Article Text

Abstract
Objectives Our aim was to evaluate systemic lupus erythematosus (SLE) disease activity and SARS-CoV-2-specific immune responses after BNT162b2 vaccination.
Methods In this prospective study, disease activity and clinical assessments were recorded from the first dose of vaccine until day 15 after the second dose in 126 patients with SLE. SARS-CoV-2 antibody responses were measured against wild-type spike antigen, while serum-neutralising activity was assessed against the SARS-CoV-2 historical strain and variants of concerns (VOCs). Vaccine-specific T cell responses were quantified by interferon-γ release assay after the second dose.
Results BNT162b2 was well tolerated and no statistically significant variations of BILAG (British Isles Lupus Assessment Group) and SLEDAI (SLE Disease Activity Index) scores were observed throughout the study in patients with SLE with active and inactive disease at baseline. Mycophenolate mofetil (MMF) and methotrexate (MTX) treatments were associated with drastically reduced BNT162b2 antibody response (β=−78, p=0.007; β=−122, p<0.001, respectively). Anti-spike antibody response was positively associated with baseline total immunoglobulin G serum levels, naïve B cell frequencies (β=2, p=0.018; β=2.5, p=0.003) and SARS-CoV-2-specific T cell response (r=0.462, p=0.003). In responders, serum neutralisation activity decreased against VOCs bearing the E484K mutation but remained detectable in a majority of patients.
Conclusion MMF, MTX and poor baseline humoral immune status, particularly low naïve B cell frequencies, are independently associated with impaired BNT162b2 mRNA antibody response, delineating patients with SLE who might need adapted vaccine regimens and follow-up.
- lupus erythematosus
- systemic
- vaccination
- COVID-19
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
BNT162b2 efficacy and safety has been described in studies mixing different rheumatic and musculoskeletal diseases (RMDs).
What does this study add?
No serious adverse effects nor systemic lupus erythematosus (SLE) flares have been documented after BNT162b2 in patients with SLE.
Not only mycophenolate mofetil and methotrexate, but also a poor humoral immune status at baseline, impair vaccine antibody response.
Although decreased, serum neutralising activity against variants of concerns is conferred to vaccine responders.
How might this impact on clinical practice or future developments?
These parameters could be helpful for physicians to delineate which patients should have antibody measurement after full BNT162b2 vaccination and should be proposed a third injection of BNT162b2 vaccine.
Introduction
Because of the tremendous paucity of data on the impact of rheumatic and musculoskeletal diseases (RMDs) and associated immune-modulatory treatments on SARS-CoV-2 vaccination efficacy, most of the recommendations are currently based on expert opinions. Messenger RNA (mRNA) vaccination is a novel practice, and its tolerance, immunogenicity and efficacy are poorly documented in RMD. Consequently, rules for vaccine against SARS-CoV-2 vary according to country and over time.1 2 Factors affecting the anti-SARS-CoV-2 antibody response have been explored, but only after a first dose or in studies mixing RMD.3 4 Furthermore, the impact of treatments on the vaccine response is often studied mixing different RMDs.5 Importantly, Simon et al recently showed that interindividual variations to vaccination were more related to the disease itself rather than to concomitant treatments.3 Additionally, most of these studies focused on RMD treatments and not on the immunological status, which may also affect the antibody response. Among RMDs, systemic lupus erythematosus (SLE) could represent a peculiar challenge to vaccination against SARS-CoV-2.6 The deregulation of type I interferon (IFN) pathways associated with this condition7 might impact on vaccine antibody response.8 SLE-associated impaired lymphocyte functions might also impair vaccine efficacy.9 10 Altogether, the risk of flares induced by vaccines is highly dependent on the disease studied and the specific scores used to measure this activity. It is therefore important to focus vaccine evaluation on homogeneous groups of patients.
Compared with the general population, patients with SLE do not seem to be at higher risk of SARS-CoV-2 infections or severe COVID-19,11–14 but this finding remains controversial as other studies found that patients with SLE may be at higher risk of hospitalisation during their COVID-19 course.15 16 Increase of SLE disease activity has been previously reported during COVID-1917 18 but the risk of SLE flares following vaccination does not appear to be increased,18 although this point still requires confirmation through follow-up of patients with SLE evaluated at identical pre-vaccination and post-vaccination timepoints in a prospective study. Finally, it remains unclear whether failures to induce antibody responses in patients under immunomodulatory regimens such as abatacept, mycophenolate mofetil (MMF), CD-20 inhibitors, calcineurin inhibitors5 19 are also associated, or not, with an absence of vaccine-induced SARS-CoV-2-specific T cell responses. Here, we report post-vaccination disease activity data in 126 patients with SLE, prospectively followed during the completion of a two-dose mRNA Pfizer/BioNTech (BNT162b2) vaccination regimen. SARS-CoV-2-specific humoral and cellular responses were monitored against not only the SARS-CoV-2 historical strain but also against SARS-CoV-2 variants of concern (VOCs).
Methods
Patients
The clinical study was conducted in the Internal Medicine Department 2, French National Reference Center for SLE, Pitié-Salpêtrière Hospital, Paris, France. Eligible patients were 18 years or older, with a diagnosis of SLE according to the revised American College of Rheumatology (ACR) classification criteria.20 Active lupus was defined with two scores: (1) at least 1 British Isles Lupus Assessment Group (BILAG) B in any organ, (2) SLE Disease Activity Index (SLEDAI) 2K score >4. Patients were vaccinated according to the French recommendations for COVID-19 vaccination.2
Outcomes and follow-up
Patients were vaccinated at baseline (first dose) against SARS-CoV-2 with Pfizer/BioNTech (BNT162b2) vaccine and received the second dose at day (D) 21–28, unless contraindicated. Patients were evaluated at baseline and at D7–14, D21–D28, D42. Patients were asked to contact their physician if they developed any symptoms in order to be promptly examined.
At each visit, the following endpoints were assessed:
Adverse events.21
SLE activity measured with SLEDAI 2K score22 23 and BILAG score.24
SLE flares defined with the SELENA-SLEDAI Flare Index (SFI)22 23 and BILAG 2004 score.24–26
SARS-CoV-2 infection measured with anti-nucleocapsid antibodies.
Changes in serological activity (anti-dsDNA antibodies and C3), IFN-α, anti-phospholipid antibodies.27
Anti-spike antibodies.
B, T and natural killer cell quantification.
B lymphocyte subsets.
Patient and public involvement
Patients were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Serological analysis
SARS-CoV-2-specific immunoglobulin G (IgG) antibodies were measured as previously described.28 Serum samples were tested with the Maverick SARS-CoV-2 Multi-Antigen Serology Panel (Genalyte, USA) according to the manufacturer’s instructions. The panel is designed to detect antibodies to five SARS-CoV-2 antigens: nucleocapsid, spike S1 receptor binding domain (RBD), spike S1S2, spike S2 and spike S1, within a multiplex format based on photonic ring resonance technology. Briefly, 10 µL of each serum sample was added to a sample well plate array containing required diluents and buffers, and the plate and chip were loaded in the instrument for chip equilibration with the diluent buffer to measure baseline resonance. The serum sample was then charged over the chip to bind specific antibodies to antigens present on the chip. The chip was then washed to remove low-affinity binders, and specific antibodies were detected with anti-IgG secondary antibodies.
Pseudoneutralisation assay
Lentiviral particles carrying the luciferase gene and pseudotyped with spikes of SARS-CoV-2 historical strain or VOCs were produced by triple transfection of 293T cells as previously described.28 Serum dilutions were mixed and co-incubated with 300 transducing units of pseudotyped lentiviral particles at room temperature for 30 min and then diluted in culture medium (Dulbecco’s modified Eagle’s medium–GlutaMAX (Gibco)+10% fetal calf serum (Gibco)+1% penicillin/streptomycin (Gibco)). This mixture was then plated on tissue culture–treated black 96-well plates (Costar) with 20 000 HEK 293T-hACE2 cells per well in suspension. To prepare the suspension, cell flasks were washed with Dulbecco’s phosphate buffer saline (DPBS) twice (Gibco), and a single-cell suspension was made in DPBS+0.1% EDTA (Promega) to preserve integrity of hACE2 protein. After 48 hours, the medium was removed from each well and bioluminescence was measured using a luciferase assay system (Promega) on an EnSpire plate reader (PerkinElmer).
B cell phenotyping
B cell phenotyping was assessed on fresh whole blood. Briefly, 400 µL of blood was washed in PBS1X-RPMI 5% (Gibco) then transferred in tubes containing anti-CD45 V500, anti-CD19 APC, anti-IgD FITC, anti-CD38 PerCPCy5.5, CD27 PE-Cy7, CD24 APC-H7, CD86 PE, CD3 BV421, CD14 BV421, CD21 BV421 lyophilised antibodies (BD Horizon Lyo technology). This lyophilised version of the multicolour panel increases the reagent stability and the assay performance. Cell staining was performed at room temperature for 15 min, then cells were washed and fixed (BD Cell Fix). Events were acquired on a BD FACS Canto II flow cytometer (BD Biosciences) and analysed with FlowJo V.10 software (FlowJo, LLC) according to the gating strategy presented in online supplemental figure S1.
Supplemental material

Study population and enrolment process. Patients with systemic lupus erythematosus (SLE) were offered BNT162b2 vaccine through 15 January 2021.
SARS-CoV-2-specific T cell responses
SARS-CoV-2-specific T cell responses were assessed in the clinical immunology laboratory of Pitié-Salpêtrière Hospital by a whole blood Interferon-Gamma Release Assay (IGRA) following manufacturer’s instructions (Quantiferon SARS-CoV-2, Qiagen). This test uses two Qiagen proprietary mixes of SARS-CoV-2 spike protein (Ag.1 and Ag.2) selected to activate both CD4 and CD8 T cells. Briefly, venous blood samples were transferred into the Quantiferon tubes containing spike peptides as well as positive and negative controls. Whole blood was incubated at 37°C for 16–24 hours and centrifuged to separate plasma. IFN-γ (IU/mL) was measured in these plasma samples using QuantiFERON Human IFN-γ SARS-CoV-2 ELISA kit (Qiagen) on Dynex DS2 analyser (Qiagen).
Statistical analysis
Baseline characteristics are reported with descriptive statistics. Linear regression models were used to assess the association between clinical and biological characteristics and the titre of IgG anti-RBD at day 42 in unadjusted and multivariable analysis. We considered potential confounders known or suspected to be associated with vaccine response such as demographic features (age, sex), activity of SLE, concomitant immune modulatory treatments and data from T, B and NK cells phenotyping. The beta coefficient is the degree of change in the outcome variable for every 1 unit of change in the predictor variable. If the beta coefficient is not statistically significant (ie, the p value is not significant), the variable does not significantly predict the outcome. If the beta coefficient is significant, examine the sign of the beta. If the beta coefficient is positive, the interpretation is that for every 1-unit increase in the predictor variable, the outcome variable will increase by the beta coefficient value. If the beta coefficient is negative, the interpretation is that for every 1-unit increase in the predictor variable, the outcome variable will decrease by the beta coefficient value. For example, if the beta coefficient is 0.80 and statistically significant, then for each 1-unit increase in the predictor variable, the outcome variable will increase by 0.80 unit. Paired t-tests were used to detect differences in activity scores and biological data over time. As we excluded the 10 patients for whom follow-up was incomplete, we did not have to perform any imputation for missing data. Non-parametric test were used as Mann-Whitney U test to compare two independent groups, Wilcoxon test to compare paired values and Pearson coefficient to calculate correlation. Significant p values are indicated as follows: *p<0.05; **p<0.01; ***p<0.001; ****p<0.0001. Statistical analysis was performed using R software (V.4.1.0) and GraphPad Prism software, V.6 (GraphPad, San Diego, California, USA).
Results
Demographic and disease characteristics
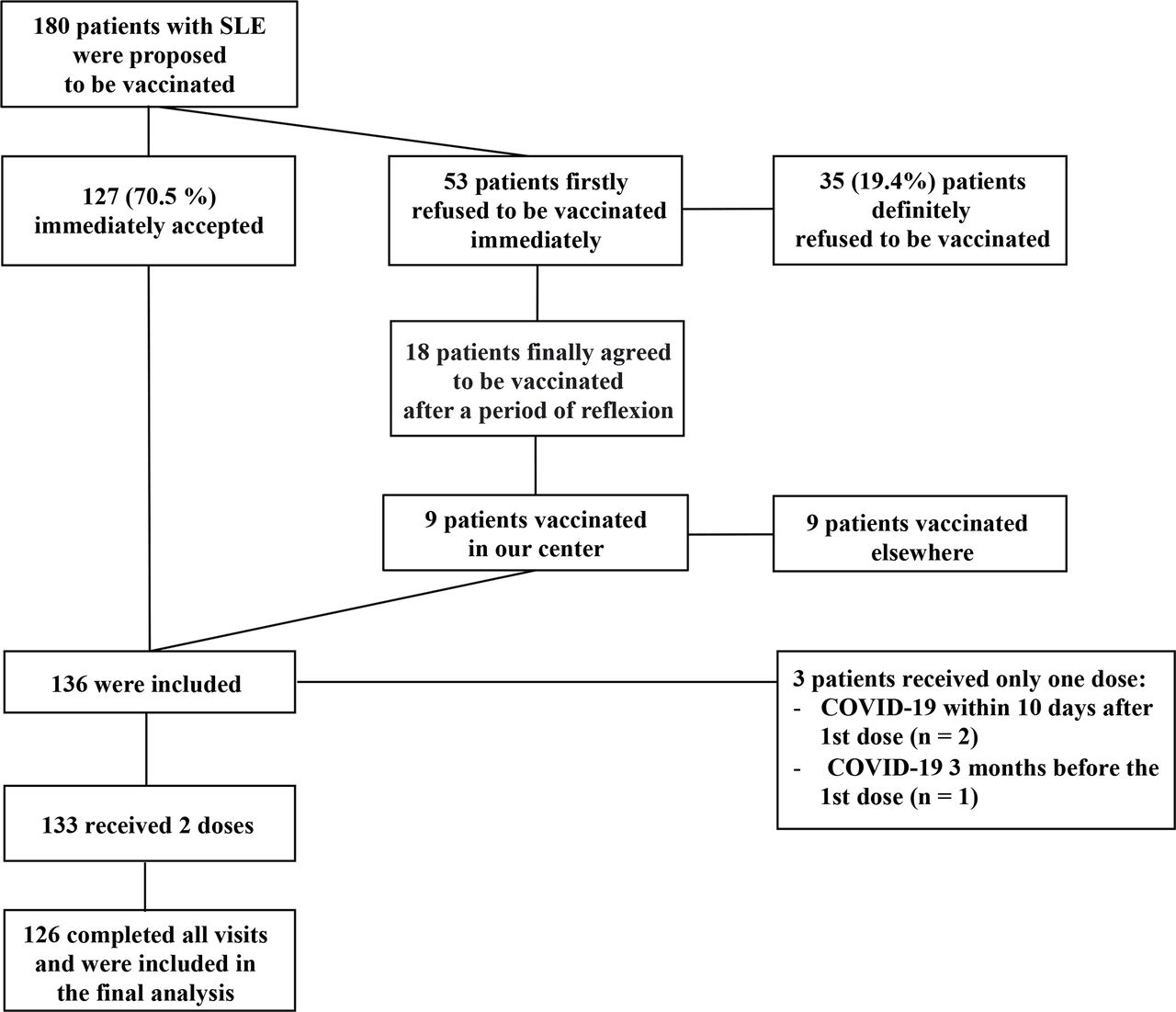
Vaccination against SARS-CoV-2 with Pfizer/BioNTech vaccine was proposed by their SLE referring physician to 180 patients with SLE; 127 (70.5 %) immediately accepted, 35 (19.4%) patients refused and 18 (10.0%) eventually accepted on reflection, 9 of them were vaccinated in another centre (figure 1). A total of 136 patients with SLE were enrolled and received one first dose; 3 patients received only one dose: either because they developed COVID-19 within 10 days after the first dose (n=2) or because COVID-19 had been contracted 3 months before the first dose (n=1). Among the 133 patients with SLE who received two doses, 126 (92.6%) completed all the visits and were included in the final analysis. Baseline clinical characteristics of these 126 patients are summarised (table 1). Treatments received from D1 to D42 were distributed as follows: hydroxychloroquine (n=106; 84.1%; median daily dose: 400 mg), prednisone (n=70; 55.5%) with 57 patients (45.2%) receiving less than 10 mg daily (median daily dose: 5 mg) and 13 (10.3%) more than 10 mg daily (median daily dose: 19 mg), methotrexate (n=20; 15.9%; median weekly dose 15 mg); mycophenolate mofetil (n=24; 19.0%; median daily dose=2000 mg), azathioprine (n=5; 4.0%; median daily dose: 100 mg) and belimumab (n=15; 11.9%), of whom 7 had intravenous and 8 subcutaneous injections, respectively.
Demographics and clinico-biological features of patients with SLE
Adverse BNT162b2 vaccine-associated events in patients with SLE
No related serious adverse events (AEs), no grade 4 reactions and no withdrawals due to related AEs were observed (online supplemental figure S2 and online supplemental table S1). Local reactions, predominantly pain at the injection site, were mild to moderate (grade 1 and 2).
Supplemental material
Supplemental material

Evolution of systemic lupus erythematosus (SLE) activity following vaccination. (A) Repartition of maximal British Isles Lupus Assessment Group (BILAG) score at baseline and following vaccination. (B) Evolution of mean SLE Disease Activity Index (SLEDAI) 2K score following vaccination.
BNT162b2 vaccine effect on SLE disease activity
At baseline, 29 (23.0%) and 20 (16.7%) patients had active SLE according to SLEDAI (SLEDAI 2K>4) and to BILAG (≥1 BILAG B), respectively. Within 42 days following vaccination (figure 2A), mild disease flares were observed in three patients following vaccination, with a mucocutaneous BILAG score going from C to A in one individual, a musculoskeletal BILAG going from C to B in one individual and from D to C for one another vaccinated patient. In return, nine patients (five active and four inactive) clinically improved following vaccination with a musculoskeletal BILAG going from B to C for four patients and from C to D for three patients, a mucocutaneous BILAG going from A to C for one patient and a renal BILAG going from A to B for one patient. No statistically significant variation of SLEDAI score was observed throughout the study for patients with active and inactive SLE according to initial SLEDAI score (SLEDAI 2K score ≤4 at day 1: mean (SD); 1.2 (1.4) day 1; 1.3 (1.2) day 14; 1.0 (1.2) day 28; 1.3 (1.4) day 42, ns; SLEDAI score >4 at day 1: 11 (5.1) day 1; 10.1 (4.9) day 14; 10.0 (5.3) day 28; 9.9 (5.3) day 42, ns; figure 2B). Altogether, vaccination is not preferentially associated with exacerbation of SLE symptoms than with clinical improvement. When observed, variations of BILAG and SLEDAI scores were not preferentially observed in patients with either active or inactive SLE at baseline.
Effect of treatments and baseline immune status on the immunogenicity of the BNT162b2 vaccine in SLE
Higher total serum IgG levels measured at baseline were associated with better seropositivity rates (β=2.0; 95% CI 0.34 to 3.6; p=0.018), while MMF and MTX uses were associated with lower anti-spike antibody production(β = −78; 95% CI −133 to –22; p=0.007 and β=−122; 95% CI −184 to –61; p<0.001, respectively) measured 14.7 days on average after the second injection (SD 1.9 days). Total lymphocyte counts and IFN-α levels at baseline were not significantly associated with seropositivity rates (table 2). Hydroxychloroquine, steroids (either high or low dose) or belimumab use during the 42 days following vaccination did not impact anti-spike antibody production. Of note, SLE activity was not correlated with anti-spike antibody response, regardless of the score used to measure disease activity (see table 2 and online supplemental table S2 with BILAG and SLEDAI, respectively).
Baseline predictors of day 42 anti-SARS-CoV-2 RBD IgG titres according to linear regression model
Since IgG levels but not total lymphocyte counts were significantly associated with the antibody response, we next studied the effect of lymphocyte subpopulation counts at baseline (table 3).
Baseline B, T and NK cell count predictors of day 42 anti-SARS-CoV-2 RBD IgG titres according to linear regression model
We found that B lymphocyte counts were the sole lymphocyte population associated with anti-spike antibody response (β=0.38; 95% CI 0.13 to 0.62; p=0.003). We further characterised the effect of B lymphocyte subsets at baseline. Treatments modifying B cell subpopulations were adjusted in this analysis (table 4). Strikingly, naïve B lymphocyte frequency at baseline was positively associated with anti-spike antibody response at D42 (β=2.5; 95% CI 0.87 to 4.0; p=0.003; table 4).
Baseline B cell predictors of day 42 anti-SARS-CoV-2 RBD IgG titres according to linear regression model
Effect of treatments on BNT162b2-induced neutralisation responses
We next analysed whether vaccine-induced antibody responses may be protective by evaluating serum-neutralising activity. As expected, we confirm a strong correlation between anti-RBD antibody levels and neutralisation titres (SARS-CoV-2 D614G r=0.82, p<0.0001; figure 3A). Consequently, parameters listed above influencing seroconversion also influenced neutralisation activity (online supplemental table S3). MMF and MTX in particular have a negative impact on induction of neutralising activity (β=−1.1; 95% CI −1.9 to –0.34; p=0.005 and β=−1.9; 95% CI −2.7 to −1.1; p<0.001, respectively, online supplemental table S3). While a majority of MMF/MTX-treated patients still harboured detectable neutralising activity (65% (15/23) MMF-treated patients, 68% (13/19) MTX-treated patients vs 96% (81/84) patients without MMF or MTX), their serum neutralising activity drastically dropped compared with patients receiving other treatments (inhibitory dilution 50 (ID50) D614G median(min–max); 111.2 (30–18 910) in MMF-treated patients vs 90.4 (30–5527) in MTX-treated patients and 684.6 (30–12061) in other patients; p<0.05; figure 3B).
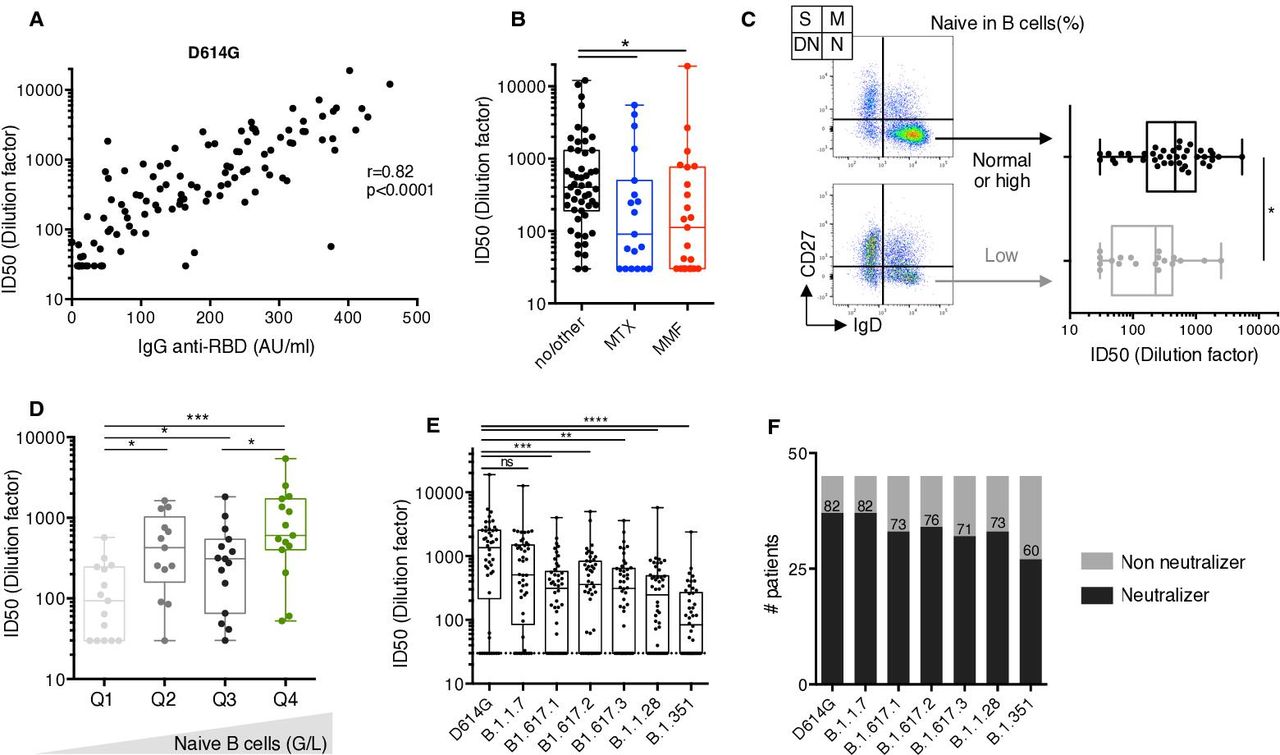
Vaccine-induced neutralising potency. (A) Comparison of serum anti-RBD IgG levels measured by photonic ring immunoassay with neutralising capacity against D614G SARS-CoV-2 (n=126). Spearman coefficient (r) and p value (p) are indicated. (B) Serum neutralising activities against D614G SARS-CoV-2 measured as inhibitory dilution 50 (ID50) in 126 serum samples at D42. Methotrexate (MTX)-treated and mycophenolate mofetil (MMF)-treated patients are colour coded (blue and red, respectively). Patients receiving other treatments are indicated in black. The boxplots show medians (middle line) and first and third quartiles, while the whiskers indicate minimal and maximal values. P value was calculated using Kruskal-Wallis test (*p<0.05). (C) Comparison of serum neutralising activities measured as ID50 against D614G SARS-CoV-2 in patients with systemic lupus erythematosus (SLE) with baseline low (grey, n=19) or high (black, n=40) naïve B cell frequency (arbitrary cut-off=42% of total B cells). Naïve B cells (N) are defined as CD27-Ig+ B cells, switched memory B cells (S) as CD27+IgD-, marginal zone B cells (M) as CD27+IgD+ and double negative B cells (DN) as CD27-IgD-. The boxplots show medians (middle line) and first and third quartiles, while the whiskers indicate minimal and maximal values. P value was calculated using Mann-Whitney test (*p<0.05). (D) Serum neutralising activities against D614G SARS-CoV-2 measured as ID50 in 59 patients with SLE classified according to their naïve B cell counts. Q1, Q2, Q3 and Q4 defined the naïve B cell count quartiles. P value was calculated using Kruskal-Wallis test (*p<0.05; ***p<0.001). (E) Serum neutralising activities against indicated SARS-CoV-2 variants B.1.1.7 (Alpha), B.1.617.1 (Kappa), B.1.617.2 (Delta), B.1.617.3, B.1.28 (Gamma) and B.1.351 (Beta) measured as ID50 in 46 serum samples at D42. The boxplots show medians (middle line) and first and third quartiles, while the whiskers indicate minimal and maximal values. P value was calculated using Kruskal-Wallis test (**p<0.01; ***p<0.001; ****p<0.0001). (F) Positive rates of serum neutralising activity against SARS-CoV-2 variants in 46 SLE samples at day 42. Patients were defined as ‘neutralisers’ (black) or ‘non-neutralisers’ (grey) according to the presence of neutralising activity at first serum dilution (1/30), or not. IgG, immunoglobulin G; RBD, receptor binding domain.
Effect of baseline immune status on BNT162b2-induced neutralisation responses
Consistent with serological studies, naïve B cell decrease at baseline was negatively associated with serum D42 neutralising activity (β=0.04; 95% CI 0.01 to 0.07; p=0.006; online supplemental table S4). As shown in figure 3C, patients with a low naïve B cell compartment (<42% of B cells) developed a lower neutralising activity than patients with normal or high naïve B cell subset frequencies (229.2 (30–2510) in low naïve B cell patients vs 468.3 (30–5421); p<0.05; figure 3C). To more accurately evaluate the effect of naïve B cells on neutralising antibody response, we divided patients with SLE into four groups according to their naïve baseline B cell counts (median(min–max) naïve B cell counts/μL: 9 (0.01–23.2); 41 (27.2–50.9); 68.1 (57.2–98.7); 133.8 (110.1–160.2) in quartiles 1, 2, 3 and 4, respectively; figure 3D). We confirm that naïve B cell counts are positively associated with vaccine-induced neutralising antibody responses (ID50 D614G 93.4 (30–246.5) vs 340.1 (30–1632) in quartiles 1 and 2, respectively; p<0.05 vs 315.2 (30–721.1) in quartile 3; p<0.05; vs 679.9 (60.4–2510) in quartile 4; p<0.001; figure 3D).
These data therefore underline the importance of interrogating initial B cell status as well as immunosuppressive treatments to predict vaccine response.
Broad neutralising activity against VOCs in BNT162b2 vaccine responders
The Pfizer/BioNTech vaccine was designed to target the Wuhan isolate described by the end of 2019. However, emerging variants, with enhanced infectivity and the ability to escape immune control, rapidly became dominant. Concerns have been raised as to whether Pfizer/BioNTech vaccine will be effective against these emerging variants, particularly in vaccinated individuals receiving immunosuppressive drugs. We therefore measured neutralising activities in the last 46 serum samples longitudinally collected against four major SARS-CoV-2 lineages: B.1.1.7 (originating in the UK), B.1.351 (described in South Africa), B.1.1.28 (reported in Brazil) and B.1.617 (emerged in India). Consistent with previous studies,29 30 we found that vaccine-induced IgG antibodies efficiently cross-neutralise variants B.1.1.7 (ID50 median (min–max); D614G 1453 (30–18 910) and B.1.1.7 514.5 (30–12 625), ns; figure 3E). It is noteworthy that serum neutralisation activity decreased with lineages bearing the E484K mutation in the RBD (ID50 B1.617.1 341.1 (30–3996), p<0.001; B.1.617.2 379.3 (30–4982), p<0.001; B.1.617.3 317.9 (30–3604), p<0.01; B.1.1.28 302.3 (30–5757) and B.1.351 88.1 (30–2389); p<0.0001; figure 3E), but remained detectable in a majority of patients (82% for B.1.1.7; 73% for B.1.617.1; 76% for B.1.617.2; 71% for B.1.617.3; 73% for B.1.1.28; 60% for B.1.351; figure 3F). Among patients with neutralising antibody activity against D614G strain, 100% (37/37) of patients also efficiently neutralised B.1.1.7 strain, 89% (33/37) B.1.617.1 variant, 92% (34/37) B.1.617.2 variant, 87% (32/37) B.1.1.28 variant, 89% (33/37) B.1.1.28 variant and 60% of patients (27/37) had detectable neutralising activity against B.1.351.
Altogether, these results demonstrated that vaccinated-SLE harboured decreased neutralising activity against VOCs, as previously described in vaccinated healthy donors.31 32
SARS-CoV-2-specific T cell responses induced by the BNT162b2 vaccine in SLE
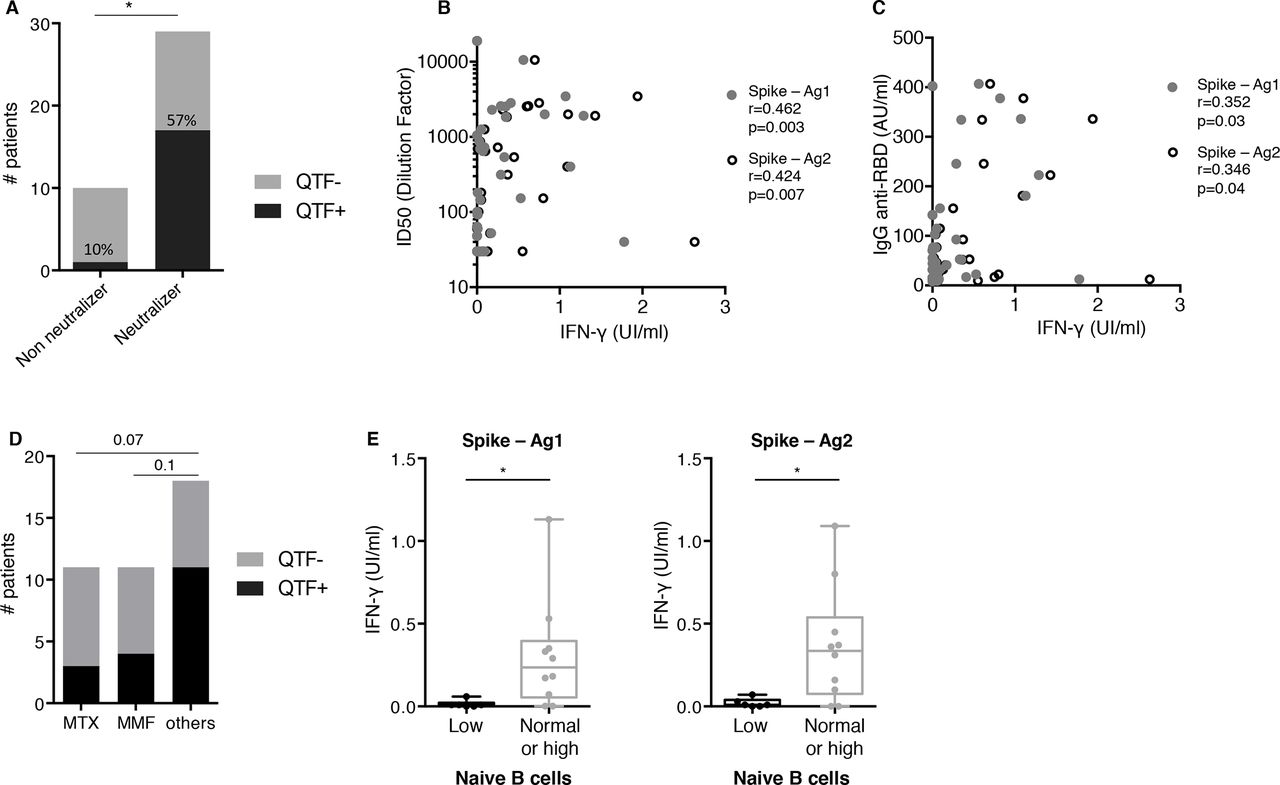
Beyond antibodies, T cell immunity is required to confer optimal immune protection. In order to gain insight into the specific SARS-CoV-2 T cell response after vaccination in patients with SLE, we evaluated IFN-γ secretion levels after specific T cell stimulation at day 15 after vaccination. While SARS-CoV-2-specific T cell responses were detected in 57% (17/30) of patients who had neutralising antibody titres, cellular responses were only detected in 10% (1/10) of patients who had non-neutralising antibody titres (p<0.05; figure 4A). Interestingly, SARS-CoV-2-specific T cell responses were nevertheless detected in two out of six patients with very low levels of neutralising activity in their serum (ID50 below 100 for D614G strain). Overall, the strength of neutralising antibody response correlates with IFN-γ production by SARS-CoV-2-specific T cells (antigen 1, r=0.462, p=0.003; antigen 2 r=0.424, p=0.007, figure 4B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
T cell responses correlate with anti-SARS-CoV-2 humoral responses. (A) Positive rates of Quantiferon SARS-CoV-2 testing in 40 patients with systemic lupus erythematosus (SLE) at day (D) 42, grouped according to serum neutraliser and non-neutraliser status, as defined in figure 3D. Numbers indicate the percentage of patients with a detectable T cell response. (B) Comparison of nterferon-γ (IFN-γ) levels (UI/mL) after specific T cell stimulation using Quantiferon SARS-CoV-2 test and serum neutralising activity reported with inhibitory dilution (ID50) in 40 patients with SLE at D45. Spearman coefficient (r) and p value (p) are indicated. MMF, mycophenolate mofetil; MTX, methotrexate.
Discussion
Here, we report BNT162b2 antibody response measured both with anti-RBD antibody levels and neutralisation activity in a cohort of 126 French patients with SLE, with both active and inactive disease. To our knowledge, this is the first evaluation of BNT162b2-induced T cell and neutralisation responses against VOCs in a cohort of patients with SLE.
Global acceptance of BNT162b2 vaccine was 80.5%, in line with previous studies.33 Most patients with SLE were followed up for a long time before vaccination in our centre and vaccine was proposed by their treating physician. Interestingly, 18 (10%) patients who first refused vaccination finally agreed to be vaccinated after a reflection time, a finding that is often lacking in COVID-19 vaccine acceptance studies. Tolerance of BNT162b2 vaccine was also good with a majority of local reactions and few systemic reactions.
SLE activity at time of vaccination, assessed either with the BILAG or the SLEDAI scores, neither reduced vaccine efficacy nor increased the risk of subsequent SLE flares or vaccine side effects. Consistent with this finding, previous meta-analysis of seasonal influenza and pneumococcal vaccinations in SLE demonstrated that immunisation had no significant effect on the SLE activity measured with SLEDAI score.34 Our results support the recommendation not to defer mRNA vaccination in patients with active SLE.1
One should note, however, that patients with active SLE would subsequently receive treatments that could blunt BNT162b2 antibody response. Indeed, MMF profoundly lowers BNT162b2 antibody response as previously reported in transplant recipients35 and patients with RMDs.5 MTX, a drug that is widely used for SLE, decreases Covid-vaccine antibody response in a similar extent to MMF. Our results confirm recent studies5 36 showing that MTX hampers immunogenicity to BNT162b2 mRNA COVID-19 vaccine in immune-mediated inflammatory diseases. However, since these two studies mixed different RMDs, the impact of these two drugs on BNT162b2 mRNA antibody response was assessed without adjusting with specific SLE parameters that could also affect BNT162b2 antibody response (disease activity, IFN-α levels). Reduced humoral responses to both seasonal influenza and pneumococcal vaccines with MTX in patients with rheumatoid arthritis (RA) have been previously reported37 38 while transitory MTX discontinuation improves the immunogenicity of seasonal influenza vaccination in patients with RA.39–42 Based on these trials, the ACR recommended that vaccination should be performed at least seven days after MTX treatment,1 but the evidence supporting this recommendation is unclear and was counterbalanced by the potential for RA flare associated with withholding MTX for a too long period, a recommendation that could not be extrapolated to SLE.
By contrast, neither hydroxychloroquine nor anti-BAFF belimumab did affect vaccine antibody response.
High-dose steroids were not associated either with a lower vaccine-induced antibody response. The median prednisone daily high dose was 19 mg in our study, a threshold that is lower than the one used for transplant recipient patients.43 There is still controversy regarding the effect of steroids on SARS-CoV-2 vaccine efficacy, in particular whether a daily dose prednisone threshold above which antibody response might be blunted could be defined.1 As a consequence, there is currently no expert panel recommendation to delay or not COVID-19 vaccination in patients with RMD receiving glucocorticoids at a prednisone-equivalent dose of ≥20 mg/day.1 Optimal antibody responses seem to be elicited in RMDs patients on glucocorticoid monotherapy,44 although the daily prednisone dose was not reported in the latter study. Our data suggest that patients with SLE with a daily dose of prednisone close to 20 mg should properly respond to BNT162b2 vaccine.
Elevated IFN-α serum levels were not associated with impaired BNT162b2 antibody response, an observation in line with the lack of influence of SLE activity on vaccine efficacy. By contrast, elevated baseline total serum IgG levels were associated with a better antibody response. This association remains significant (p=0.018) when the analysis is adjusted for immunosuppressive drugs that could decrease IgG levels. For patients with chronic lymphocytic leukaemia, higher serum immunoglobulin levels at time of BNT162b2 mRNA vaccination were independently associated with a better response rate (IgG levels ≥550 mg/dL (OR 3.70, 95% CI 1.08 to 12.66)).45 IgM levels were also an independently associated with serologic response (IgM ≥40 mg/dL (OR 2.92, 95% CI 1.21 to 7.02)) in these patients. The influence of baseline IgG and IgM levels on COVID-19 vaccine antibody response has never been reported before in RMD and might be considered in future studies.
Our data also underline the importance of interrogating initial B cell compartments as correlates of predicted vaccine response. A marked decrease of naïve B cells is known to be characteristic of SLE and not only the result of immunosuppressive drugs.46 47 Here, we observed a strong correlation of naïve B cell loss with poor vaccine antibody response, which likely points the role of naïve B cells as a source of spike reactive B cells. In recent studies, extensive screening of pre-pandemic naïve B cell repertoires revealed the presence of SARS-CoV-2-neutralising antibody precursors. This subset of germline antibodies bound SARS-CoV-2 ACE2 RBD, although weakly, and may be engaged on vaccine exposure to generate germinal centres and then follow affinity maturation process.48 49 Indeed, Rincon-Arevalo et al observed a significant difference in the frequency of SARS-CoV-2 RBD-specific naïve B cells between BNT162b2 responders and non-responders.50 Reduced naïve B cell pool in SLE would thus readily impact precursor frequency available to encounter the antigen, therefore impairing vaccine efficiency. Future vaccination strategies in SLE should consider naïve B cells as an essential biomarker to define individuals at high risk of suboptimal response that might benefit from reinforced vaccine regimens.
It will remain to define in future studies whether patients eventually seroconverting after a third dose would have had readily detectable T cell responses after the second dose. Finally, much larger studies will be necessary to determine whether BNT162b2-induced T cell responses are solely sufficient to prevent at least from severe forms of the COVID-19 in patients.
Our study has some limitations. It is surprising to note that SARS-CoV-2-specific T cell responses were detected in only 57% of patients who had neutralising antibody titres. This observation questions the sensitivity of the quantiferon (QTF) assay used in our study and another.51 Future studies should include other assays such as T cell ELISPOT52 to confirm this observation and whether low T cell responses would be more likely associated with SLE, compared with other RMDs and to healthy controls. Moreover, QTF assay was performed 15 days after the second dose, a timing that may be too short to optimally detect SARS-CoV-2-specific T cell response. Longitudinal studies are thus required to determine whether patients with SLE develop a delayed cellular immune response.
Unlike previous authors,3–5 we did not use antibody response positivity thresholds. There are, however, no studies showing that these thresholds give patients with RMD real protection against the risk of subsequent infection with SARS-CoV-2. It is not yet clear as to what immunogenicity parameter is predictive of vaccine-induced protection. Additionally, these thresholds vary according to the assays used and the variants studied, their clinical relevance is therefore questionable. To address this issue, Khoury et al 53 recently analysed the relationship between in vitro neutralisation levels and the observed protection from SARS-CoV-2 infection using data from seven current vaccines and from convalescent cohorts. These authors found that despite expected inconsistencies between studies, comparison of normalised neutralisation levels and vaccine efficacy demonstrates a remarkably strong non-linear relationship between mean neutralisation level and the reported protection across different vaccines (Spearman r=0.905; p=0.0046). In this setting, the strong correlation we observed between RBD antibody levels and the neutralising activity is reassuring about the usefulness of serology in clinical practice. In our survey, only 1 out of 126 patients presented high IgG anti-RBD levels and low neutralising activity (figure 3A). Antibody response was assessed 14 days after the second injection. We cannot rule out the hypothesis that a higher antibody response would have been observed later.44 Of note, Polack et al measured antibody responses as soon as 7 days after second injection21 and were able to link BNT162b2 efficacy to prevention of SARS-CoV-2 infections in healthy individuals. Lastly, this SLE cohort did not comprise rituximab-treated patients, in whom antibody responses are abrogated.54 Rituximab is not approved for SLE, although it is being used in clinical practice.
Despite its limitations, this study provides evidence that in SLE, use of MMF or MTX is associated with reduced vaccine efficacy. We also show that low baseline IgG levels and a reduced pool of naïve B cells are predictive of impaired vaccination-induced neutralising activity against SARS-CoV-2. These parameters could be helpful for physicians to delineate which patients should have antibody measurement after full BNT162b2 vaccination and should be proposed a third injection of BNT162b2 vaccine.
Supplemental material
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Ethics approval
The study protocol was approved by the Comité d’Ethique Sorbonne Université (CER-2021-011).
Acknowledgments
The authors wish to thank the patients who agreed to participate in this study, nurses from the Internal Medicine Department of Institut E3M (Assistance Publique Hôpitaux de Paris (AP-HP), Hôpital Pitié-Salpêtrière, 75013 Paris, France) who participated in this study, all members from the Immunology Department, (Assistance Publique Hôpitaux de Paris (AP-HP), Hôpital Pitié-Salpêtrière, 75 013 Paris, France), who performed Quantiferon analysis and B-cell phenotyping, Laura Wakselman from clinical research unit (URC) of Pitié-Salpêtrière Hospital for helping with regulatory and ethical issues.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Twitter @michelinepha
QM, DS, MM, FA, GG and ZA contributed equally.
Contributors QM, AM, RL, FA, JH, MP, LB and ZA recruited patients. QM, PB, HC, PMF and PG-D collected demographic and clinico-biological data. MM, DS and PG-D prepared the specimens. MM, QM, FA and DS designed and performed experiments. QM, DS, FA, MM, SdA and SM analysed data. QM and DS prepared the figures. QM, DS, GG and ZA wrote the manuscript. QM, DS, FA, MM, GG and ZA designed the study and reviewed the manuscript.
QM, DS, MM and FA contributed equally to this work.
GG and ZA jointly directed this work.
Funding The study was supported by the Agence Nationale de la Recherche (ANR Flash COVID19 program, MUCOVID, PI: DS) and by the SARS-CoV-2 Program of the Faculty of Medicine from Sorbonne University ICOViD programs, PI: GG).
Competing interests ZA has received research grants from Amgen, AstraZeneca, GSK and Roche; fees for consultancy from AstraZeneca, GSK and Kezar. MM received consulting fees from Genalyte Inc. 3 years ago. Other authors declare that they have no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.