Article Text

Abstract
No single organ has received as much attention in systemic lupus erythematosus (SLE) as the kidneys. During the period 2019–2022, the Annals of the Rheumatic Diseases published several original papers, brief reports and letters that further elucidate the pathogenesis and advance the management of LN. A selection of representative original papers is highlighted in this review.
- Lupus Erythematosus, Systemic
- Lupus Nephritis
- Autoimmunity
Statistics from Altmetric.com
Introduction
Approximately 20%–40% of patients with systemic lupus erythematosus (SLE) may develop kidney disease. More importantly, lupus nephritis (LN) is a major cause of morbidity increasing substantially the risk for kidney failure (by up to 45×) and death (by up to 3×) especially among younger patients. To this end, in a recent publication from Canada, the all-cause age-specific standardised mortality ratio (SMR) was particularly high in younger (19–39 years old) patients with SLE (SMR=12.4) as compared with individuals older than 40 years (SMR=3.1). Of note, the all-cause and cause-specific SMR significantly decreased over time, likely reflecting the advances in the management of the disease and its comorbidities.1
During the period 2019–2022, the Annals of the Rheumatic Diseases published several original papers, brief reports and letters that further elucidate the pathogenesis and advance the management of LN. A selection of representative original papers is highlighted below.
Part I: pathogenesis and novel molecular targets: new and old players
Why do some patients with SLE develop LN? The interaction of genes and environment
LN has a high genetic load
Patients with SLE with severe disease—including nephritis—have a high genetic risk score—calculated based on 57 SLE risk loci—and are more likely to develop lupus earlier, accrue damage and have decreased survival. Of note, LN patients with increased genetic risk score have a higher risk for end-stage kidney disease (ESKD) (OR 5.58), proliferative LN (odds ratio [OR) 2.42) and anticardiolipin antibodies (OR 1.89–2.29) and decreased overall survival (HR for death 1.83).2
STAT4, smoking and LN
Intronic single nucleotide polymorphisms in the STAT4 gene, tagged by rs7574865[T], are associated with increased susceptibility to SLE and a more severe disease phenotype, with nephritis and stroke. What could be the possible link between SLE and the STAT4 gene?
IL-12 signalling through STAT4 is essential for induction of optimal levels of interferon (IFN)-γ production and commitment of Th1 cells. T cells from patients with SLE carrying the rs7574865[T] allele display an augmented response to IL-12 and IFN-α, and this subset of patients could benefit from JAK inhibition treatment. Smoking in the presence of the STAT4 risk gene variant increases the risk of myocardial infractions and nephritis in SLE (OR 2.14 and 1.53, respectively). Levels of IL-12 induced phosphorylation in CD8 T cells are higher in smokers. These data highlight the role of the IL-12-STAT4 pathways in SLE-cardiovascular and renal morbidity and its interaction with smoking.3
Why only few patients with the STAT4 SLE risk allele develop SLE? IFN-a as an environmental modifier
The majority of STAT4 risk allele carriers do not develop disease, posing the question whether this allele exerts the same effect in healthy individuals. Given the important role of type I IFN in SLE, IFN-α was explored as a putative environmental modulator of the STAT4 risk allele. Indeed, IFN-α enhances the IL-12-induced STAT4 activation selectively in carriers of the STAT4 SLE risk allele rs7574865[T]. Importantly, this particular STAT4 risk allele has opposite effects in healthy individuals compared with patients with SLE, due to the effect of IFN-α. This finding may explain why the majority of risk allele carriers do not develop disease, and suggests a mechanism whereby STAT4 risk allele carriers are at risk to develop SLE when IFN production is triggered (for instance during a viral infection).4
Missing heritability in SLE and shared genetic basis for SLE and kidney function response to injury
Genome-wide association studies have identified more than 100 susceptibility loci for SLE risk, yet these known loci only partially explain the disease heritability. In a meta-analysis, Yin et al identified 113 genomic regions including 46 novel loci for SLE risk. The study prioritised 110 putative causal variants including 10 putative causal variants with high confidence (posterior probability ≥0.8). Of interest, the study found for the first time the significant genetic correlations between SLE, albumin/globulin ratio and non-albumin protein. These shared genetic basis findings might suggest a common pathway underlying the SLE risk and kidney function, in addition to the direct damage of SLE autoantibodies.5
The internal environment in SLE: gut microbiota dysbiosis triggers LN
The gut microbiota exerts a strong influence over the host immune system and dysbiosis of this microbial community can affect the clinical phenotype in chronic inflammatory diseases. Emerging evidence suggests that gut microbiota dysbiosis may play crucial role also in the occurrence and development of SLE. LN patients have decreased species richness diversity in faecal samples, with overrepresentation of Ruminococcus gratus and Lachnospiraceae family associated with specific antibacterial and autoantibody responses for anti-DNA and low C3 and C4. These data suggest that akin to other rheumatic diseases such as spondyloarthritis and rheumatoid arthritis, epithelial surfaces such as the gut may constitute also a gateway for LN, stimulating antibacterial and autoantibody responses likely through toll-like receptors (TLRs) and other pathogen-associated and damage-associated molecular patterns.6 7
Why is the treatment of LN challenging? Data from transcriptome analysis, novel targets and liquid biopsy
The transcriptome represents the closest genomic correlate to disease phenotype. Thus, RNA sequencing-based transcriptomic analysis may provide insights to pathogenesis, biomarkers and potential molecular targets for the disease. Among all patients with SLE, active LN patients have the most widespread perturbation in gene expression, with over 6000 genes displaying altered expression in the peripheral blood, with signatures specific for IFN, granulocytes and plasmablast/plasma cell pathways. These patients also have perturbed mRNA splicing enriched in immune system and IFN signalling genes. This complex pathophysiology may explain the low rates of complete response at 6 months after treatment and support multitargeted approaches for nephritis.8 Comparative cross-tissue and cross-species analysis in gene expression between murine and human SLE in combination with machine learning analysis showed that the murine kidney transcriptome partially mirrors the blood transcriptome of patients with LN, with at least 11 key transcription factors regulating the cross-species active LN signature. Integrated protein-to-protein interaction and drug prediction analyses identified the kinases TRRAP, AUT2, CDK16 and SCYL1 as putative targets of these factors and capable of reversing the LN signature. Importantly, a set of 20 genes in the peripheral blood can discriminate LN from non-LN patients and this could be further explored as a liquid biopsy for LN.9
Neutrophils in LN: the underappreciated cells
A strong granulocytic signature in the peripheral blood and increased rates of NETosis have been reported in LN. Neutrophil extracellular traps (NETs) are networks of extracellular webs composed of extruded nuclear DNA and associated granular components, histones and cytoplasmic proteins. Yet, very few intact neutrophils are present in kidney biopsies. At the same time, agents that cause neutropenia such as cyclophosphamide are effective in severe LN. How could someone put these data together? The following papers published in the Annals of the Rheumatic Diseases shed light into the role of neutrophils and NETosis in LN.
Emergency granulopoiesis and extramedullary haemopoiesis in SLE
Emergency granulopoiesis is the de novo generation of neutrophils in response to immune activation. Extramedullary haematopoiesis (EMH) is the expansion and differentiation of haematopoietic stem and progenitor cells outside of the bone marrow. The ultimate goal of these two processes is primarily to enhance neutrophil output from the bone marrow to meet the higher demand for neutrophils on immune activation, when these cells are consumed in large quantities during the innate immune response in inflamed tissues. Patients with severe lupus such as nephritis have a strong myeloid signature indicative of activation of neutrophils, emergency myelopoiesis and EMH which may sustain and amplify the inflammatory response and contribute to the risk of flare. More specifically, in SLE deregulation of haemopoiesis is characterised by myeloid skewing and priming of proinflammatory ‘immune trained’—haemopoietic stem and progenitor cells (HSPCs). These primed HSPCs promote granulopoiesis at the expense of lymphopoiesis and support EMH, which takes place in the spleen and kidney and correlates with LN activity. EMH at these sites may provide the inflammatory license to neutrophils produced in the periphery to mediate kidney and endothelial injury likely via NETosis, as will be discussed next.10
Autophagy and NETosis in LN
Autophagy is an intracellular degradation system aiming to maintain neutrophil homoeostasis in response to immunological stress, wherein it is upregulated. Autophagy is essential for major neutrophil functions, including differentiation of progenitor cells of the myeloid lineage toward neutrophils, degranulation, reactive oxygen species production and release of NETs. Patients with LN have increased autophagy in their neutrophils associated with the REDD1 pathway resulting in increased NETosis. Tissue factor-bearing and interleukin 17A-bearing NET are abundant in discoid skin lesions and in the glomerular and tubulointerstitial compartment of proliferative LN specimens. Active NETs represent scaffolds with high concentration of bioactive IL-17A and TF that remain in end-organ tissues even in the absence of intact neutrophils, activating resident cells and promoting thromboinflammation and fibrosis. This may provide a link between thromboinflammation and fibrosis in SLE and may account at least in part for the salutary effects of hydroxychloroquine (HCQ) in LN, since HCQ inhibits the autophagy/REDD1/NETosis pathway.11 Together, these data suggest that although intact neutrophils may not be present in LN, their remnants in the form of NETs may amplify the inflammatory response beyond their short lifespan in the tissues.
B cells in LN: not be ignored
B cells, upregulation of mitochondrial respiration and increased organ damage
Transcriptomic, epigenomic and genomic analyses using 19 immune cell subsets from peripheral blood of patients with SLE revealed oxidative phosphorylation (OXPHOS)/mitochondrial dysfunction in SLE memory B cells. An OXPHOS-regulating gene, PRDX6 (peroxiredoxin 6), was a key driver in SLE B cells and pathology including LN. Prdx6-deficient B cells showed upregulated mitochondrial respiration, as well as increased antibody production. Since OXPHOS consists of the electron transport chain, a functional unit in mitochondria, these findings suggest the importance of mitochondrial dysfunction as a key immunological pathway involved in SLE.12
Part II: management of LN
Early diagnosis: the SLE Risk Probability Index
The diagnosis of SLE often poses significant challenges especially at early stages, when adequate features may not be present. The SLE Risk Probability Index (SLERPI) is a machine learning-based model that includes 14 variably weighted, standard clinical and serological features and can produce individualised SLE risk probabilities, enabling the classification into unlikely, possible, likely and definite SLE. The model showed very high combination of sensitivity and specificity for SLE (including early and severe forms of SLE, like LN) against competing rheumatologic diagnoses. The logistic regression model can be converted into a simple scoring system for both clinical and serological features, with an operational cut-off score of 7. Items of relevance to LN are scored in the SLERPI as follows: proteinuria more than 500 mg/24 hours: 4.5, positive ΑΝΑ: 3; low C3 and low C4: 2; anti-DNA or antiphospholipid antibodies: 2.5. The sensitivity of SLERPI for LN is as high as 98%.13
Histology: new common patterns of injury in class III/IV LN
The International Society of Nephrology/Renal Pathology Society classification with its 2018 revision is the gold standard for the characterisation of LN on renal biopsy, with therapeutic repercussions. To further improve and simplify the clinical relevance of this scoring system, a total of 353 renal biopsies from the Belimumab International Study in LN were assessed through central pathology review. Using a novel method to partition the cases into k clusters based on their similarity (KMeans), features from the cohort of ‘pure’ class III/IV cases (n=214) were analysed to determine alternative subdivisions based on phenotypic data. To this end, KMeans revealed the presence of two main clusters, membranoproliferative-like (n=83) or vasculitis-like (n=131). This study introduces two new phenotypic forms of LN, surpassing the traditional classes as determined by the current classification. Future validation and confirmation are required for these findings, including assessment of their impact on response to therapy and prognosis.14
Renal outcomes and response to therapy
Increased awareness for LN in European centres over the last decade, facilitated by the EULAR recommendations for SLE first published in 2008, has led to earlier recognition of LN and better outcomes, with an estimated 20-year ESKD rate of 10%, as compared with 20% in previous years. In a cohort of 381 patients (90.5% Caucasians), patients achieving the EULAR/ERA-EDTA response criteria at 1 year (either complete (defined as proteinuria <0.5 g/24 hours, (near) normal estimated glomerular filtration rate (GFR), or partial response (≥50% proteinuria reduction to subnephrotic levels, (near) normal eGFR) had good renal outcomes. In this cohort, after 12 months of therapy, 58%, 26% and 16% of patients achieved complete, partial and no response, respectively. During a median follow-up of 10.7 years, 53 patients developed CKD. At 15 years, CKD-free survival rate was 95.2%, 87.6% and 55.4% in patients with complete, partial and no response at 12 months, respectively (p<0.0001). Of note CKD-free survival rates did not differ between complete and partial responders (p=0.067).15
Conventional immunosuppressive therapy in LN: further refinements and new agents
Duration of immunosuppressive therapy
The optimal duration of maintenance immunosuppressive therapy (IST) is unknown. The WIN-Lupus trial tested whether IST discontinuation after 2‒3 years was non-inferior to IST continuation for two more years in patients with proliferative LN. Between 2011 and 2016, 96 patients were randomised to continue (n=48) or discontinue IST (n=48). Relapse of proliferative LN occurred in 5/40 (12.5%) patients with IST continuation and in 12/44 (27.3%) patients with IST discontinuation (difference 14.8%). Severe SLE flares (renal or extrarenal) were less frequent in patients with IST continuation (5/40 vs 14/44 patients; p=0.035). Adverse events did not differ between the groups. These data confirm previous reports that IST discontinuation is associated with a higher risk of severe SLE flares.16
MMF versus tacrolimus as initial therapy: tacrolimus may be an alternative for MMF
Randomised controlled trials (RCTs) of LN have shown that the difference in kidney function preservation of various treatment regimens may be more obvious after at least 5 years of therapy. In a study reporting the 10-year outcomes of a large cohort of patients with LN treated with either MMF or tacrolimus induction, followed by azathioprine maintenance, there were no significant differences in renal flares or kidney function decline between the two regimens. A urinary protein creatinine ratio (UPCR)≤0.75 g/g and eGFR≥80 mL/min at month 18 best predicted a favourable outcome. Maintenance therapy of less than 5 years was associated with higher flares. The authors concluded that tacrolimus may be considered as an alternative to MMF as induction therapy of LN, with treatment aiming at UPCR≤0.75 and eGFR≥80 mL/min by month 18. Maintenance therapy should best be continued for 5 years or more, particularly in high-risk patients. Despite these encouraging results, these data need to be replicated in non-Asian patient populations.17
Novel therapies and biomarkers
Novel agents for B cell depletion-Obinutuzumab is effective and safe
Two RCTs of the type I anti-CD20 antibodies rituximab and ocrelizumab in patients with LN failed to show a difference against placebo in the primary endpoint of complete renal response (CRR), yet subsequent analyses suggested that the rapidity, depth and duration of peripheral B-cell depletion are associated with favourable renal response. Obinutuzumab, a type II anti-CD20 antibody that results in deeper B-cell depletion than rituximab, proved superior to placebo for the achievement of complete and overall renal responses at week 52, when added to MMF and glucocorticoids in a phase 2 RCT (NOBILITY). Importantly, improved renal responses with obinutuzumab compared with placebo continued through week 104. Equally important, obinutuzumab resulted in rapid and potent depletion of peripheral B cells, without an increase in the incidence of serious adverse events, serious infections or death compared with placebo. Based on these results, the use of obinutuzumab in LN is being further evaluated in a global phase 3 study.18
Anifrolumab in LN: a higher dose may be required
Anifrolumab targets the type I IFN signalling pathway, which plays a role in the pathogenesis of LN. TULIP-LN was a phase II RCT exploring this IFN-targeted therapy in patients with active LN. In this trial, 147 patients were randomised (1:1:1) to receive monthly intravenous anifrolumab basic regimen (300 mg), intensified regimen (IR, 900 mg×3, 300 mg thereafter) or placebo, alongside standard therapy (oral glucocorticoids, MMF). Although the primary endpoint of the study (change in baseline 24-hour UPCR at week 52) was not met, anifrolumab IR was associated with increased numerical improvements over placebo across endpoints, including CRR (45.5% vs 31.1%), CRR with UPCR≤0.5 mg/mg (40.9% vs 26.7%), CRR with inactive urinary sediment (40.9% vs 13.3%) and sustained glucocorticoid reductions (55.6% vs 33.3%), suggesting that patients with LN may require an IR of anifrolumab relative to non-renal SLE, to obtain adequate drug exposure and clinical efficacy. Incidence of herpes zoster was higher with combined anifrolumab versus placebo (16.7% vs 8.2%). Incidence of serious adverse events was similar across groups.19
Urine biomarkers
Using a quantitative planar protein microarray, Vanarsa et al screened 1000 proteins in the urine of LN patients and found that 64 were elevated. Further analysis led to the discovery of urine Angptl 4 (a protein induced by peroxisome proliferation activators that acts as an apoptosis survival factor for vascular endothelial cells), L-selectin (a cell adhesion molecule found on the cell surface of leukocytes) and TGFb1 as potential biomarkers for LN disease activity.20
Concluding remarks
LN represents a key area of interest for Annals of Rheumatic Diseases. The papers highlighted above represent a small fraction of original articles published by the journal from 2019 to 2022.
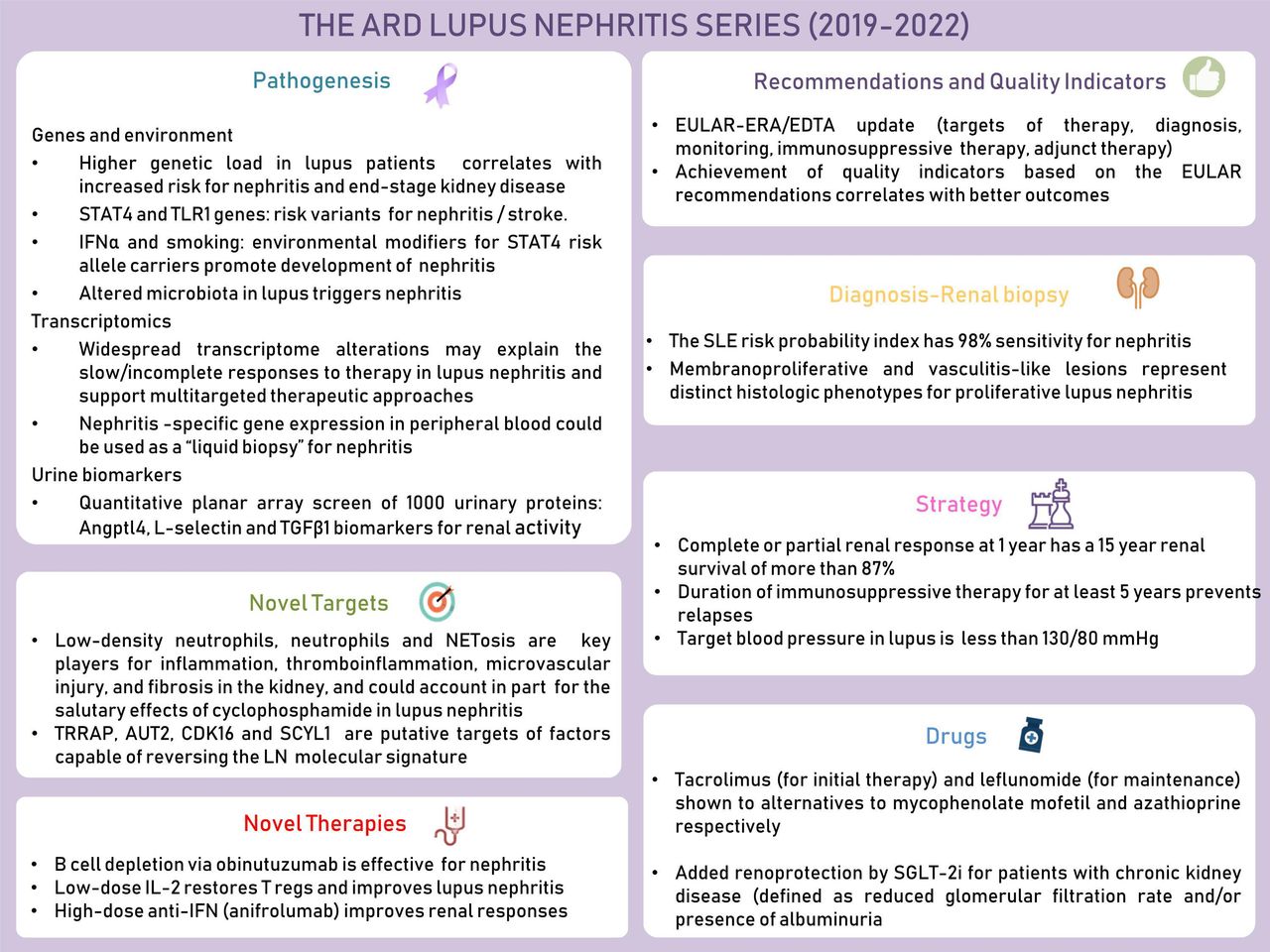
In addition to these papers discussed, several other papers and letters related to LN were published by the Annals of Rheumatic Diseases providing new data on the pathogenesis, novel targets and therapies, management strategy and recommendations, and drugs.21–35 Key findings from these papers are depicted in a graphical abstract (figure 1). Although several issues in LN still await further refinement, it is clear that significant advances have been made in the understanding and managing this most fascinating aspect of SLE.
{kind=link}
Key points from the annals of the rheumatic diseases lupus nephritis series (2019–2022). SLE, systemic lupus erythematosus.
Ethics statements
Patient consent for publication
References
Footnotes
Handling editor Josef S Smolen
Twitter @none
Contributors All authors have equally contributed to the writing, editing and reviewing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.