Article Text

Abstract
Background: Elderly rheumatoid arthritis (RA) patients are generally at increased risk of serious infections (SI). At the same time, treatment with bDMARDs has been associated with a higher SI risk than treatment with csDMARDs (1). However, long-term use of bDMARDs did not increase the risk of SI in a small group of elderly patients over 65 (2). The extent to which elderly patients are exposed to a higher SI risk when treated with JAK inhibitors (JAKi) is an open question.
Objectives: To assess the effects of bDMARDs and specifically JAKi on the risk of SI in elderly patients with RA.
Methods: The German register RABBIT is a prospective, longitudinally followed cohort of RA patients enrolled with a new start of a DMARD after at least one csDMARD failure. This analysis comprises patients over 70 years of age who were enrolled between 01/2007 and 04/2020 and had at least one follow-up.
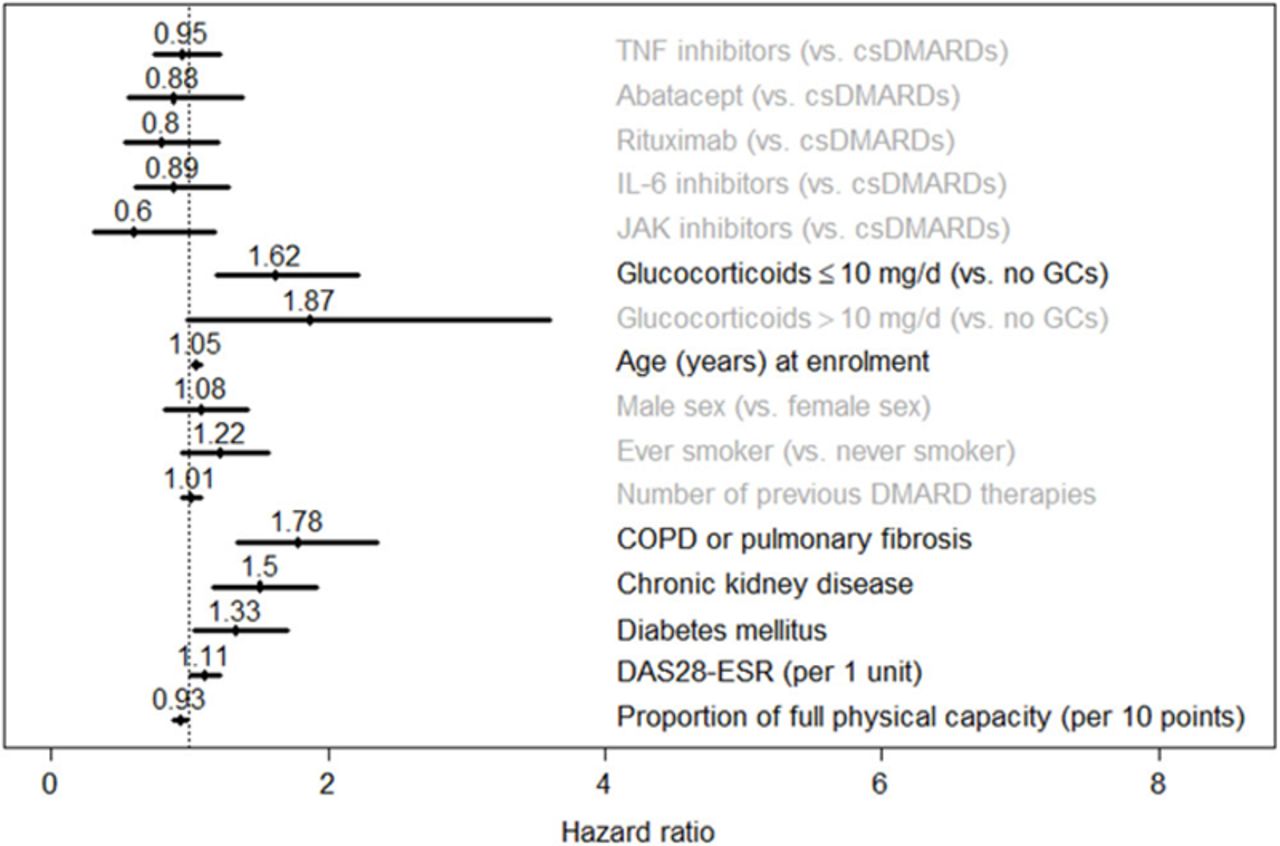
Results: Of 13,491 patients followed-up in RABBIT, 2274 with an age > 70 years were included in the analysis. 626 SI were observed in 425 of these patients. Baseline characteristics at start of the respective DMARD are shown in Table 1. In most characteristics, patients on JAKi were more comparable to patients under bDMARDs than to those on csDMARDs. JAKi patients received glucocorticoids (GC) less frequently than patients on other treatments. The HR for SI was lower than 1 in patients receiving bDMARDs or JAKi compared to csDMARDs, but without statistical significance (Figure 1). GC use (HR 1.6, 95% CI: 1.2 – 2.2 for ≤ 10 mg/d), higher DAS28-ESR values (HR 1.1, 95% CI: 1.0 – 1.2 per 1 point increase), COPD or pulmonary fibrosis (HR 1. 8, 95% CI: 1.3 – 2.4), chronic kidney disease (HR 1.5, 95% CI: 1.2 – 1.9) and diabetes mellitus (HR 1.3, 95% CI: 1.0 – 1.7) were associated with an increased risk of SI. Better physical capacity was associated with a decreased risk of SI (HR 0.9, 95% CI: 0.88 – 0.98 for a 10 point increase).
Patient characteristics by treatment at baseline
{kind=link}
Hazard ratios for serious infections with 95% confidence intervals
Conclusion: Treatment with JAKi as well as treatment with bDMARDs was not associated with an increased risk of SI in elderly patients above 70 years of age. Key comorbidities such as diabetes mellitus, chronic pulmonary and kidney diseases were associated with increased risk, as was concomitant GC use and higher disease activity.
References: [1] Listing J et al., Rheumatology 2013; 52 (1): 53-61.
[2] Kawashima H. et al., Rheum. Intern. 2017; 37: 369-376.
Acknowledgements: RABBIT is supported by a joint, unconditional grant from AbbVie, Amgen, BMS, Celltrion, Fresenius-Kabi, Gilead, Hexal, Lilly, MSD, Pfizer, Roche, Samsung Bioepis, Sanofi-Aventis, UCB, and Viatris.
Disclosure of Interests: None declared