421 patients with complete respiratory data included in this study.
At 15 years the mean (SD) age of these 421 patients was 62 (13) years and mean disease duration since symptom onset was 16.0 (1.1) years; 68% were female (table 1) and 79.3% cumulatively fulfilled the 1987 ACR criteria for RA. Disease activity was moderate with a median (IQR) DAS28 score of 3.0 (2.2–3.9) and a median HAQ score of 0.88 (0.25–1.63). Thirty-nine percent of the patients were using non-biological DMARDs and about 6% used a biological agent.
Demographic, clinical characteristics and spirometry values at 15 years
Abnormal lung function test
Mean (SD) FEV1 and FVC were slightly higher for men than for women (2.65 (0.77) l vs 2.10 (0.60) l and 3.39 (0.94) l vs 2.62 (0.73) l, respectively). 6.1% of female patients and 17.1% of male patients satisfied the criteria for OLD and 6.9% of female patients and 24.7% of male patients satisfied the criteria for RLD. Forty-seven of 421 patients (11%) were not categorised as having OLD, RLD or normal lung function. In the total IP population, 12.4% used medication for respiratory symptoms. Of the 419 patients who completed the MRC respiratory questionnaire, 14.1% (14.7% of women and 12.8% of men) reported being breathless (≥grade 3).
Associations with OLD and RLD
Table 2 shows the baseline predictors of abnormal lung function test at 15 years. Age and male gender were predictors of both OLD and RLD in patients with IP. Current smoking at baseline (adjOR 15.25, 95% CI 3.14 to 73.99) and a trend towards previous smoking (adjOR 4.59, 95% CI 0.99 to 21.33) were strong predictors of OLD. DAS28 measured at baseline (adjOR 1.41, 95% CI 1.00 to 1.99) was also a predictor of OLD. No other clinical variables were associated with OLD, whereas RLD was predicted by a high baseline tender joint count (adjOR 1.07, 95% CI 1.02 to 1.12), worse DAS28 score (adjOR 1.44, 95% CI 1.09 to 1.91) and higher HAQ score (adjOR 2.28, 95% CI 1.36 to 3.83). In addition, patients who fulfilled the 1987 criteria for RA (adjOR 2.56, 95% CI 1.24 to 5.29) and patients with nodules (adjOR 4.79, 95% CI 1.46 to 15.71) at baseline were more likely to have RLD 15 years after inclusion in the NOAR cohort. To further test the association between clinical and demographic characteristics measured early in the disease with the development of lung disease, the analyses were repeated excluding patients (n=12) who used drugs for respiratory symptoms at baseline since we did not perform a spirometry test at baseline and thus could not define patients as having OLD or RLD at baseline. DAS28 was no longer a predictor for OLD (p=0.062), probably because of lack of power, whereas all other results remained the same.
Baseline predictors of obstructive and restrictive lung disease
Cross-sectional associations between demographic and clinical variables with OLD and RLD at 15 years are shown in table 3. Age and male gender at the 15-year follow-up were associated with OLD and RLD. Current smoking at 15 years (adjOR 15.91, 95% CI 3.00 to 84.3) and also previous smoking (adjOR 5.90, 95% CI 1.32 to 26.4) were associated with OLD at 15 years. This could probably be explained by the 51 patients who were smoking at baseline and stopped smoking during follow-up. Among all the patients who stopped smoking prior to the 15-year follow-up visit and with available data on time of smoking cessation (n=148), the risk of having OLD reduced with longer cessation time (OR 0.98, 95% CI 0.94 to 1.02) although this was not significant.
Associations of obstructive and restrictive lung disease: cross-sectional analysis at 15 years
Patients with a high DAS28 were more likely to have OLD (adjOR 1.49, 95% CI 1.05 to 2.10) but not RLD (adjOR 1.22, 95% CI 0.83 to 1.80). In contrast, patients with decreased functional ability were more likely to have RLD (adjOR 2.90, 95% CI 1.78 to 4.71) and a trend for OLD (adjOR 1.60, 95% CI 0.96 to 2.66). High BMI (adjOR 1.08, 95% CI 1.00 to 1.16) was associated with RLD and, although not significant, there was a trend towards an association between CRP (adjOR 1.01, 95% CI 1.00 to 1.03), nodules (adjOR 2.22, 95% CI 0.88 to 5.57) and RLD. Use of steroids at the time of the 15-year assessment was associated with RLD, but use of methotrexate did not differ between patients with lung function abnormalities and those without. Restricting the analyses to patients who cumulatively fulfilled the 1987 ACR criteria for RA resulted in similar findings (see online supplementary file tables S1 and S2).
Comparison of abnormal lung function test between patients with IP and the general population
This part of the study included 373 patients with IP and 1492 people from the general population in Norfolk, UK (table 4). The mean (SD) age in both cohorts was 62 (11) years and 68% were women. Patients with IP were more often current smokers (relative risk ratio (RRR) 2.76, 95% CI 1.89 to 4.02) or ex-smokers (RRR 1.97, 95% CI 1.54 to 2.52) than people from the general population. Although a small difference, FEV1 was significantly lower for patients with IP than in the general population (adjβ −0.08, 95% CI −0.13 to −0.02) but FVC was similar between the two populations (adjβ 0.06, 95% CI −0.01 to 0.13) with adjustment for smoking. However, when adjusting for smoking and BMI, patients with IP were less likely to have RLD than the general population (table 4). Thirty-two of 277 patients (11.6%) had OLD in the IP population compared with 55/1124 (4.9%) in the general population (adjOR 2.01, 95% CI 1.26 to 3.22); for women and men these figures were, respectively, 18/197 (9.1%) vs 25/789 (3.2%) (adjOR 2.47, 95% CI 1.29 to 4.71) and 14/80 (17.5%) vs 30/335 (9.0%) (adjOR 1.76, 95% CI 0.87 to 3.58). RLD was observed in 14.6% (42/287) of the IP population and in 17.5% (227/1296) of the general population (adjOR 0.76, 95% CI 0.53 to 1.10). Eleven percent (22/201) women with IP and 13.4% (118/882) women in the general population had RLD (adjOR 0.77, 95% CI 0.47 to 1.28). In men these percentages were 23.3% (20/86) and 26.3% (109/414), respectively (adjOR 0.82, 95% CI 0.47 to 1.43). Overall, patients with IP used medication for respiratory symptoms more often than people from the general population (12.1% vs 2.8%) (OR 4.84, 95% CI 2.91 to 8.06).
Comparison of spirometry data for patients with IP and the general population
Discussion
In this study of patients with established IP, 9.0% had OLD and 11.9% had RLD. The percentage with OLD was higher than in the general population matched for age and gender. We found a strong association between smoking and OLD, an association not observed with RLD. A number of measures of disease severity assessed early in the disease were mainly predictive of RLD after 15 years. However, DAS28 was the only clinical variable associated with OLD in both the longitudinal and the cross-sectional analysis. Nodules, another extra-articular manifestation of RA, were also associated with RLD.
In previous studies inconsistent results have been found between measures of disease activity, demographic factors, smoking and RLD and OLD.2 ,10–13 The findings of our study are supported by prior studies that have identified clinical and other demographic factors in association with either RLD or OLD with respect to HAQ, BMI, male gender and age. However, in contrast to other studies,10 we did not find a significant association between ACPA and RF and lung function abnormalities, but a trend between RF at baseline and OLD and a trend between ACPA at baseline and RLD at 15 years was observed . We did not find an association between smoking and RLD, whereas a strong association between smoking and RA-ILD was found in a previous study defining RA-ILD by means of carbon monoxide transfer factor, FVC<80%pred and perfusion abnormality.12 Smoking, especially current smoking, was strongly associated with OLD, an observation previously observed in both the general population25 ,26 and RA population.10
Only a few other studies have investigated the association between demographic and clinical factors and both OLD and RLD in the same IP/RA cohort. In one study, including 159 patients with RA without cardiovascular disease and with a mean disease duration of 10 years, breathlessness, BMI and prednisone use were predictors of RLD, and chronic cough, prior diagnosis of lung disease, gender, exercise, BMI, current smoking, RF positivity and prednisone use were predictors of OLD in a final multivariate regression model.10 In our study we found an association between breathlessness and OLD, but not with RLD in univariate regression analysis. The MRC respiratory symptom questionnaire used in the present study was developed to detect respiratory symptoms, a surrogate marker of chronic obstructive pulmonary disease (COPD), and thus our results seem valid. The association between oral steroids and abnormal lung function tests found in our study and in the previous study may be a reflection of worse disease activity or because they are prescribed because of their lung disease.
Pulmonary toxicity of methotrexate has been reported in a number of studies27–29 but not in other investigations.30 Since methotrexate is the DMARD of first choice in most countries, we also investigated the association between methotrexate use and lung function test abnormalities in this study. Cross-sectionally, we did not find worse lung function in those patients who used methotrexate in the total population, but a protective effect was found in those with RA. We also analysed the effect of methotrexate use since symptom onset on lung function test abnormalities (data not shown), and again no association was found. This may be due to channelling bias, by which methotrexate treatment is avoided or discontinued in those with respiratory problems. Alternatively, the lack of association could reflect the fact that methotrexate pulmonary toxicity leads to either a severe pneumonitis (in which case the patient may be lost to follow-up) or a self-limiting pneumonitis from which the patient fully recovers when methotrexate is discontinued.
A number of problems arise when comparing results of lung function disorders in RA populations based on spirometry tests, especially RLD between studies. In contrast to OLD for which generally accepted criteria are available (ie, FEV1pred≤80% and FEV1/FVC<0.70), no internationally accepted pulmonary function test criteria exist for RLD. Furthermore, the comparison group varies between studies. In our study, patients with RLD and OLD were compared with patients with normal lung function defined as FVCpred≥70% and FEV1pred≥80% at 15 years. It is, however, possible that some patients with OLD at 15 years had RLD at baseline and vice versa.
The second objective of this study was to compare the prevalence of an abnormal lung function test in patients with IP and the general population in Norfolk, UK. OLD occurred more frequently in patients with IP than in the general population after adjusting for smoking, as previously observed.9 In another study the prevalence of pulmonary function abnormalities was also higher in non-smoking patients with RA compared with the general population.8 Although RA-ILD is the most common form of lung involvement in RA and we did find an association between worse disease and RLD in this study, RLD was not more evident in the IP population than in the general population. Since RLD, once clinically apparent, rather than OLD is especially associated with increased mortality in RA,1 ,2 it is possible that those patients with the most severe RLD did not survive to the 15-year follow-up (see online supplemental file for a description of underlying causes of death) or were no longer participating in the study.
This study has some limitations. RLD was not confirmed by any other test such as HRCT.31 ,32 The findings regarding the comparison of an abnormal lung function test between the IP population and the general population should particularly be interpreted with caution. The protocol used to assess FEV1 and FVC differed between the two cohorts. In order to define patients with OLD and RLD we had to estimate the expected FEV1 and FVC based on equations derived from the English population. Although the estimated and actual reading of both FEV1pred and FVCpred were strongly correlated, it is known that the prevalence of COPD may vary between areas in the UK.33 The difference in the obtained FEV1 value was small but statistically significant and the difference in the percentage of patients with OLD between the two populations was relatively large. A slight change in the value may already define whether or not a person has OLD or RLD. This was noticeable when a few patients with IP who were identified as having OLD based on the actual measurement no longer had OLD when the FEV1pred was calculated again for the comparison study, although a strong correlation existed between the obtained FEV1pred and the calculated FEV1pred. Clinically, it is therefore important to perform other diagnostic tests as well. Another limitation is that those patients with IP with, for example, cardiovascular diseases or who were frail were excluded from this study whereas no exclusion criteria were applied in the EPIC cohort. This may have led to an underestimate of the true difference in abnormal lung function tests between the IP population and the general population because of the increased likelihood of abnormal lung function tests in people with these comorbidities.
In conclusion, OLD (but not RLD) is more prevalent in an established IP population than in the general population. Functional disability is especially associated with RLD whereas smoking is associated with OLD. The latter finding and the known association between smoking and a poor disease prognosis—and the better prognosis in those who stopped—strengthens the importance of smoking cessation in patients with inflammatory arthritis.
Acknowledgments
We would like to acknowledge the contribution of the local general practitioners and rheumatologists in Norwich in referring patients to the register, the NOAR metrologists in the collection of the clinical data and the database management team in Manchester.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Handling editor Tore K Kvien ▸ Additional data are published online only. To view this file please visit the journal online (http://dx.doi.org/10.1136/annrheumdis-2012-201698).
-
Contributors All authors contributed to the design of the study, interpretation of the results and approval of final version of the manuscript.
-
Funding NOAR is funded by Arthritis Research UK (grant reference 17552).
-
Competing interests None.
-
Ethics approval Ethics approval was obtained from the Norwich local research ethics committee, UK.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/