Article Text

Abstract
Background We aimed to describe the uptake of newer biologic or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) in psoriatic arthritis (PsA) in the Nordic countries and to compare their retention and effectiveness.
Methods Patients with PsA starting a b/tsDMARD in 2012–2020 in five Nordic rheumatology registers were included. Uptake and patient characteristics were described, with comorbidities identified from linkages to national patient registries. One-year retention and 6-month effectiveness (proportions achieving low disease activity (LDA) on the Disease Activity Index for PSoriatic Arthritis based on 28-joint evaluation) for the newer b/tsDMARDs (abatacept/apremilast/ixekizumab/secukinumab/tofacitinib/ustekinumab) were compared with adalimumab through adjusted regression models stratified by treatment course (first, second/third, and fourth or more).
Results In total, 5659 treatment courses with adalimumab (56% biologic-naïve) and 4767 courses with a newer b/tsDMARD (21% biologic-naïve) were included. The uptake of newer b/tsDMARDs increased from 2014 and plateaued in 2018. Patient characteristics appeared similar across treatments at treatment start. Adalimumab was more often used as the first course and newer b/tsDMARDs more often in biologic-experienced patients. Used as a second/third b/tsDMARD, the retention rate and the proportion achieving LDA were significantly better for adalimumab (rate 65%, proportion 59%) compared with abatacept (45%, 37%), apremilast (43%, 35%), ixekizumab (LDA only, 40%) and ustekinumab (LDA only, 40%), but not significantly different from other b/tsDMARDs.
Conclusion Uptake of newer b/tsDMARDs occurred mainly in biologic-experienced patients. Regardless of mode of action, only a minority of patients starting a second or later b/tsDMARD course remained on drug and achieved LDA. Superior outcomes for adalimumab indicate that the positioning of newer b/tsDMARDs in the PsA treatment algorithm remains to be established.
- biological therapy
- epidemiology
- spondylitis, ankylosing
- tumor necrosis factor inhibitors
Data availability statement
Due to privacy and ethical concerns any raw data can not be shared. Aggregated data can be shared upon reasonable request
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The increasing number of biologic and targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) available in psoriatic arthritis (PsA) warrants investigation of their effectiveness to establish optimal treatment strategies.
WHAT THIS STUDY ADDS
Uptake of newer b/tsDMARDs was fast in Nordic routine care, mainly in biologic-experienced patients.
Inferior outcomes for certain newer b/tsDMARDs versus adalimumab highlight unestablished position in the PsA treatment algorithm.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The overall low remission rates across treatments in biologic-experienced patients pinpoint the need for additional treatment alternatives, including non-pharmacologic interventions.
Introduction
The treatment landscape in psoriatic arthritis (PsA) is widening, with an increasing number of biologic and targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs), with different modes of action, becoming available.1 2 However, the most effective treatment strategy in routine care, overall and by line of therapy, remains to be established.3
So far, comparative intervention studies in PsA across different modes of action have only been performed for adalimumab versus interleukin 17 inhibitors (IL-17i) and for adalimumab versus the janus kinase inhibitor (JAKi) upadacitinib.4–6 In two head-to-head trials, the IL-17is secukinumab and ixekizumab were respectively compared with adalimumab, with both studies suggesting equivalent effect of IL-17i and tumour necrosis factor inhibitors (TNFi) on arthritis, enthesitis and dactylitis, but better effect of IL-17i on skin psoriasis.4 5 In a randomised controlled trial (RCT) for upadacitinib versus adalimumab, the currently approved dose for upadacitinib (15 mg daily) also showed a similar effect on arthritis as adalimumab, while the higher dose of 30 mg daily was superior.6 One RCT of the JAKi tofacitinib in PsA also included adalimumab as an active comparator, suggesting numerically similar effect sizes.7 Further, a substantial number of observational studies have attempted comparisons of effectiveness in routine care across several different drug classes.8–15 Within the Nordic countries, we have previously shown similar treatment retention and 6-month response in patients with PsA treated with secukinumab and adalimumab.16
In the absence of other intervention studies informing on comparative effectiveness of the different drug classes used in PsA, a number of meta-analyses have aimed at pooling data from RCTs, with the objective of either comparing or ranking efficacy.17–25 The results of these studies are not consistent, but several arrive at the conclusion that TNFi (infliximab, adalimumab and etanercept) and secukinumab may outperform apremilast, abatacept, ustekinumab and tofacitinib (and possibly ixekizumab) in terms of American College of Rheumatology (ACR) response rates,17–23 although others report no significant differences between abatacept, secukinumab, ustekinumab and apremilast.24 25 With these results in mind—and knowing that patients with PsA included in RCTs are not necessarily representative of patients with PsA in a clinical setting26—it seems unlikely that further meta-analyses will provide a definitive answer as to how the different drugs should be positioned in the clinical treatment algorithm for PsA.
From an evidence-based perspective, it is not surprising that the 2019 EULAR (European Alliance of Associations for Rheumatology) recommendations adopted a cautious approach and refrained from ranking the TNFi, IL-17i or IL-12/23 inhibitors,27 whereas abatacept, JAKi and apremilast were placed later in the treatment algorithm. For JAKi (at that time tofacitinib), the reason for this was a poorer effect on psoriasis, safety signals regarding adverse effects and less robust long-term data compared with the other treatment options. For apremilast and abatacept, use was only recommended in special cases, primarily due to lower efficacy in indirect comparisons.27 Information on how to choose mode of action when treating an individual patient with PsA is thus still needed.
The aims of this study were to describe the uptake of newer, non-TNFi b/tsDMARDs (abatacept, apremilast, ixekizumab, secukinumab, tofacitinib and ustekinumab) in the Nordic countries and to directly compare treatment retention and response to these drugs with that of adalimumab. We used adalimumab as the comparator drug to facilitate comparison with the above-mentioned prior active comparator RCTs and head-to-head trials.
Methods
Study design
This is an observational study of patients with PsA based on data collected prospectively in rheumatology registries and other healthcare registers of the Nordic countries.
Data sources
Information on treatment courses with b/tsDMARDs and on disease activity was collected from the rheumatology registers of the five Nordic countries: Denmark (register: DANBIO), Finland (ROB-FIN), Iceland (ICE-BIO), Norway (NOR-DMARD) and Sweden (SRQ). Data from these registers were then enriched by linkage to other national registers to identify previous comorbidities and infections (treated in either inpatient or outpatient specialised care).
Case definition and exposures
All patients with a diagnosis of PsA (as registered in the rheumatology registry according to the treating physician) who started any approved b/tsDMARD between January 2012 and December 2020 (study period) were included. Each patient could contribute with several b/tsDMARD treatment courses. The start of the study period was set at 2012 because ustekinumab was approved for use in Europe in 2013. Registered interruptions in treatment of less than 3 months were disregarded and thus considered as ongoing treatment, as were switching between originator TNFi and their biosimilars.
Each registry extracted data on disease activity during the first year of treatment for each b/tsDMARD treatment course. Baseline data were captured within the time window −30 to +14 days from treatment initiation, and the 6-month follow-up visit from within 90 to 270 days thereafter. In case more than one visit occurred within a given time window, the one closest to the intended time point was selected.
Patients who had failed at least one TNFi due to inefficacy were identified based on information on previous treatment courses and reasons for treatment stop.
Patient characteristics
Patient characteristics at the start of an individual b/tsDMARD (baseline) were retrieved from the rheumatology registries and included gender, age, disease duration, disease activity, number of previous b/tsDMARD treatments and concomitant treatment with conventional synthetic (cs) DMARDs.
Disease activity was reported as C reactive protein (CRP, mg/L), patients’ global health score on Visual Analogue Scale (VAS, 0–100 mm), patients’ pain VAS score, Disease Activity Score based on 28-joint evaluation and Disease Activity Index for PSoriatic Arthritis based on 28-joint evaluation (DAPSA28).28
Extra-musculoskeletal manifestations included previous uveitis and inflammatory bowel disease. Comorbidity score was calculated by summing up the number of different comorbidities registered 0–5 years prior to baseline, indicating overall comorbidity burden. Definitions are presented in online supplemental table S1. Not all countries were able to deliver comorbidity linkage data for the full observation period (Denmark until August 2018, Finland until December 2018, and Sweden, Iceland and Norway for the whole study period).
Supplemental material
Outcomes
Uptake of newer b/tsDMARDs
Newer b/tsDMARDs were defined as abatacept, apremilast, guselkumab, ixekizumab, secukinumab, tofacitinib, upadacitinib and ustekinumab. Uptake and treatment patterns were described by numbers and baseline characteristics of patients starting each drug.
Due to the few registered treatment starts for guselkumab and upadacitinib during the study period (n<10, respectively), further details for these drugs are not provided.
Treatment retention
The 1-year treatment retention was defined as the proportion remaining on the respective b/tsDMARD after 1 year. Censoring occurred at death or end of follow-up (defined for Sweden as 16 March 2022, for Denmark 31 December 2021, for Norway 11 May 2021, for Iceland 30 November 2021 and for Finland generally 15 March 2021, although a few Finnish centres had shorter follow-up).
Treatment response
Treatment response at 6 months after treatment start was described as the proportion achieving DAPSA28 low disease activity (LDA, ≤14) in patients remaining on treatment, with proportions achieving DAPSA28 remission (≤4) reported separately.28 To simulate intention-to-treat analyses, the LDA and remission rates were moreover LUNDEX-corrected, thus incorporating the proportion still on treatment.29
For treatment retention and response, results and comparisons for treatment starts in <100 patients are not shown.
Statistics
Statistical analyses were performed in SAS V.9.4, while graphs were produced with Stata V.14 and Excel. Data from all countries were pooled for combined analyses. Because the newer b/tsDMARDs were expected to be used to a larger extent in patients previously treated with TNFi (opening for confounding by indication), all analyses were performed separately for the first b/tsDMARD course, second or third course, and fourth course or more.
Uptake
Patient characteristics on start of individual b/tsDMARDs are reported as percentages or means with SDs, as appropriate. Graphical presentations of the uptake over time are presented.
Retention
One-year retention was visualised through Kaplan-Meier analyses. Crude and adjusted HRs for discontinuation, using adalimumab as reference, were estimated through Cox regression analyses. Baseline adjustment factors were decided a priori and included age (and its quadratic term), sex, disease duration (categorised according to quartiles), concomitant csDMARD use (yes/no), CRP (quartiles), patient’s global health (quartiles), start year (2012–2014, 2015–2017, 2018–2020), comorbidity score (0, 1, 2+) and history of infections in the previous 5 years (yes/no). For the second/third course, the exact treatment course (second or third) was added as adjustment factor. Country was added in the model as a stratification term by adding a strata statement in the SAS procedure. The assumption of proportional hazards was tested through Schoenfeld’s residuals.
Response
Logistic regression was used to estimate the OR of attaining remission and LDA, adjusted for the same covariates as mentioned for Cox regression above, with adalimumab as reference, among patients with at least 6 months of follow-up.
Missing data
Multiple imputation with the fully conditional specification method was performed to account for missing baseline data, with 25 imputed data sets.30 Two sets of imputed data sets were created: in the retention analyses, only the covariates CRP and patient’s global health were imputed, while in the response analyses the outcome was also imputed. All variables included in the Cox and logistic models were also included in the respective imputations. Therefore, the crude proportions of patients achieving LDA and remission are presented as the mean and range (minimum–maximum) of the values across imputations.
Throughout, comparative analyses across drugs were only performed if there were at least 100 patients in each treatment group, and for the Cox regression also at least 10 outcome events.
Sensitivity analyses
As a complement to the comparative analyses performed on the imputed data sets, complete case analyses were also performed for the logistic models. Further, the regression analyses were repeated for the subset of patients who had previously failed at least one TNFi due to inefficacy. Also, inverse probability of treatment-weighted (IPTW) Cox regression and logistic model were estimated as alternative ways to account for the confounding factors.
Patient and public involvement
Patient representatives were involved in the upstart and planning of this Nordic collaboration across registries, but no patients participated in the design of this specific study.
Results
Treatment uptake and patient characteristics
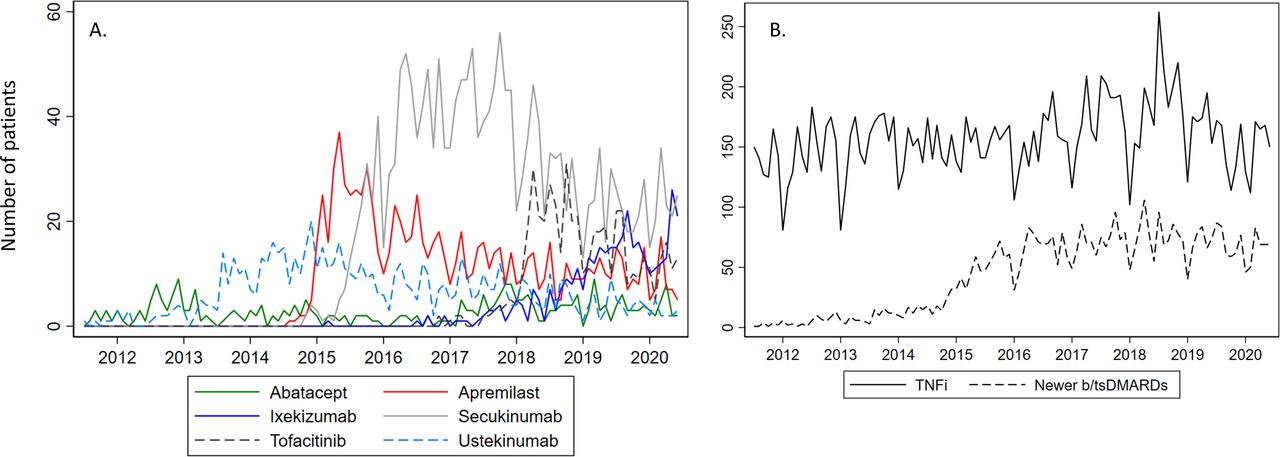
In total, 12 792 patients with PsA were identified, contributing 16 976 treatment courses with any TNFi (whereof 5659 were adalimumab, which was used as comparator drug) and 4767 courses with a newer b/tsDMARD in 2012–2020 (table 1). Country-specific distributions are shown in online supplemental table S2. Fi gure 1A presents the uptake of newer b/tsDMARDs as the number of new starts per month, and figure 1B the number of new starts of all TNFis versus the newer b/tsDMARDs combined (in both figures irrespective of treatment course).

Number of b/tsDMARD treatment starts per month in 2012–2020. (A) Number of newer b/tsDMARD starts. (B) Number of combined TNFi and combined newer b/tsDMARDs. TNFi includes adalimumab, certolizumab pegol, etanercept, golimumab and infliximab. b/tsDMARDs, biologic and targeted synthetic disease-modifying antirheumatic drugs; TNFi, tumour necrosis factor inhibitor.
Baseline characteristics of patients starting any TNFi, adalimumab or a newer b/tsDMARD, presented by course of b/tsDMARD treatment
Overall, there was a rapid increase in the number of patients starting a newer b/tsDMARD from 2014 and onwards, plateauing in 2018, while the number of TNFi new starts remained unchanged over the period. The increased use of newer b/tsDMARDs was initially driven by ustekinumab, followed by apremilast, secukinumab, tofacitinib and ixekizumab, as they became available for use. Throughout there were steady low rates of abatacept starts. During the last 3 months of the study period, there were on average 161 new TNFi starts per month, 43 IL-17i (approximately equal numbers of secukinumab and ixekizumab), 13 tofacitinib, and <10 for apremilast, abatacept and ustekinumab.
The baseline characteristics of patients treated with any TNFi, adalimumab and the newer b/tsDMARDs are shown in table 1, with additional data on comorbidities and distribution across countries in online supplemental table S2 and the proportion of missing data in online supplemental table S3.
During the study period, 10% of the first course of b/tsDMARDs were newer b/tsDMARDs, and for the second/third course and for the fourth course or more these percentages were 25% and 53%, respectively. For first course treatments, apremilast was the most frequently used newer b/tsDMARD, mainly in Swedish and to some extent Finnish patients (table 1). Second/third course newer b/tsDMARDs were mainly secukinumab, but also ustekinumab and apremilast, again mainly in Swedish patients. For the fourth course or more, a similar pattern was seen (as in second/third course), but with tofacitinib also used. For all treatment courses, use of newer b/tsDMARDs other than secukinumab was minimal in Norway and Iceland.
Baseline characteristics (demographics, disease activity, previous comorbidities) appeared largely similar across treatments for all treatment courses (table 1). Differences were mainly observed in the first course b/tsDMARDs, which might be explained by relatively low numbers for some treatments. For extra-musculoskeletal manifestations, the numbers were low, but previous uveitis seemed slightly more prevalent for adalimumab.
Among patients starting a second b/tsDMARD course, 32% of newer b/tsDMARD treatment initiators (n=995) had previously failed adalimumab (data available for 82% of patients), while for the third course the corresponding figure was 52%.
Treatment retention
For first course treatments, the crude 1-year retention rates across b/tsDMARDs ranged from 58% to 83% (not evaluated for abatacept, ixekizumab and tofacitinib due to few treatment starts), for the second/third course from 43% to 68%, and for the fourth course or more from 35% to 65% (figure 2). The crude 1-year retention was poorer for abatacept and apremilast, compared with adalimumab, in all assessed treatment cohorts, and in the fourth course or more this was also seen for ustekinumab.

Retention rate and treatment discontinuation at 1-year follow-up. Results of multivariable Cox regression analyses presented by b/tsDMARD treatment course. *HR not estimated for groups with <100 patients. The error bars for retention and HR represent 95% CI. HRs were adjusted for age (and the quadratic term), sex, disease duration, csDMARD use, C reactive protein, patient’s global health score, treatment start year, comorbidity score and previous infection. ABT, abatacept; ADA, adalimumab; APR, apremilast; b/tsDMARDs, biologic and targeted synthetic disease-modifying antirheumatic drugs; csDMARD, conventional synthetic disease-modifying antirheumatic drug; IXE, ixekizumab; SEC, secukinumab; TOF, tofacitinib; UST, ustekinumab.
The adjusted HRs for discontinuation confirmed this pattern, although when used as first course b/tsDMARD ustekinumab moreover had a significantly lower hazard of discontinuation compared with adalimumab. The assumption of proportional hazards was valid in the model for first course treatments, but not in the other two models (violated by abatacept, secukinumab and ustekinumab). The crude Kaplan-Meier curves and the Cox models split at 6 months of follow-up (to handle the non-proportionality) are presented in online supplemental figure S1 and online supplemental table S4. These analyses suggested higher risk of discontinuation for abatacept and ustekinumab in the 6-month to 12-month period, as compared with adalimumab, although not statistically significant.
Treatment response
Of the 10 426 compared treatment courses (adalimumab or newer b/tsDMARD), 10 388 had at least 6 months of follow-up and could be included in the response analyses.
Figure 3 shows the percentages achieving DAPSA28 LDA or remission, together with the corresponding LUNDEX-corrected proportions, presented by course of treatment. Adalimumab had a higher proportion achieving LDA and remission across all treatment courses, compared with abatacept, apremilast and ustekinumab.

{kind=link}
{kind=link}
{kind=link}
Proportion of patients achieving DAPSA28 LDA (≤14) or remission (≤4) at 6 months, crude and LUNDEX-corrected, presented by treatment course. Results including imputation of missing data; vertical lines illustrate range (minimum–maximum) across the 25 imputations. Not estimated for groups with <100 patients (not available (NA)). ABT, abatacept; ADA, adalimumab; APR, apremilast; DAPSA28, Disease Activity index for PSoriatic Arthritis based on 28-joint evaluation; IXE, ixekizumab; LDA, low disease activity; SEC, secukinumab; TOF, tofacitinib; UST, ustekinumab.
The adjusted ORs for achieving LDA and remission are presented in table 2. For abatacept, apremilast and ustekinumab, the odds of achieving LDA were lower than for adalimumab in all analysed treatment cohorts (could not be calculated for the first course abatacept due to too few treated patients), and for ixekizumab also in the second/third cohort and the fourth or more cohort. For secukinumab and tofacitinib, no statistically significant differences versus adalimumab were found in the achievement of LDA.
DAPSA28 LDA (≤14) or remission (≤4) at 6 months with OR and presented by treatment course: results of multivariable logistic regression analyses
Sensitivity analyses
A comparison of the proportion of patients achieving LDA and remission in the imputed data and in the complete case analyses (online supplemental figure S2) showed similar results. The corresponding complete case analyses are shown in online supplemental table S5.
In the subset of patients who had previously failed at least one TNFi due to inefficacy, we found similar estimates for risk of discontinuation (Cox regression analyses) and treatment response (logistic regression) as in the main analyses (online supplemental table S6).
Using an IPTW approach to adjust for confounding factors resulted in similar estimates as the main analyses (table 2 and online supplemental table S4), with the exception of the HR for discontinuation not indicating superiority for ustekinumab compared with adalimumab when used as the first course, and suggesting higher discontinuation for tofacitinib than adalimumab when used as the fourth course or more.
Discussion
In this study of patients with PsA from five Nordic countries, the number of new starts of any TNFi and the uptake of newer b/tsDMARDs levelled out from 2018, and the newer b/tsDMARDs were mainly used in b/tsDMARD-experienced patients. Our results showed differences in outcomes across the treatment options, where abatacept and apremilast seemed to have inferior effectiveness compared with adalimumab, while ixekizumab, secukinumab and tofacitinib performed similar to adalimumab, and ustekinumab somewhere in between. Similar results were found in the subgroup of patients who previously failed a TNFi due to inefficacy. Based on the LUNDEX-corrected rates, the numbers needed to treat (NNT) in second/third courses for one patient to achieve LDA at 6 months were two for adalimumab and three for secukinumab, ixekizumab, tofacitinib and ustekinumab, but five and four for apremilast and abatacept, respectively.
Numerous signalling patterns are modifiable in the complex and multifaceted disease entity of PsA. This has resulted in an increasing number of treatments available for the routine care treatment of PsA. Thus, treatment algorithms and suggestions of which treatment to use in which patient are of utmost interest. However, so far only three RCTs have reported direct comparisons across modes of action in PsA (adalimumab vs secukinumab,4 vs ixekizumab5 and vs upadacitinib6). The results of the present study are in line with the head-to-head comparison between adalimumab and secukinumab, indicating no significant differences regarding response to arthritis. However, our findings of poorer response outcomes for ixekizumab than for adalimumab are in contrast to the head-to-head trial. Several previous meta-analyses have also attempted comparisons across different drugs in PsA, some of which find results in line with ours. For example, one meta-analysis including TNFi, apremilast, ustekinumab and secukinumab reported better ACR20/50/70 week 24 responses for adalimumab compared with the non-TNFi treatments, as well as higher Psoriasis Area Severity Index (PASI) 75/90 responses.19 However, several of these analyses were funded by competing pharmaceutical companies, warranting some caution when interpreting the results.17–19 31
In our study, 17.7% of patients received treatment with four or more b/tsDMARDs. The retention and corresponding LUNDEX-corrected response rates were remarkably low for these fourth or more b/tsDMARD treatment courses. This resulted in high NNT (1.6%–8.1% reaching DAPSA28 LUNDEX-corrected remission, with corresponding NNTs of 63 and 12) and adds to the discussion on the value of switching between multiple antirheumatic medications. Recent points to consider within rheumatoid arthritis address the importance of investigating residual inflammatory activity in case of multiple treatment failures, and to approach factors such as depression, lifestyle or coping.32–34 Although no definition of difficult-to-treat PsA exists, the same type of multimodal approach is likely important here, since previous studies have indicated fibromyalgia, high body mass index and comorbidities contribute to multiple treatment failures in PsA.35–37 Indeed, our study emphasises that some patients seem to cycle several b/tsDMARDs with apparently minimal effects. However, prediction analyses of the factors associated with difficult-to-treat disease were beyond the scope of this study.
This study has several strengths. The collaboration across five countries increases power for rare exposures and offers insights into differences in treatment patterns. Extensive linkages to nationwide registries allowed for identification of concomitant comorbidities and extra-musculoskeletal manifestations. The lack of direct pharma funding sets the study apart from many of the previous comparisons across different b/tsDMARDs in PsA.
Some limitations also need to be pointed out for this study. The PsA disease entity is heterogeneous, and disease manifestations include psoriasis (of skin, nails), dactylitis, enthesitis, axial disease, uveitis and inflammatory bowel disease, not to mention metabolic syndrome and other comorbidities. Channelling across treatments, due to this heterogeneity, is likely to occur, and although we accommodated this to some extent by adding comorbidities to the multivariable analyses, residual confounding is likely to have impacted our results. Further, all types of disease domains are not covered in the outcome measures—for example, skin manifestations, dactylitis and enthesitis are not sufficiently captured in the rheumatology registries contributing to this study, and while 28-joint counts are available the data on 66/68-joint counts had high missingness and data on axial involvement were not available. This could impact our study results as the available b/tsDMARDs affect the PsA domains differently.38 Other comorbidities that are primarily treated in primary care, such as depression and fibromyalgia, are also not adequately captured through the national registers and may be prevalent in difficult-to-treat patients. The differences in use of b/tsDMARDs between countries are also remarkable. Overall, Sweden and to some extent Finland seemed to have higher proportional use of newer b/tsDMARDs, where apremilast was used even as first-line b/tsDMARD. In Denmark, apremilast is not included in the national recommendations for routine care treatment of PsA, and is in Norway not reimbursed in the public healthcare system, resulting in negligible use in these countries.39 40 This differential use across countries could have biased our results if access to treatment and monitoring differed between countries. Further, a consequence of TNFi normally being used as the first b/tsDMARD,39 41 the comparatively good performance of adalimumab in this study may be boosted by clinicians choosing a TNFi (such as adalimumab) in case of secondary inefficacy of a first TNFi (and thus in a population perhaps more prone to respond to TNF inhibition), but to switch mode of action in case of primary inefficacy. We unfortunately did not have data to explore this further.
Conclusion
In this large observational study of newer b/tsDMARDs in PsA, the inferior outcomes for certain newer b/tsDMARDs versus adalimumab highlight their unestablished position in the PsA treatment algorithm. The poor remission rates irrespective of mode of action in biologic-experienced patients challenge the feasibility of treat-to-target approaches and pinpoint the need for additional treatment alternatives, including non-pharmacologic interventions.
Data availability statement
Due to privacy and ethical concerns any raw data can not be shared. Aggregated data can be shared upon reasonable request
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the data protection and/or ethical committees in each of the Nordic countries, as required. Denmark: Capital Region Data Protection Office (RH-2015-209, I-suite 04145); ethical approval not required for registry studies (komitélovens §14, stk 2; www.nvk.dk). Finland: Helsinki University Hospital Coordinating Ethics Committee (73/13/03/00/2014). Norway: Regional Ethics Committee of South Eastern Norway (2011/1339 and 2017/243). Sweden: Ethical Review Board Stockholm (2015/1844-31/2). Iceland: National Bioethics Committee of Iceland (17-048-V13 and VSNb2017010049/03.01). Informed written consent for the reporting of anonymised registry data for research purposes was not required according to the approval committees, apart from Norway where such approval was required (and collected) for patients included after 2012. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
On behalf of the Danish DANBIO, Swedish SRQ, Norwegian NOR-DMARD, Finnish ROB-FIN and Icelandic ICEBIO registries.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
BGI and DDG contributed equally.
Contributors Substantial contributions to study conception and design: BGl, DDG, UL, JKW. Substantial contributions to acquisition of data: all authors. Substantial contributions to analysis and interpretation of data: DDG, UL, BGl, JKW. Drafting the article or revising it critically for important intellectual content: all authors. Final approval of the version of the article to be published: all authors. Guarantor of the overall content: BGl
Funding The study is partly funded by NordForsk and Foreum grants. It is also partly funded by Vinnova, Swedish Research Council, Swedish Heart Lung Foundation and Karolinska Institutet/Region Stockholm (ALF). The Center for Treatment of Rheumatic and Musculoskeletal Diseases (REMEDY) is funded as a Centre for Clinical Treatment Research by the Research Council of Norway (project 328657).
Competing interests BG: Pfizer, BMS, Sandoz and chairs the steering committee of the Danish Rheumatology Registry (DANBIO), which receives public funding from hospital owners and funding from pharmaceutical companies. JKW: AbbVie, Amgen, Eli Lilly, Novartis and Pfizer. DCN: AbbVie, BMS, Lilly, MSD, Novartis, Pfizer, Roche and UCB. MLH: AbbVie, Biogen, BMS, Celltrion, Eli Lilly, Janssen Biologics BV, Lundbeckfonden, MSD, Pfizer, Roche, Samsung Bioepis, Sandoz and Novartis. JA: AbbVie, BMS, Eli Lilly, Galapagos, MSD, Pfizer, Roche, Samsung Bioepis and Sanofi. Agreements between Karolinska Institutet (with JA as PI) and the listed entities, mainly for the national safety monitoring of rheumatology immunomodulators in Sweden (ARTIS). TS: AbbVie, BMS, Celgene, Medac, Merck, Novartis, Orion Pharma, Pfizer, Roche, Sandoz, UCB and Boehringer Ingelheim. SAP: Boehringer Ingelheim. BM: Novartis. EKK: Center for Treatment of Rheumatic and Musculoskeletal Diseases (REMEDY) funded as a Centre for Clinical Treatment Research by the Research Council of Norway (project 328657). LD: BMS, Janssen, UCB and Boehringer Ingelheim.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.