Article Text

Statistics from Altmetric.com
Over the last decade, the application of new therapeutic strategies and the availability of newer molecules have ‘raised the bar’ regarding goals and expectations for systemic lupus erythematosus (SLE) management, and there is now consensus that disease remission should be the ultimate goal when treating patients with SLE, while low disease activity (LDA) could be considered a suitable alternative outcome only when remission cannot be achieved,1 typically in patients with refractory disease.
It has to be pointed out that experts consider very important to have a unified definition of remission and LDA in order to be able to compare the results of different studies. This is the reason why a considerable effort in establishing an agreed-upon definition of remission and LDA has been shared among researchers in the last few years.2–4 In 2015, the Definitions Of Remission In SLE (DORIS) Task Force has been set up, and in 2021, the DORIS definition of remission has been published.5 Clinical remission in SLE can be conceptualised as the absence of clinical manifestations or urinary or haematological abnormalities due to active immune pathways. The concept underlying such definition is that patients in a sustained state of remission would not experience pathological consequences of the disease over time. In the same years, the Asia Pacific Collaboration group proposed and validated the lupus low disease activity state (LLDAS) definition.6 Since then, a huge amount of data regarding prevalence, durability, and protective effect of remission and LLDAS on disease outcomes such as damage, quality of life and flare rate has been accrued.7–13 These studies validated the definitions of DORIS remission and LLDAS worldwide.
Nevertheless, there are setting in which the application of these definitions is not possible. This is the case of the study by Ugarte-Gil et al,14 carried out in the SLICC cohort, where data on physician global assessment (PGA) were lacking. What should researchers have done in this case? Give up and not evaluate this topic in their cohort? The authors decided to use an alternative definition of remission, namely the one proposed by Zen et al (Padua definition), which was already validated in different settings,11 12 15 and to modify the LLDAS definition by excluding PGA. Does this choice limit the relevance of their results? The paper by Ugarte-Gil et al suggests that, despite the great effort made by the DORIS Task Force and the good performance of the LLDAS, it is unlikely that a single definition of remission (the DORIS) and LDA (the LLDAS) will be used all over in the next years. Although debatable, the blossoming of a number of definitions of remission and LDA for SLE is not an unusual finding, resembling other diseases, including rheumatoid arthritis (RA), where a number of definitions of remission and LDA exist and are currently used.16
The results presented by Ugarte-Gil et al 14 also enforce the long and controversial debate regarding the importance of including PGA in the definition of remission and LDA. PGA is generally regarded as the gold standard for evaluating disease activity in SLE. However, PGA has a substantial inter-rater variability partly related to variations among rheumatologists in weighing different organ manifestations and serological activity.17 In addition, the PGA International Standardisation Consensus in SLE study has recently demonstrated a major need for both standardisation and training in the scoring of PGA, suggesting that only expert physicians can efficiently rate the PGA, and it should be preferably scored by the same rater at each visit, making its use particularly challenging in multicentre and longitudinal studies.18 It has also to be pointed out that in a multicentre study evaluating different definitions of remission, the addition of PGA to clinical SLE Disease Activity Index 2000 (SLEDAI-2K) did not increase the performance of SLEDAI-2K in predicting damage accrual,19 and no studies ever evaluated the correlation between PGA and damage accrual, according to a recent review.17 Thus, since the choice of a target for treatment should be based on the interpretation of measures that are potential predictors of a bad outcome, PGA seems not essential in defining remission and LDA in SLE.
One strength of the DORIS remission and the LLDAS is the inclusion of a therapeutic item in their definition, unlike what was done in RA. In particular, the inclusion of a cut-off of glucocorticoid (GC) dose is very reasonable, as higher doses of GCs can disguise an active disease.
However, the treat-to-target (T2T) approach in SLE has to be considered a stepwise process where the first step should be the achievement of clinical remission, or clinical LDA, both meant as control of disease activity irrespective of the treatment (GCs, immunosuppressants, biologics) at least in the short term,20 since the first driver of damage and poor outcome still remains the disease activity itself. As a second step, the decrease in GC dosage and even their withdrawal should be always attempted. In this regard, it is worthy to note that a significant heterogeneity in GC administration across different cohorts has been observed,21 also in the management of patients in clinical remission or LDA.
Notably, the study by Ugarte-Gil et al 14 highlights that the feasibility of achieving and maintaining the targets—remission or LLDAS—not only depends on the definition used, but also on genetic, geographical and socioeconomic factors of the population(s) studied (figure 1). Ethnicity influences SLE outcomes, having Caucasians a better prognosis compared with Afro-Caribbeans and Asians; a low socioeconomic status is associated with worse SLE damage, greater mortality and poorer quality of life.22 In addition, the type of healthcare system and its financial resources might highly affect the availability of therapeutic options, in particular more expensive drugs, and the access to care, thus influencing the probability of achieving the targets. In RA, it was shown that the macroeconomic environment is an important determinant of the access to biological disease-modifying antirheumatic drugs. The limited use of biologics was attributed to a low/difficult access to specialists and the cost of biologics, which contributes to restrictive guidelines for their use and administrative constraints, most likely related to the gross domestic product in each country,23 but also to the type of healthcare regimen.24 A review on the healthcare quality in SLE carried out in USA showed that access to care, health insurance, and financial and organisational arrangements of the health system represent relevant determinants of different disease outcomes in SLE, including disease activity and damage.25 The fact that the Italian National Health Service provides free and equal access for all citizens to all healthcare services, including primary, hospital and emergency care, as well as visits, diagnostic procedures and therapies, including biologics and other innovative drugs, might have contributed to the high attainment of remission observed in Padua Lupus cohort2 7 12 and in other Italian studies.15 19 26 Thus, these observations suggest that not only disease phenotypes but also geographic and socioeconomic factors might drive the choice of the most reasonable and appropriate target in different populations. Accordingly, different settings could require diverse definitions of remission and LDA.
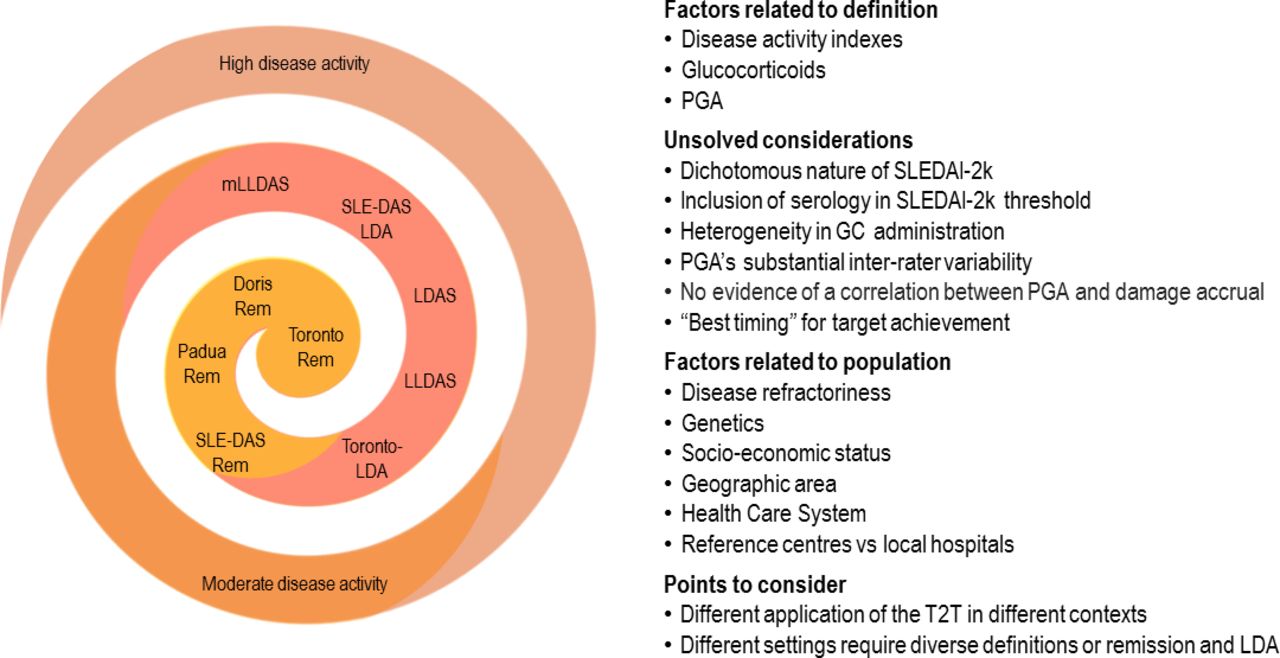
{kind=link}
Factors influencing the attainment of the T2T goals remission and LDA. Toronto rem, Toronto lupus Cohort definition of remission, Polachek et al. 3; DORIS rem, DORIS definition of remission, van Vollenhoven et al. 5; Padua rem, Padua lupus Cohort definition of remission, Zen et al.2 12; SLE-DAS rem, SLE-DAS definition of remission, Jesus et al.33; Toronto-LDA, Toronto lupus Cohort definition of LDA, Polachek et al.3; LLDAS, lupus low disease activity state, Franklyn et al.6; LDAS, low disease activity status, Ugarte-Gil et al 4; SLE-DAS LDA, SLE-DAS definition of low disease activity, Assunção et al.34; mLLDAS, modified LLDAS, Ugarte-Gil et al.14 GC, glucocorticoid; LDA, low disease activity; PGA, physician global assessment; SLEDAI-2K, Systemic Lupus Erythematosus Disease Activity Index 2000; T2T, treat-to-target.
Another aspect that emerges as a possible driver of unbalanced outcomes in multicentre studies is the different application of the T2T in different contexts. In reference rheumatology centres, the strategy of treating to the target—remission whenever possible, LDA in refractory patients—with treatment adjustments until the target is reached and maintained, using antimalarials in all patients who tolerate them, immunosuppressants if needed, with the possibility of an early use of biologics, aiming at the lowest doses of GCs, is already a reality. Thus, it is hard to set up a clinical trial investigating T2T as opposed to a standard approach only aimed at symptomatic control, which would lead to an ethically unacceptable undertreatment. Where the T2T strategy still needs to be implemented is in local hospitals, which are often those with economic restrictions and/or without lupus clinics. In addition, we are looking forward to seeing the results of the randomised ‘LUPUS-BEST’ trial for the application of the tight control T2T approach, with a glimpse on overtreatment-related drawbacks.27 An important issue would also be to understand whether there is a ‘best timing’ for the achievement of the target in different SLE manifestations, similarly to what has already been demonstrated in lupus nephritis,28 which could guide the intensity, escalation, and de-escalation of treatment, and how to better define ‘refractory’ SLE.
Besides these considerations, the heterogeneity among disease manifestations makes the definition of LDA challenging, and we wonder whether the LLDAS or the LDA-Toronto Clinic definition3 really capture all patients in LDA. In clinical practice, we consider our patients in LDA when they have mild clinical manifestations or mild urinary or haematological abnormalities. The entity of these manifestations should be as ‘mild’ as they are acceptable in terms of residual damage progression they can be responsible for. Indeed, the choice to settle for LDA is based on the balance between the residual disease activity and the increase in therapy, which would be required to completely abolish disease activity in that particular patient. Serology has relatively little value in the definition of disease activity and remission, as well as in driving therapy; thus, to include serology in the definition of LDA is questionable.
Defined as such, clinical LDA is not frequently observed in patients with SLE. LDA can be transiently present in the relapsing-remitting pattern of disease activity, in the phases of transition from remission to disease activity and vice versa, or in cases of chronic active disease with mild manifestations, the less frequent pattern of SLE.29 30 Thus, the high prevalence of LDA reported in different cohorts using the LLDAS definition is related to the inclusion of patients in remission within the LDA group. The overlap between LLDAS and remission was reported in several studies, and was confirmed by the study of Ugarte-Gil et al.14 Recently, in a prospective cohort study carried out in 1707 patients from 13 international centres, LLDAS overlapped with the 2021 DORIS definition of remission in 75% of total visits, meaning that only 25% of visits represented patients in LLDAS but not in remission.31
Another issue is that not all patients in LDA can be captured by LLDAS. In fact, the definition of LLDAS excludes patients with major organ system involvement, including renal, cardiopulmonary, central nervous system, vasculitis, fever, haemolytic anaemia and gastrointestinal activity. Thus, through the LLDAS, one should exclude the possibility of LDA in renal, serosal and vasculitic domains. Moreover, since the threshold of the SLEDAI-2k in LLDAS has been set at four points including serology, patients with mild arthritis (four points in the SLEDAI-2k) or skin manifestations (two points) but with positive serology are precluded from being classified as in LDA by the LLDAS. This means that LLDAS can also miss patients with mild skin and joint disease.
As LDA suffers from a lack of defined borders discriminating it from remission, some effort is still needed to clearly depict what LDA is in lupus, including its definition and prevalence. A new measure of disease activity, the SLE disease activity score, has been proposed to overcome these limitations, related to the dichotomous nature of the SLEDAI-2k,32 with cut-offs for remission33 and LDA also derived and validated.34 It would be interesting to see its performance in capturing patients with clinical LDA in different cohorts.
In conclusion, the identification of beneficial targets, such as remission and LDA, represents an important step in the application of the T2T strategy in SLE, with the ultimate goal of decreasing damage progression and improving quality of life.35 The application of a unified definition of remission and LDA would be ideal to directly compare results from different cohorts as well as from randomised control trials for new drugs in the research setting; however, in clinical practice, different definitions could suit better diverse patient cohorts, taking into account variation in ethnicity, demographics and access to care, which might impact on T2T applicability.
Ethics statements
Patient consent for publication
References
Footnotes
Handling editor Josef S Smolen
Contributors MZ, MG and AD were involved in drafting the article and revising it critically for important intellectual content; all authors approved the final version to be submitted for publication and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.